Archive
DDS license staff didn’t appear to notice problems mounting for resident at group home
Timothy Cheeks is a 41-year-old man with Down syndrome who lives in East Longmeadow in a group home managed by the Center for Human Development (CHD), a corporate provider to the Department of Developmental Services.
Since 2017, Tim’s foster mother and co-guardian, Mary Phaneuf, has dealt with a string of problems with Tim’s care at the residence including:
- A lack of proper medical care for Tim, including no documented visits to a primary care physician or dentist for seven years;
- No documented visits to a cardiologist for six years despite Tim’s having been born with a congenital heart defect;
- A failure to treat Tim for two years for back pain and a degenerative back problem, and to fill a prescription for pain medication for him;
- A failure to ensure that Tim was receiving Social Security benefits for at least two years;
- The unexplained removal of Tim from his day program run by the Work Opportunity Center (WOC) in Agawam without informing Mary of that fact; and
- The diversion of food stamp benefits for Tim and at least one other resident of a CHD group home
Despite the seriousness of those issues, an online June 2017 DDS licensure inspection report for CHD on the department’s website does not mention those or similar problems in the agency’s group homes. The licensure report recommended deferring a new two-year license for CHD, but for generally worded reasons such as “medication treatments plans must address all required elements,” and “individuals’ funds and expenditures must be fully tracked.”
There was no indication on the DDS provider licensure report website whether a recommended follow-up review of the provider occurred or what the result was.
COFAR has reached out to DDS and CHD for comment. In an email sent this past Tuesday (July 9) to DDS Commissioner Jane Ryder, I asked whether DDS’s licensure staff takes abuse complaints and investigations into account in drafting licensure reports concerning providers.
In a separate email the same day to CHD President and CEO James Goodwin, I asked whether Goodwin believes his agency has sufficient policies and practices in place to prevent the types of problems Mary Phaneuf is alleging or whether such policies and practices are needed. I also asked whether CHD has policies both to ensure communication with family members and guardians who raise concerns about care, and to ensure that action will be taken to address those concerns.
To date, I have not heard back either from Commissioner Ryder or from Goodwin.

Tim Cheeks with his foster sister Nicole Phaneuf Sweeney
Based on email correspondence between Mary Phaneuf and the former CHD manager of Tim’s group home, it appears that his East Longmeadow residence was inspected in 2017 as part of a two-year, DDS licensure process.
In June, DDS issued a resolution letter in response to a complaint filed by Mary with the Disabled Persons Protection Commission (DPPC). The complaint alleged that Tim had been neglected medically and that his SSI had improperly been allowed to lapse.
The DDS resolution letter also concerned a separate complaint filed by an anonymous reporter that the then house manager had misappropriated food stamp benefits for Tim and another resident.
The DDS resolution letter asked CHD to provide an accounting of Tim’s health care and that of the other resident for the past four years as well as an accounting for $2,000 in food stamp benefits that were allegedly taken from Tim and the other resident.
The DPPC had referred Mary’s complaint to DDS and apparently referred the complaint about the food stamps to the Hampden County District Attorney.
The DDS resolution letter did not dispute any of the problems Mary raised, but said an investigator had concluded that none of the problems constituted a risk of serious harm to Tim. Mary disagrees with that assessment, and has filed an appeal of the resolution letter.
Mary said she wants the public to know about the ongoing issues with her son’s care, and about her frustration in getting DDS and the provider to react to them and provide her with answers to her questions. She would like to see her information investigated by the state Attorney General’s Office, which COFAR has previously reached out to in an effort to persuade the AG to focus on care in the DDS private provider system.
Family had implicitly trusted the system
Mary said that prior to 2017, when she discovered by accident that Tim had been removed without her knowledge from his day program by the then manager of his group home, she had implicitly trusted the system. She thought, for instance, that the group home staff was regularly taking him to doctors’ appointments, particularly given that such visits were part of his care plan or Individual Support Plan (ISP).
When she found out, however, that he had been removed from his day program, she began to question everything the provider staff did or said. She was later to discover, for instance, that while Tim’s 2018 ISP stated that he had been to a dentist in September of that year and a doctor in October, CHD was unable to provide any documentation to back up those claimed visits. She now doubts that many, if any, of those visits actually occurred.
Adopted as a foster child
Tim first came to live with Mary and her family in 1981 as a foster child when he was three years old. At 22, when he became eligible for DDS services, he moved into a group home, and Mary became his co-guardian along with Tim’s birth mother. However, Tim’s birth mother has not been in contact with him, and Mary said she was told by DDS that the birth mother subsequently resigned as co-guardian.
Last year, one of Mary’s daughters, Jessica Szczepanek, became Tim’s health care proxy. Mary would like to make Jessica Tim’s co-guardian.
A 2017 DDS licensure report for CHD describes the provider as “a large, multifaceted organization,” and states that CHD operates throughout western Massachusetts as well as Connecticut.
Untreated back pain
Mary said Tim has complained of severe back pain since 2017; but after being assured by the then CHD house manager that he had been seen by a doctor who suggested it was just a posture problem, Mary discovered that he was sleeping on a “very old” futon mattress without a box spring to support it.
Additionally, she said, she discovered that he was sleeping several nights per week at another CHD residence in Wilbraham, on the Springfield line, where he had to sleep on a couch or the floor. She said she requested that CHD provide him with a proper mattress and box spring, and either purchase a bed for him at the other residence, or stop taking him there overnight.
Shortly after that, she said, she received a statement in writing from the house manager that she had purchased new memory-foam mattresses for Tim for both the East Longmeadow and Wilbraham residences.
But Tim’s back problems continued. And after visiting his East Longmeadow residence in January, Jessica went into his bedroom to look at his mattress that the house manager said she bought for him. There was not a memory foam mattress or box spring in his room, she said. Instead, he still had a futon mattress, and the tag on the mattress was so old that the letters were not legible.
No documented doctor’s appointments for seven years
In a letter sent in January to DDS Area Director Dan Donnermeyer, Mary said that she and Jessica were told the previous fall that a doctor’s appointment had been scheduled for Tim, but that the appointment kept getting rescheduled by the group home management.
In an email to COFAR, Jessica stated that during an ISP meeting last October, the then house manager had told her a physical for Tim had been scheduled for the following month of November. But in November, the house manager said the appointment had been rescheduled by the doctor’s office to late December.
Then, the day before the scheduled December doctor’s visit, the house manager told Jessica there had been “a miscommunication,” and Tim’s appointment had been moved to March 2019.
