Archive
Data show a recent decline in the developmentally disabled population in state-run residential care
Data provided by the Baker administration show that the number of residents in remaining state-run residential programs for the developmentally disabled has begun to decline, raising questions about the state’s policy for the future of state-run services.
The data, which were provided under a Public Records Law request, indicate that the previous fiscal year (2016) may have been the peak year for the residential population in state-operated group homes and the Wrentham and Hogan developmental centers.
The graph below, which is based on the DDS data, shows the number of residents living in state-operated group homes each year since Fiscal Year 2008:

As we have frequently pointed out, the administration appears to have placed a priority on funding privatized residential services offered by corporate providers to the Department of Developmental Services. A question remains, however, as to whether the administration’s policy also entails phasing out state-operated care.
While Governor Baker’s Fiscal 2018 budget proposes $59.9 million in additional funding for privatized group homes, his budget proposes a $1.8 million cut in the state-operated group home account. That would amount to a $6.9 million cut in that account when adjusted for inflation.
Similarly, the governor is proposing a $2.4 million cut in the state-run developmental centers line item. That’s a $4.9 million cut when adjusted for inflation.
DDS operates or manages both state-run and privatized systems of residential care in Massachusetts. The state-run system, which is now much smaller than the privatized system, includes the two remaining developmental centers and the state-operated group homes.
The ultimate elimination of state-run residential services would take away a key element of choice for individuals and families in the DDS system. State-run residential centers and group homes provide residential care to some of the most profoundly disabled persons in the commonwealth, and they tend to employ staff with higher levels of training and lower rates of turnover than do corporate-run facilities.
COFAR has sent a follow-up Public Records request to DDS, seeking any policy documents that concern the future of state-operated care in Massachusetts.
The administration of then Governor Deval Patrick began closing the remaining developmental centers in Massachusetts in Fiscal 2008, reducing the number of those federally overseen facilities from six to two. Most of the residents in the now-closed developmental centers were transferred either to the Wrentham center or to state-operated group homes, leading to an initial surge in the residential populations in those facilities. But those residential population numbers now appear to be dropping.
According to the DDS data, the number of residents in state-operated group homes rose from just over 1,000 in 2008, when four of the six developmental centers were targeted for closure, to roughly 1,150 in Fiscal 2016. As of the current fiscal year, that number had dropped to about 1,130.
As the graph below shows, both a population surge and drop-off have also occurred at the Wrentham Developmental Center since Fiscal 2008:

The DDS data appear to provide further confirmation of COFAR’s contention that state-run residential facilities are not being offered as residential choices to persons waiting for residential care in the DDS system. We believe that if those facilities were routinely offered as choices, the number of residents in them would either continue to rise or remain steady, but would not be declining.
If DDS is failing to offer state-run group homes and developmental centers as options to people waiting for residential care, that situation would appear to be in violation of federal laws, which require that all available services be offered as options.
The Home and Community Based waiver of the Medicaid Law (42 U.S.C., Section 1396), requires that intellectually disabled individuals and their guardians be informed of the available “feasible alternatives” for care. In addition, the federal Rehabilitation Act (29 U.S.C., Section 794) states that no disabled person may be excluded or denied benefits from any program receiving federal funding.
We think the DDS data closely track the closures of the Fernald, Monson, and Glavin developmental centers, starting in Fiscal 2008, and the transfer of the residents of those facilities primarily to the state-operated group homes and the Wrentham center.
But as we reported in 2014, while 49 new state-operated group homes were built between 2008 and 2014, 28 state-operated homes were closed during that period. The new state-operated homes appear to have been intended to accommodate only the residents of the homes that were being closed and the residents transferred from the developmental centers.
Nevertheless, an undisclosed number of disabled individuals are reportedly waiting for residential services in Massachusetts, although the state does not maintain an official waiting list that would publicly identify the number of people waiting. The Massachusetts Developmental Disabilities Council has continued to cite a 2010 survey indicating that some 600 people were waiting for residential services in the state, and up to 3,000 people were waiting for family support services.
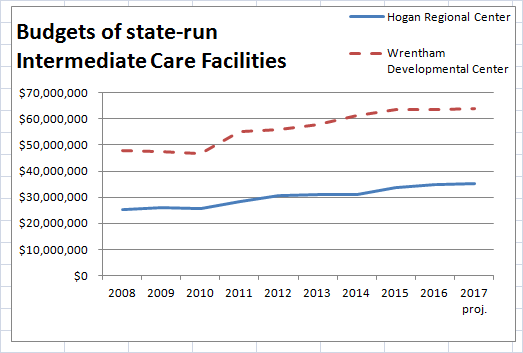
As noted, the administration appears to be attempting to meet the demand for residential care by boosting funding to corporate residential providers. While that hasn’t prevented the budgets of state-run developmental centers from increasing, those budgets may be leveling off.
The DDS data, which includes information about the Wrentham and Hogan developmental center budgets, shows increases in those budgets between Fiscal 2008 and 2015. Wrentham’s budget, in particular, appears to have leveled off, starting in Fiscal 2015.
It is unclear if or when the administration intends to phase out state-run DDS residential care, but the initial data are cause for concern. If you have a loved one in a state-run facility or are seeking care in a state-run setting, please let your local legislators know about this situation.
You can find your legislators at this link.
Harvard researcher looks for the key to understanding the link between Down syndrome and Alzheimer’s disease
The link between Down syndrome and Alzheimer’s disease has become the subject of increasing scientific interest, and a major new study is seeking to shed further light on that connection.
Dr. Florence Lai of Harvard University, McLean Hospital in Belmont, and Massachusetts General Hospital, is the lead Massachusetts investigator in a multi-center, five-year study funded by the National Institutes of Health.