Jessica then called the doctor’s office directly. The receptionist confirmed that Tim did indeed have an appointment scheduled for March 2019, but that the appointment had only been made one day prior to her call on December 21, and that it was a new-patient visit because Tim had never been seen at that office.
At that point, Jessica wrote, she asked that CHD in December to provide her with documentation of Tim’s last visit to a primary care physician, as well as his last visit to his cardiologist, who he is supposed to be seeing annually for his congenital heart defect.
Mary provided us with CHD’s documentation of a visit to a Dr. Masih Farooqui in Wilbraham in January 2011, which she said was the most recent doctor’s visit that CHD was able to document. She said the most recent visit to a cardiologist for which CHD provided documentation was in 2012.
Despite that, Tim’s ISP documents, which are dated October 2018, contain a claim that his last physical was in September 2018. The 2018 ISP also lists the name of Dr. Farooqui as Tim’s primary care physician. Mary believes the visits claimed in the ISP never occurred.
The 2018 ISP also listed Dr. Farooqui as practicing at the 77 Boylston Street, Springfield, address of Hampden County Physician Associates. COFAR confirmed, however, that Hampden County Physician Associates no longer exists, and that Dr. Farooqui is now on the oncology staff of the Mercy Medical Center in Springfield.
COFAR was unable to reach Dr. Farooqui to confirm the year that he left that primary care practice.
Back pain prescription not filled
Mary said that on January 14 of this year, Jessica brought Tim to an Urgent Care clinic after CHD contacted her to report that Tim was continuing to experience severe back pain. She said she subsequently learned that group home staff had taken Tim to the same clinic a couple of weeks before at the end of December without her knowledge.
Mary said that after doing X-rays at the January Urgent Care visit, the doctor told Jessica that Tim had deterioration of muscle between vertebrae in his back, and that the pain he was experiencing could have been alleviated with physical therapy in 2017 when he first began complaining of back pain.
Mary added that during the previous Urgent Care visit in December, which was also for back pain, Tim was given medication and was prescribed a muscle relaxant. However, she said, CHD later informed her that the manager on duty at the group home never had the prescription filled. This resulted in continuing back pain and spasms for Tim.
Meanwhile, Jessica found out at the January Urgent Care appointment that Tim’s Mass Health coverage had been allowed to lapse for the past two years and that his Massachusetts state ID had also lapsed.
Removal from day program
In May 2017, Mary discovered that Tim had been removed from his day program at WOC without her knowledge or consent and in violation of his ISP. She said she also learned that Tim had been left alone in his group home during the day for the previous two months.
In a lengthy letter of explanation to Mary, dated in June 11, 2017, the then group home manager acknowledged that she had removed Tim from the day program, and apologized for “…my failure to talk with you and get your permission/input/opinion…”
The group home manager’s letter stated that after a sheltered workshop program at WOC was terminated (along with all remaining sheltered workshops in the state as of 2016), the manager found that there was little for Tim to do at WOC. She said she then organized a series of other activities for Tim and planned to enroll him in a “wrap-around” program approved at CHD to replace the WOC program.
Mary responded to the group home manager in an email, saying that she wasn’t taking issue with the reasons the manager had listed in her letter for removing Tim from his day program, but with the fact that she had done it without Mary’s knowledge or consent.
Mary also told DDS that she was later told by a CHD supervisor that the supervisor was unaware Tim had been removed from the WOC program, and that CHD did not have a replacement wrap-around day program as the former group home manager had claimed.
Mary added that, “no one from CHD can tell me where Tim was and who he was with for those two months” during which he was removed from the WOC day program.
Not receiving Social Security funds
In March of this year, Mary discovered that Tim had not received his Supplemental Social Security Income (SSI) since 2017. The federal SSI funds were supposed to be sent to his account managed by the group home. The funding had lapsed due to CHD’s failure to update the Social Security Administration with current information about Tim.
For two years, Mary said, the group home did not receive Tim’s monthly SSI payment of $670 from which Tim was supposed to receive a $100 monthly stipend for his needs. The missed funding over the two years totaled $2,400 that Tim needed for items such as underwear, socks, pants, shorts, sneakers, and a spare set of sheets.
DPPC referred to DDS, which found no risk of serious harm
In March, Mary filed a complaint with the DPPC alleging both neglect and financial abuse in Tim’s CHD group home. Her complaint noted that Tim had not received SSI benefits for at least two years and that he had not been seen by a doctor and had been medically neglected for at least seven years.
A separate complaint from an anonymous reporter stated that $2,000 in clients’ food stamp benefits had been taken from the two CHD group homes in East Longmeadow and Wilbraham. Both complaints appear to have been referred by the DPPC to DDS. The DDS resolution letter, dated June 7, stated that the group home manager had resigned from the group home.
The resolution letter also concluded that there was no indication of serious risk of harm to Tim. However, the letter stated that CHD had been required to respond within 30 days concerning:
- Medical appointments that have not occurred as recommended in the provider’s residences.
- Oversight that exists to ensure proper medical care in those residences.
- An accounting of food stamps taken from group home residents.
Mary filed for reconsideration of the DDS letter, disputing the finding that Tim was not at risk. For years, she noted, he was denied medical attention to monitor a hole in his heart. He was further denied treatment from 2017 to 2019 for his back pain despite having been recently diagnosed with a degenerative back disk.
Mary also contended that Tim’s loss of two years of SSI income had caused him emotional distress due to a shortage of clothing, and that he is due back payment from CHD of at least $2,400.
Mary argued that CHD needs an individual to oversee and manage all Social Security representative payee duties, and needs to ensure renewal of all MassHealth and state IDs for all clients. She further called for a review of licensing of DDS group homes. “How could seven years of missed medical and dental appointments go unnoticed?” she asked.
DDS licensure report doesn’t show any serious problems
DDS most recent online licensure report for CHD, which is dated June 2017, did not note any issues with medical care in the CHD’s residential facilities except to state that medical plans for two residents “did not fully address all required elements.”
The licensure report stated that “the vast majority of individuals in the survey sample were supported to receive timely annual physical and dental examinations, attend appointments with specialists, and receive preventive screenings as recommended by their physicians.”
The licensure report stated that audits had been completed at six 24-hour CHD residential locations, but did not say how many residential locations the provider has in total.
In her June 2017 letter to Mary, the former house manager indicated that Tim’s home was going to be inspected as part of the DDS licensure process. Her letter stated:
…in addition to my normal responsibilities I have been preparing for our licensing process (kind of like an audit) which is incredibly stressful. I was chosen mid May…both of my houses…which prompted me to work 16-hour days for weeks and try to make sure everyone still was busy, happy and having a good life.
DDS has not provided answers to Mary’s questions
Mary said that to date, her questions to DDS about Tim’s care and how his group home was able to be relicensed have gone unanswered. She said that during a May meeting to discuss Tim’s ISP, DDS and provider officials declined to discuss the many issues that she had raised.
“They only wanted to talk about correcting the ISP,” she said. “They all apologized (for the problems), but said ‘all we can do is move forward.'”
But while the officials said the former group home manager had resigned and a new manager was hired, Mary said that new manager quit in the beginning of May, telling her he was not receiving adequate support from the provider or DDS.
It isn’t surprising that DDS doesn’t want to talk about what has gone wrong in Tim’s group home for the past several years. It’s always much easier to say “let’s look forward.” But that is a prescription for continuing to repeat the mistakes of the past, and is, in fact, a tacit acknowledgement that the Department isn’t serious about addressing those problems.
We think the Attorney General’s Office needs to investigate this case and others like it as part of an overall investigation of the DDS group home system. After we met with staff of the AG in May, those officials expressed interest in undertaking such an investigation.
The Legislature’s Children, Families, and Persons with Disabilities Committee, has also done little or nothing that we know of to date to address or examine these issues. We have not heard of any results from two informational hearings that the Children and Families Committee held last year on abuse and neglect in the DDS system.
Massachusetts is a leader on many public policy fronts, but when it comes to care of the developmentally disabled, this state has a lot of catching up to do.
The late Judge Joseph L. Tauro honored at memorial service
The late United States District Court Judge Joseph L. Tauro, who paved the way for improved care for thousands of persons with developmental disabilities in Massachusetts, was honored on June 7 in a memorial service at the Moakley federal courthouse in Boston.
From 1972 through 1993, Judge Tauro oversaw Ricci v. Okin, a combined class-action lawsuit first brought by the late activist Benjamin Ricci over the conditions at the Belchertown State School. The lawsuit resulted in a consent decree that included the then Belchertown, Fernald, Wrentham, Dever, Monson, and Templeton state schools.
![]()
Tauro, who died in November at the age of 87, had visited Belchertown and the other Massachusetts facilities in the early 1970s to observe the conditions first hand. He noted two decades later in his 1993 disengagement order from the consent decree that the legal process had resulted in major capital and staffing improvements to the facilities and a program of community placements.
Together, those improvements and placements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world,” Tauro wrote.
Among those attending the June 7 memorial service were former Governor Michael Dukakis, who signed the consent decree in 1975 on behalf of the State of Massachusetts, and Beryl Cohen, the original attorney for the plaintiffs.
Speakers at the June 7 service included U.S. Supreme Court Associate Justice Stephen G. Breyer, Senior U.S. District Judge Michael A. Ponsor, Governor Dukakis, and Major League Baseball Commissioner Robert D. Manfred Jr. Manfred, an attorney, clerked for Tauro after graduating from law school.
Also attending the service were Ed and Gail Orzechowski, advocates for persons with developmental disabilities. Ed Orzechowski’s 2016 book, You’ll Like it Here, chronicled the life of the late Donald Vitkus, a survivor of the Belchertown school.
In March, as Ed Orzechowski received the 2019 Dr. Benjamin Ricci Commemorative award from the Department of Developmental Services, he credited three men with improving the lives of persons with developmental disabilities in Massachusetts — Benjamin Ricci, Beryl Cohen, and Judge Tauro.
Ed Orzechowski (left) with former Massachusetts Governor Michael Dukakis, who signed the 1975 consent decree in the landmark Ricci v. Okin lawsuit overseen by Judge Tauro.

Gail Orzechowski, an advocate for the developmentally disabled (left), with Beryl Cohen, the attorney for the plaintiffs in the 1972 class action lawsuit, Ricci v. Okin. Gail’s sister, Carol, is a former resident of the Belchertown School.

A written remembrance of Judge Tauro in the memorial service program.
Federal deinstitutionalization bill would lower human services care standards
Unfortunately, the entire Massachusetts congressional delegation has signed onto a newly filed bill in Washington, which, as currently written, would encourage further unchecked privatization of human services, diminished oversight, and reduced standards of care across the country.
In Massachusetts, the bill, known as the federal Disability Integration Act of 2019 (HR.555 and S.117), would threaten the Wrentham Developmental and Hogan Regional centers, the state’s only two remaining residential facilities for the developmentally disabled that meet federal Intermediate Care Facility (ICF) standards.
Moreover, we think the bill does not comply with the law under the 1999 U.S. Supreme Court decision in Olmstead v. L.C., which recognized the value and legitimacy of institutional or congregate care for those who want and need it.
HR.555 (and the Senate version, S.117) calls explicitly for the the “transition of individuals with all types of disabilities at all ages out of institutions and into the most integrated setting…” (emphasis added). The legislation specifies that the federal government would provide funding for technical assistance to states “to prevent or eliminate institutionalization” of persons with developmental disabilities.
This language does not comport with Olmstead, which held that that the Americans with Disabilities Act (ADA) does not condone or require removing individuals from institutional settings when they are unable to benefit from a community-based setting. In addition, the ADA does not require the imposition of community-based treatment on patients who do not desire it.
At the very least, the language in this bill should be changed to respect the choice of individuals, families, and guardians, either to apply to get into, or to remain in congregate-level care facilities.
So far, we have made our concerns known to the office of Senator Elizabeth Warren, and have requested that Warren reconsider her co-sponsorship of the bill. A staff member said the office will look into our concerns and will convey them to the office of Senate Minority Leader Charles Schumer, the lead sponsor of the bill.
We plan to contact the office of Senator Edward Markey and other members of the Massachusetts delegation as well.
Failure to acknowledge problems with deinstitutionalization
HR.555 perpetuates the myth of institutions as providing “segregated” care. It fails to acknowledge the relentless pursuit of deinstitutionalization in recent decades, which has caused “human harm, including death and financial and emotional hardship.”
What the bill particularly fails to take into account are the major upgrades in care and standards in congregate-care facilities since the 1970s, largely as a result of federal lawsuits brought in Massachusetts and other states.
The irony is that while those lawsuits also led to the introduction and growth of privatized, community-based care throughout the country, poor oversight and low pay and training of staff in the privatized group-home system has recreated many of the warehouse-like characteristics of large institutions prior to the 1980s.
The bill falsely purports to encourage choice
HR.555 states that its purpose is “to clarify that every individual who is eligible for long-term (human) services and supports has a federally protected right to be meaningfully integrated into that individual’s community…” in order to receive those services and supports.