Dr. Florence Lai
In an interview with COFAR, Dr. Lai said the study is seeking “biomarkers” that may predict the onset of Alzheimer’s disease and enable researchers to learn more about Down syndrome. It is intended to be “the most comprehensive study of the links between Down syndrome and Alzheimer’s disease up to this point.”
Lai and her colleagues, Dr. Diana Rosas, a neurologist, and Dr. Margaret Pulsifer, a psychologist, are in charge of the Massachusetts portion of the study.
While the average person with Down syndrome develops symptoms of Alzheimer’s disease in their early 50’s, some may not develop the dementia until the age of 70, and a very few escape it altogether.
“The study seeks, among other things, to learn the reasons for that variation,” Dr. Lai said.
The Massachusetts General Hospital’s facility at the Charlestown Navy Yard is one of seven sites around the country and England that are coordinating their research efforts as part of the study. The other sites include Columbia University (New York City), the University of California Irvine, the University of Pittsburgh, Cambridge University (UK), the University of Arizona (Phoenix), and the University of Wisconsin (Madison).
The NIH study represents a natural progression in Dr. Lai’s clinical practice and research. Over several decades, she has evaluated and followed some 750 individuals with Down syndrome, including Joanna Bezubka, a cousin of COFAR Board member and former president, George Mavridis. In 2013, Mavridis published a compelling memoir about his experience in caring for Joanna, who died of Alzheimer’s disease in 2012 at the age of 60.

George Mavridis and Joanna Bezubka on Joanna’s 60th birthday. Joanna, who had Down Syndrome, died in 2012 at the age of 60 of Alzheimer’s Disease. She had been one of Dr. Lai’s clinical patients.
In a recent letter to Mavridis, Lai said that her hunch that women with Down syndrome who developed menopause early were more likely to develop Alzheimer’s disease earlier, led to an earlier multi-year NIH study by a colleague who proved the hypothesis.
Another hunch of hers that immunological factors in Down syndrome might be involved in Alzheimer’s disease is now the subject of intense scientific interest with many researchers concentrating on neuro-inflammation as a causative factor.
Those avenues of inquiry “may pave the way to think outside the box for potential treatments for AD (Alzheimer’s disease),” Lai wrote to Mavridis.
In her interview with COFAR, Dr. Lai said scientists have discovered that people with Down syndrome are genetically predisposed to create large concentrations in their brains of amyloid protein, which is connected with destruction of brain cells in Alzheimer’s disease.
The gene for the precursor of amyloid protein is located on Chromosome 21. Since people with Down syndrome have an extra copy of Chromosome 21, Dr. Lai explained, they “make the amyloid earlier and more of it. That may be the reason for the high incidence of Alzheimer’s disease in people with Down syndrome.”
In order to learn more about the impact of the amyloid protein and other potential biomarkers of Alzheimer disease, the NIH study is designed to collect a broad range of information from the participants in the study, including information on their health history, cognitive functioning, immune and genetic factors, and daily living activities. The information is obtained from cognitive testing, from blood samples that are sent to specialized labs around the country, and from caregivers of the participants.
The study also includes an MRI brain scan of the subjects and an optional PET scan (Positron Emission Tomography), which involves the introduction of a small dose of radioactive material to examine the presence of amyloid protein in the brain. Another optional part of the study includes analyzing the cerebral spinal fluid obtained from a spinal tap.
The 3-year NIH study is limited to adults over the age of 40 with Down Syndrome at three of the sites (including Charlestown) and over age 25 at the other four sites. At the MGH Charlestown site, the study involves three cycles of visits with each cycle involving two to three visits of up to five hours each. The second and third cycles each take place 16 months after the previous cycle.
Although the study was initially funded in September 2015, it took about a year to “harmonize the procedures at all the sites,” Dr. Lai said, and to receive the necessary approvals from the participating institutions including the Research Review Committee of the Department of Developmental Services in the case of Massachusetts. Lai said the researchers at the seven study sites hope to recruit up to 700 individuals to participate in the study.
Lai said that although the NIH authorized the multi-million dollar study in 2015, the federal agency recently announced that it will be forced to cut some of the funding. She noted that the study is expensive to perform. A large number of specialized personnel is needed, and doing the brain scans is “very costly.”
At the MGH site, about 20 participants have been recruited so far and have been through a preliminary visit, Lai said. They receive a modest payment for their participation. The information collected is anonymous, she said. Even the researchers analyze only coded, aggregate data.
Continuing to treat Down Syndrome patients
Apart from the NIH study, Drs. Lai and Rosas continue to clinically treat, test, and follow the life histories of patients with Down syndrome at McLean hospital. They see each patient once a year and generate neurological evaluations which are shared with caregivers and family.
Lai has collected hundreds of blood samples, some of which have been stored at a Harvard-affiliated facility at -80 degrees C. However, the samples have lain dormant for many years due to a lack of funding needed to analyze them. Lai noted that many of her colleagues have experienced the same funding frustrations, and have had to supplement federal funding with industry grants and philanthropic donations.
It was actually due to the generosity of several families of her patients, Lai said, that she herself was able to start a Down Syndrome Fund for Alzheimer Research at MGH. The Fund got a boost of several thousand dollars a few years ago when a member of the MGH Board of Directors called Lai to thank her for her care of a patient with Down syndrome whom he knew personally.
Lai said that if the Down Syndrome Fund ever does get more sizeable contributions, her “dream” is to team up with colleagues to fully analyze the stored blood samples, and “to encourage a younger generation of clinicians and investigators to devote their energies to care for and study those with Down syndrome.”
Persons interested in learning more about the NIH study at MGH can call 617-726-9045 or 617-724-2227.
Those interested in an evaluation and follow-up with Drs. Lai and Rosas at the McLean Hospital Aging and Developmental Disabilities Clinic can call 617-855-2354.