But the bill states that a group home or other facility can only be considered community-based if it has four or fewer unrelated residents. That is an unworkable and actually choice-limiting proposition that is almost as radical as the position of the National Council on Disability that an institution is a facility with four or more people who did not choose to live together.
So, while the bill purports to be in favor of choice, the only choice it recognizes as valid is a community-based setting; and that means a residential setting with four or fewer residents.
But the Supreme Court held in Olmstead that congregate care is appropriate for some persons with developmental disabilities. In Massachusetts, we have repeatedly heard from families and guardians who are satisfied with the high level of care delivered in the Wrentham and Hogan centers.
The people remaining at Wrentham and Hogan are more profoundly disabled and have more serious medical issues on average than in other DDS settings. These people need the intensive care that is regulated by ICF-level standards. HR.555 does not recognize the distinctions or the different levels of care needed by different individuals.
In fact, the real purpose of the bill, in our view, is to eliminate the choice of ICF-level care, which is based on strict federal standards for staffing, in particular.
The political impetus to close all remaining congregate care settings comes, as it has for years, from state-funded, corporate human services providers, who have a conflict of interest because they stand to gain additional state contracts as state-run facilities are closed and their functions are privatized.
Massachusetts, as do most states, allows the providers to operate under a waiver of the ICF regulations, which permits lower standards of care for community-based services. Even so, the cost of that care is oustripping the ability of states to pay for it.
The cost is not identified
HR.555 would require states to offer community-based services immediately to all persons needing such services, and those jurisdictions would not be allowed to impose cost caps or use waiting lists. The bill, however, does not identify what the cost of such a requirement would be or where the funding would come from.
The VOR, which advocates nationally for persons with developmental disabilities, calls the bill “clearly unaffordable.” Simply encouraging, funding, or requiring the transfers of more people out of institutions into community-based care will only exacerbate problems in the latter system.
To the extent that the bill recognizes the cost of care, it attempts wrongly to place the blame on institutions. It refers to “billions of dollars in unnecessary spending related to perpetuating dependency and unnecessary confinement.”
This statement, however, does not recognize the high cost of executive salaries and of mismanagement in the community-based system. In Massachusetts, the cost of institutional care is less than 10% of the cost of privatized, community-based care.
The bill, however, does appear at least to recognize that there are costs in providing community-based care because the bill would require states and providers to review their funding sources and analyze “how those funding sources could be organized into a fair, coherent system that affords individuals reasonable and timely access to community-based long-term services and supports.”
Such a review sounds reasonable, and we think it should be done before legislation is enacted that would encourage further deinstitutionalization. As noted, the deinstitutionalization required by this bill would place a significant financial strain on the community-based care system for which no additional funding has been identified.
We would suggest that people contact the members of the Massachusetts congressional delegation, whose contact information can be found at this site: https://lwvma.org/your-government/federal/.
We hope all of the members of the delegation will reconsider their support of HR.555 and S.117.
COFAR asks state attorney general to take a more active role in protecting the developmentally disabled
COFAR members met last week with officials in the state Attorney General’s Office to raise concerns about an apparent lack of focus by the state’s chief law enforcement agency on abuse and neglect of persons with developmental and other disabilities.
While Attorney General Maura Healey’s office has lately taken an active role in scrutinizing and penalizing operators of nursing homes that provide substandard care to elderly residents of those facilities, the same cannot be said of her office when it comes to investigating corporate providers of group homes for the developmentally disabled.
In March, Healey announced a series of settlements totaling $540,000 with seven nursing home operators for violations of standards of care and conditions in those facilities. In light of the attorney general’s actions and the substantial media coverage that resulted from them, COFAR asked Healey’s office for records of similar fines, settlements or penalties levied against Department of Developmental Services providers from Fiscal 2015 to the present.
In response, the AG provided records of just two cases in which penalties were imposed on DDS providers. In one case in 2017, a provider, the Cooperative for Human Services, Inc., was required by the AG to pay $19,000 in restitution to employees who had been denied overtime payments, and to pay a $4,000 fine to the state.
In the second case in 2018, Triangle, Inc. was required to donate $123,500 to charities for having paid less than the minimum wage to participants in a former sheltered workshop, without having a proper minimum wage waiver. The provider was also required to pay $6,500 to the AG’s Office to cover administrative costs.
So, that’s seven actions taken by the AG totaling more than half a million dollars against nursing home providers in just one month, versus two actions totaling $153,000 taken against DDS providers in the past five years.
Moreover, the larger of the two actions against the DDS providers was for paying subminimum wages to sheltered workshop participants — something that is seen as a problem only by opponents of sheltered workshops themselves.
As we’ve said many times, we see the real wage problem as the failure to pay adequate compensation to direct-care workers in the DDS system. That is an issue that the AG should be investigating, along with the excessive salaries paid in many cases to provider executives.
Investigating abuse and neglect
As for investigating abuse and neglect in the DDS system, the AG appears to have done nothing at least since Fiscal 2015. (We had originally asked for a list of penalties and other actions taken against DDS and its providers going back to Fiscal 2000. The AG responded that that request was overly broad in time and scope. As a result, we narrowed the request to DDS providers since Fiscal 2015.)
Certainly, the AG’s Office doesn’t present the only option for oversight of the DDS system. The Disabled Persons Protection Commission (DPPC) might be viewed as the most logical state agency to investigate abuse and neglect. That agency received more than 11,800 calls alleging abuse in Fiscal 2018 — a 74% increase from Fiscal 2010.
But with only four investigators on its staff, the DPPC is unable to investigate more than a tiny fraction of those calls, and must refer the vast majority of them to the Departments of Developmental Services and Mental Health, and the Massachusetts Rehabilitation Commission. As we have noted, those agencies face a conflict of interest in investigating abuse and neglect within their own systems.
The state Legislature should also be exercising investigative oversight of the DDS system; but the last major report from a legislative committee on abuse and neglect in facilities run by DDS and its providers was done in the 1990s.
Partly under prodding from COFAR, the Children, Families, and Persons with Disabilities Committee did hold two informational hearings last year on abuse and neglect of DDS clients. But it is unclear that the Committee intends to follow up on those hearings or even whether the hearings were, or are, part of a larger review.
The Children and Families Committee has never responded to questions from COFAR about the scope of its review, if any, of DDS. On Monday, I sent yet another email to the chief of staff of Representative Kay Khan, the House chair of the committee, asking what the status currently is of the committee’s review, and whether any additional hearings are planned. I haven’t yet received a response to that message.
AG officials acknowledge they could do more
In last week’s meeting with the AG officials, COFAR President Tom Frain, who called in; Vice President Anna Eves, and I raised concerns about the general lack of oversight of the privatization of care of the developmentally disabled in the state, and the high level of abuse and neglect as well as financial mismanagement in the system.
The three officials from Healey’s office — Jonathan Miller, chief of public protection and advocacy; Mary Beckman, chief of healthcare and fair competition; and Abigail Taylor, assistant attorney general for child and youth protection — acknowledged that the AG hasn’t done much in recent years in terms of oversight of the DDS system; but they said there may be opportunities for them to do more. Beckman said DDS clients fit within the AG’s purview, which is to protect vulnerable populations.
While none of the three officials were specific about what the AG could or might do, Miller talked about looking at “potential tools in our toolkit.”
The AG’s dual role
Beckman acknowledged that the AG’s Office is hampered in its oversight efforts by its dual roles as both a law enforcement and investigative agency, and as the state’s lawyer.
In fact, as the state’s defense attorney, the AG has consistently taken the state’s side in disputes since 1990’s over the closures of DDS state-run developmental centers and the expansion of the privatized group home system.
Nevertheless, the AG has penalized DDS providers, at least in the two instances cited above, so it clearly has the authority to do so. The key will be whether there is any follow-up by the AG’s Office to the general statements made in last week’s meeting with us.
It is unfortunate that despite the many state agencies with the authority and responsibility to investigate the care and conditions of people with developmental and other disabilities in Massachusetts, those persons appear to have fallen through the cracks in that system.
Somehow that large collection of institutional resources has not been enough to get the job done. In the case of the AG’s Office, we think the resources have so far been misdirected. We hope the Office will correct that.
State auditor finds direct-care workers were bypassed in funding boost for providers
The State Auditor has reported that a major boost in state funding in recent years resulted in surplus revenues for human services providers in Massachusetts, but that those additional revenues have led to only minimal increases in wages for direct-care workers.
Meanwhile, the leadership of the Massachusetts House of Representatives quashed a state budget amendment last month that would have raised direct-care wages to $20 an hour. That amendment had been co-sponsored by more than a majority of the House membership.
In a May 8 report, State Auditor Suzanne Bump’s office reported that so called Chapter 257 funding, which was at least partly intended to boost direct-care wages, “likely did not have any material effect on improving the financial wellbeing of these direct-care workers.”
The state auditor examined financial records of 89 human services providers, most of them under contract with the Department of Developmental Services. Among those surveyed providers, Chapter 257 funding helped boost their surplus of revenues over expenses on average from roughly $120,000 in Fiscal Year 2010 to $404,000 in Fiscal 2017, the audit stated. That is an increase of 237%, or an increase of almost 30% a year, in surplus revenues.
However, the audit stated that during that time, the average hourly rates paid direct-care workers increased by only 24% in total, or about 3.1% per year, on average. The audit pointed out that the yearly increase in average direct-care wages only exceeded inflation by about 1% per year.
The audit found that the average hourly direct-care wage was $11.92 in Fiscal 2010, and rose to $14.76 as of Fiscal 2017.
Under Chapter 257, which was enacted in 2008, state funding rates for social-service programs are set by the Executive Office of Health and Human Services (EOHHS). Before Chapter 257 rates were implemented, state agencies typically negotiated multiyear contracts with human-service providers and established individual reimbursement rates for each contract.
As of Fiscal 2017, DDS contracts accounted for $1.3 billion, or more than 55% of total Chapter 257 funding in Massachusetts, the audit stated.
House leadership kills wage increase for direct-care workers
Last month, the House leadership killed an amendment to the proposed Fiscal 2020 state budget that would have required that additional state funding to the providers be used to boost direct-care wages to $20 an hour. The amendment had been sought by SEIU Local 509, a state employee union that also represents human service provider workers.
An SEIU official said that even the Baker administration had supported the amendment, but that the providers opposed it.
No similar amendment has been filed in the Senate, which is currently debating the Fiscal 2020 budget. The SEIU official said the union will instead push for passage of a bill in the current legislative session (H.1658) that would accomplish the same thing as the House amendment. That bill is currently in the Labor and Workforce Development Committee, which has yet to take action on it.
Although the providers reportedly opposed the SEIU amendment, the Arc of Massachusetts, a key provider lobbying organization, is supporting a related bill, HD.1130, which would set a minimum rate of $17 per hour for wages paid to entry-level direct-care workers.
But unlike H.1658, which would require that the funding for the direct-care wage increases come from Chapter 257 funds, HD.1130 does not specify a source of funding for raising direct-care workers’ wages. It appears the providers don’t want the money for higher direct-care wages to come from their Chapter 257 funding, even if that funding is providing many of them with surplus revenues.
In 2017, the SEIU issued a report asserting that Chapter 257 had enabled the providers to earn $51 million in surplus revenues. The state auditor’s report this month stopped short, however, of asserting, as the SEIU did in 2017, that the providers could and should have used surplus revenues garnered from Chapter 257 rates to boost direct-care wages.
Both the state auditor’s report and the SEIU’s 2017 report provide confirmation of a report by COFAR in 2012 that direct-care workers in the DDS contracted system had seen their wages stagnate and even decline in recent years while the executives running the corporate agencies employing those workers were getting double-digit increases in their compensation.
The SEIU’s 2017 report stated that during the previous six years, the providers it surveyed paid out a total of $2.4 million in CEO raises. The SEIU report concluded that:
This all suggests that the amount of state funding is not at issue in the failure to pay a living wage to direct care staff, but rather, that the root of the problem is the manner in which the providers have chosen to spend their increased revenues absent specific conditions attached to the funding. (my emphasis)
The Massachusetts Legislature needs to demonstrate that it is on the side of the human services caregivers who perform some of the most difficult and thankless work possible, and not strictly on the side of the corporate executives who wield virtually all of the political influence on Beacon Hill.
While we strongly support proposed reforms to the human services system such as establishing a registry of caregivers with substantiated abuse charges against them, a registry alone will not solve the abuse problem. The problem of abuse is very much the fault of poor management and a lack of training and supervision from top management. And it is a direct result of the underpayment of those caregivers.
The direct-care workers are on the front lines when it comes to making the system work. Yet, those people are easy to forget in the political power struggles at the State House; and to the extent they are remembered, it is often as the sole object of blame for the failures of the system as a whole.
The Legislature can begin to right those wrongs by supporting H.1658 and ensuring a living wage for direct-care workers.
DPPC’s public presentation of data on abuse is unclear
After a lengthy series of inquiries from COFAR, the state Disabled Persons Protection Commission (DPPC) has acknowledged that data in its annual reports on abuse in Massachusetts do not necessarily reflect the actual number of cases that it investigates or refers for investigation.
In letters in response to an April 12 order by the state’s public records supervisor to clarify to COFAR how the DPPC reports its data, a DPPC official said that the numbers listed in the DPPC’s annual reports of both “abuse reports” and “investigations” are not necessarily based on separate occurrences of alleged abuse. Those numbers are based instead on the number of calls or “intakes” that the DPPC receives from witnesses or other reporters.
As a result, the DPPC’s data “may be “inflated” because the agency’s “current method of data extraction can produce duplications when multiple intakes are received on the same incident,” according to Andrew Levrault, the DPPC’s assistant general counsel. Levrault said the agency’s database was “undergoing a redesign process, and this is one of the features we are hoping to improve.”
Levrault also stated in an email that the DPPC’s data may be “deflated” in some other instances.
The DPPC undertakes investigations of alleged abuse and neglect of adults under 60 with disabilities in Massachusetts, and supervises additional cases that it refers for investigation to the Departments of Developmental Services (DDS) and Mental Health (DMH) and to the Massachusetts Rehabilitation Commission (MRC). As such, the DPPC’s data are relied on by policymakers, researchers, journalists, and others as important indicators of the quality of life of persons with disabilities.
In light of the critical role that the DPPC plays, it is vital that data and other information that the agency publicly provides about the care and conditions of persons with disabilities be accurate and presented in a clear and straightforward way.
Levrault said that in contrast to the DPPC, DDS, to which the DPPC refers most of its cases for investigation, does report data based on the actual number of cases it investigates.
The differences between the DPPC and DDS in reporting abuse data make it difficult to compare that data, not only among agencies in Massachusetts, but potentially between Massachusetts and other states. COFAR has been attempting to analyze aggregate data on abuse and abuse investigations done by the DPPC, DDS, and other agencies.
The DPPC’s most recent online annual report for Fiscal Year 2017 states that the agency received 11,395 “abuse reports” that year, and that of that number, 2,571 “investigations” were assigned to investigators from the DPPC, DDS, DMH, and the MRC.
In his May 1 letter, Levrault stated that:
…the 2,571 investigations listed in the Fiscal Year 2017 Annual Report specifically refers to investigations of 2,571 intakes.
Levrault stated in the email that a single intake may refer to one or more occurrences of alleged abuse, or conversely, that “multiple intakes” may refer to a single occurrence of alleged abuse.
As a result, it appears that while the DPPC annual report listed 2,571 “investigations” in Fiscal 2017, it is unlikely that that number represents the number of investigations that were actually undertaken by the DPPC and by DDS, DMH, and the MRC. Similarly, the 11,395 abuse reports listed in the annual report for that year may or may not represent the actual number of alleged occurrences of abuse that were reported to the DPPC.
In a comparison of data from both the DPPC and DDS, COFAR found that the number of abuse intake calls referred by the DPPC to DDS for investigation each year from Fiscal Year 2010 to 2018 was, on average, 22.5% higher than the number of cases that DDS reported investigating. (See chart below created from data from both agencies.)
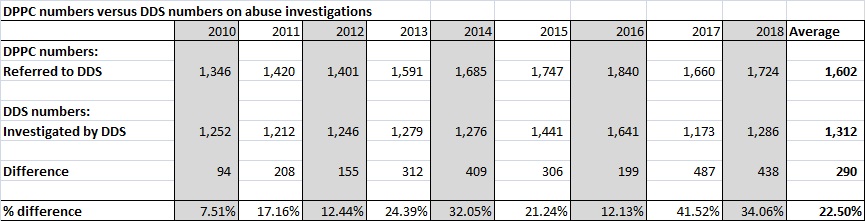
Those differences appear to be due to the differences in the ways that the DPPC and DDS report the data.
The accuracy of the DPPC’s data reporting is certainly a problem that can be corrected if and when the agency redesigns its database. It raises a question, however, as to why the DPPC has not made it clear in its annual reports as to what the data reported in them actually represents.
Yet, we have already seen that the DPPC is highly resistant to public disclosure of its investigative reports, and is pushing for legislation that would wrap a tighter cloak of secrecy around its records.
In failing to be clear about the meaning of its published data, the DPPC has not been transparent or straightforward about the scope and nature of the problem of abuse and neglect in Massachusetts.
The DPPC is the only independent agency available when family members or others discover abuse and neglect in the DDS system. Without the DPPC, the best option for reporters of abuse would be to dial 911. Yet the DPPC is an agency that needs to place a higher value than it currently does on the public’s right to know.
Legislators and the media should be concerned about secrecy in investigations of abuse of persons with disabilities
A bill in the state Legislature, which would draw an ever-tighter cloak of secrecy around investigative reports on abuse and neglect of persons with disabilities in Massachusetts (H.117), appears to be going relatively unnoticed on Beacon Hill and by the media.
Section 17 of the bill would effectively exempt all investigative reports and records of the Disabled Persons Protection Commission (DPPC) from public disclosure. Under the section, the DPPC’s records could be kept entirely secret even if all personal information in them were redacted.
At a certain point, laws and other initiatives that are ostensibly enacted or undertaken to protect privacy cross the line into secrecy and provide a curtain for agencies to hide behind. That is what we think is happening with Section 17 of this bill.
The DPPC is the state’s only independent agency charged with investigating allegations of abuse and neglect of adults under the age of 60 with developmental and other disabilities. Without access to the agency’s investigative reports, the public will have much less understanding, not only of the scope and nature of the problem of abuse and neglect, but what the DPPC and other agencies are doing about it.
Overall, H.117 and its counterpart in the Senate (S.53 ) propose making a number of changes to the DPPC’s enabling statute that seem helpful, such as replacing the term “disabled person,” with “person with a disability.” That latter term avoids the stigma associated with describing an individual totally in terms of their disability.

COFAR member Richard Buckley (left) and Vice President Anna Eves testify Tuesday at the State House about abuse and neglect of the developmentally disabled. At the hearing, COFAR offered testimony against proposed DPPC secrecy language in Section 17 of H.117.
However, Section 17 is not at all innocent, in our view. It would add language to the DPPC’s enabling statute stating that the agency’s records containing confidential or personal data “shall not be public records.” (my emphasis)
That proposed language is not needed to protect the personal privacy of victims of abuse and neglect or others involved in those investigations. The DPPC’s enabling statute currently states that the DPPC should disclose “as little personally identifiable information as possible.” That language gives the DPPC the discretion to protect the privacy of all parties involved.
The presumption of the state’s Public Records law is that all state governmental records are public documents unless they are explicitly exempted from disclosure by statute, or they fall under an exemption to the Public Records law itself.
At a legislative hearing this past Tuesday on H.117 and other bills concerning abuse of persons with disabilities, DPPC Executive Director Nancy Alterio touted the anti-stigmatizing aspects of H.117, but did not mention Section 17. Both Anna Eves, COFAR’s vice president, and I testified before the Children, Families, and Persons with Disabilities Committee against the section.
The committee members didn’t ask us any questions about our objection. We may have caught them by surprise about it.
The House and Senate versions of the bill were filed by Representative Sean Garballey and Senator John Keenan.
In February, Garballey got back to me and said he wasn’t aware of the implications of the Section 17, and would ask the DPPC about it. He said he agreed with us that the enabling statute should not completely restrict the disclosure of the DPPC’s records.
The chief of staff for Sen. Keenan was more noncommittal about the bill, but also said she would look into and ask about our concerns.
The mainstream media don’t seem to be paying attention this year
On March 21, I emailed Boston Globe Editor Brian McGrory, laying out our concerns in detail and asking whether the Globe might take a position against the language in Section 17. To date, McGrory has not responded to that or to a subsequent email I sent about the bill on April 5 and again on April 8 to The Globe and other news organizations around the state.
The New England First Amendment Coalition published our email to mainstream media outlets on its blogsite on April 8. But we have gotten little or no response from the rest of the media either.
Our media list includes current editors and other staff on 24 newspapers, including the Globe and Herald; major chains such as the North of Boston Media Group; the Associated Press, the State House News Service; CommonWealth Magazine; major Boston television news outlets; and NPR radio affiliates WBUR and WGBH.
The Globe in the past has taken strong stances in favor of the public disclosure of state records. In 2015, the paper organized coordinated editorials among several media outlets criticizing the state’s Public Records supervisor for rulings allowing the withholding of records from public disclosure by state agencies.
The Globe’s 2015 editorial maintained that the state’s criminal-records law, in particular, “was never intended to open up a memory hole to conceal unflattering information about the police.”
That is similar to the argument we have made in seeking to obtain investigative records from the DPPC. And now, Section 17 would make that cloak of secrecy even more opaque.
DPPC heading in the direction of the Elder Affairs office
Unfortunately, with the introduction of Section 17 in H.117, it appears that the DPPC is seeking to emulate the Executive Office of Elder Affairs (EOEA), which investigates abuse and neglect of persons 60 and older. The EOEA’s enabling statute does state that the agency’s records are not public.
On its website,the DPPC states that the reason for the non-public records provision in H.117 is to make the DPPC’s enabling statute conform to the EOEA’s statute in order to give persons with developmental disabilities “the same safeguards provided for the records of elders.” (Please note that the bill numbers on the DPPC website appear to be from the prior legislative session.)
But that only raises further concerns for us about the potential secrecy of the EOEA’s records.
As noted, the enabling statute of the EOEA, M.G.L. c. 19A, s. 23, explicitly states that departmental records containing confidential information are not public. The EOEA statute goes even further, giving the Elder Affairs Department the authority to actually destroy investigative records about abuse allegations if the department finds that the allegations are unsubstantiated. This seems to us to be bad law and not one that the DPPC should be emulating.
The DPPC’s regulations go further than the enabling statute in exempting records from disclosure
While the DPPC’s regulations explicitly state that the DPPC’s records are not public , the agency’s enabling statute, as noted, says only that the DPPC should disclose “as little personally identifiable information as possible.”
The DPPC’s regulations go further in shielding the agency’s records from public disclosure than does the enabling statute, and we think the regulations should therefore be changed to conform to the enabling statute. H.117, however, would do the opposite by making the statute conform to the regulations.
We hope The Globe and other media outlets in Massachusetts wake up to the threat this bill poses to transparency in state government. The DPPC receives tens of thousands of allegations of abuse and neglect each year, and “screens in” several thousand of those for investigation.
It is already extremely difficult to obtain those records from the DPPC even in redacted form. H.117 would make it virtually impossible to obtain those records, and would move state government that much further away from operating with openness and transparency.
DPPC ordered to clarify its abuse reporting system following data inflation admission
In the wake of an acknowledgement by the Disabled Persons Protection Commission (DPPC) that some of the data it had provided COFAR on abuse may be inflated, the state’s public records supervisor has ordered the agency to clarify the nature of the data it publishes.
The April 12 decision by Public Records Supervisor Rebecca Murray is in response to an appeal filed by COFAR after the DPPC stated that it was unable to provide data on the actual number of “abuse allegations” the agency receives each year and the number of such allegations that are substantiated by investigations.
In emails in March, Andrew Levrault, DPPC assistant general counsel, stated that spreadsheet data on abuse complaints and investigations, which the DPPC had previously provided to COFAR, “may be inflated.” He later stated, in a response to COFAR’s appeal, that the DPPC’s data may be “deflated” in some other instances.
Levrault said that the probable data inflation occurred because the agency does not track actual abuse allegations, but rather tracks abuse “intakes,” which are calls made to the agency. He said there may be “multiple” intake calls for each allegation, and that the DPPC is unable to “extract” the number of actual allegations that the agency receives.
Levrault’s statements appear to leave it unclear whether data listed in the DPPC’s annual reports accurately represents the number of abuse allegations or incidents that the agency is informed of or investigates. Levrault did claim in an email that the numbers in the annual reports are not inflated.
In her April 12 decision, Murray stated that while the DPPC has noted that it cannot extract data by allegation, “the DPPC did not clarify whether it could produce the data to back up the numbers DPPC uses to draft its Annual Reports.”
Murray noted that COFAR has questioned “how it is possible that DPPC is able to report the number of abuse reports and number of investigations, if it cannot extract that data from its database. I find that DPPC must clarify this.”
In an email on March 14, Levrault acknowledged deficiencies in the DPPC’s abuse tracking system. He stated that:
…our current method of data extraction can produce duplications when multiple intakes are received on the same incident. The database is undergoing a redesign process, and this is one of the features we are hoping to improve.
Later, in an April 8 response to COFAR’s records appeal, Levrault stated that when compared to the record keeping system used by the Department of Developmental Services (DDS), to which the DPPC refers many of the abuse complaints it receives:
… the DPPC’s figures may be elevated in some instances, and may be deflated in others–depending on the nature of the comparison.
Yet, when asked by COFAR, also on March 14, whether the numbers of “abuse reports” listed in the DPPC’s annual reports are therefore likely inflated, Levrault replied that the numbers in the annual reports “are not inflated. They are consistent with our long-standing statutory reporting requirements, which mandate that we report the ‘number of claims of abuse.’ (emphasis in the original)
Levrault did not explain how it could be the case that the DPPC is able to report accurate or non-inflated numbers in its annual reports if the agency is unable to track or extract data on abuse allegations, and tracks only data on intakes.
The DPPC’s most recent annual report for Fiscal Year 2017 states that the agency received 11,395 “abuse reports” that year, and that it had “screened in” 2,571 of those reports for investigation by the DPPC itself and other agencies.
The annual report stated that the same number of 2,571 “investigations” was assigned to investigators from the DPPC, the Department of Developmental Services, the Department of Mental Health, and the Massachusetts Rehabilitation Commission, and that those investigators had completed 1,866 of those investigations.
It is unclear whether the 11,395 “abuse reports” cited in the 2017 annual report is a reference to intakes or to allegations. However, given that the annual report refers to 2,571 of those 11,395 abuse reports as representing “investigations,” it would appear that the number 11,395 does refer to actual allegations.
If, however, it is the case that the spreadsheet data provided to COFAR by the DPPC is inflated, it would render that data virtually useless in attempting to determine the number of abuse allegations that agency receives and investigates each year.
However, Levrault also stated in a separate email on March 14 that:
Each intake received by the DPPC is assigned a separate case number. If the DPPC receives multiple intakes involving the same allegation and the allegation meets the DPPC’s jurisdiction, then the intakes will be combined for investigation. Moving forward, the DPPC case would then be identified by the combined intake numbers. (my emphasis)
That statement by Levrault appeared to imply that the agency does, in fact, keep documentation on the number of abuse cases that it either investigates or refers to other agencies for investigation.
As a result, COFAR asked the DPPC on March 15 for the number of abuse allegations and investigations resulting from intake reports that the DPPC had “combined for investigation.” When Attorney Levrault responded that the DPPC had no responsive records to that request, COFAR appealed the matter to the state’s Public Records Supervisor.
DDS does track abuse allegations
As noted, Levrault stated in his April 8 response to COFAR’s appeal that unlike the DPPC, DDS does have the capability of tracking individual abuse allegations or cases. The DPPC refers the majority of the abuse complaints it receives to DDS for investigation.
COFAR has previously reported that the DPPC actually has a lower abuse-allegation caseload per investigator than DDS, and that the DPPC has substantiated a higher percentage in recent years of the allegations it has investigated itself than has DDS.
In reporting those percentages, COFAR was assuming that the DPPC was consistent in reporting the number of allegations it was investigating itself, and the number of allegations that DDS was investigating.
In the past year, we have been battling with the DPPC over the transparency of the agency’s investigative policies. We think our latest appeal concerning the data the DPPC publishes underscores the need for a major review and overhaul of those policies and procedures.
Ed Orzechowski receives the Ricci award and calls for memorial to residents of former Belchertown State School
Ed Orzechowski, a former COFAR vice president, accepted the 2019 Dr. Benjamin Ricci Commemorative Award on Wednesday, and called for the establishment of a “lasting memorial” at the former Belchertown State School.
The annual Ricci award celebration recognizes the accomplishments of individuals served by the Department of Developmental Services, and the dedication of caregivers and advocates.
“I urge the Department of Developmental Services, the Legislature and local officials to create a lasting respectful memorial, a tangible commemoration to all the living and deceased former residents of Belchertown and the other institutions,” Orzechowski said in accepting the award. “What they (the Belchertown residents) experienced, what they endured, must not be forgotten.”

Ed Orzechowski accepts the Benjamin Ricci award at the State House on Wednesday. At left is Orzechowski’s wife, Gail, who has worked with Ed in advocating for residents of DDS facilities.
Orzechowski authored “You’ll Like it Here,” a gripping book published in 2016 about the life of Donald Vitkus, a one-time resident of the former Belchertown State School.
Orzechowski’s book chronicled Vitkus’s childhood in the 1950s at Belchertown, which was then notorious for its inhumane and unsanitary conditions. The book also described Vitkus’s battle throughout the rest of his life to come to terms with his past at Belchertown.
In addition to serving for many years on COFAR’s Board, Orzechowski was president of the Advocacy Network, a former advocacy organization for the developmentally disabled in western Massachusetts.
In Wednesday’s State House ceremony, DDS Commissioner Jane Ryder presented the Ricci award to Orzechowski. The award is named for Ben Ricci, the original plaintiff in the 1970s landmark federal class action lawsuit, Ricci v. Okin, that brought about upgrades in care for residents of Belchertown and other Massachusetts facilities for the developmentally disabled.
During the Wednesday ceremony, Orzechowski noted the importance of the efforts of three key individuals in the Ricci case, including Ricci himself, the late U.S. District Court Judge Joseph L. Tauro, who oversaw the class action lawsuit, and Beryl Cohen, the attorney for the plaintiffs. “Without the convergence of these three men, conditions for people who were called retarded—clinically labeled idiots, imbeciles, and morons—would not have improved the way they did,” he said.
Orzechowski also talked about his friendship with Vitkus, who died in January 2018 and was buried as was his wish in the Warner Pine Grove Memorial Cemetery for residents’ at Belchertown. In the course of writing the book, Orzechowski and Vitkus had become close; and a year ago, when Vitkus himself was selected to receive the Ricci award posthumously, Orzechowski was on hand at the State House to accept it on Vitkus’s behalf.
During Wednesday’s ceremony, Orzechowski also thanked his wife, Gail, for her advocacy efforts on behalf of her sister, Carol, who was a Belchertown resident during the period of abuse and neglect.
“I know Carol would thank you Gail, if she could,” Orzechowski said. “You are the one who has fought so hard for Carol and the human rights of so many others. You and the other family members and caregivers here have spoken up for your loved ones, and fought for the necessary funding to sustain their care. I only wrote a book. You live it every day. You deserve applause.”
Gail Orzechowski joined Ed at the podium at that point.
In discussing his call for a memorial at the Belchertown School, Orzechowski noted that he recently visited the grounds of the school, which was closed 26 years ago, and found the place to be “barely recognizable.” The town, he said, has built a new police station there, and there is now a modern continuing care facility on the site.
There are aso plans to construct a substantial brewery on the grounds. All that remains of the state school, he said, is the crumbling administration building and a few former residence halls.
Orzechowski said that while he has heard of plans for a walking trail with plaques to be a remembrance, he felt there needs to be something more substantial. He called for a museum on the grounds and for a memorial, a place for archives, and photos and exhibits.
“Many of us worked hard to close the institutions… the redevelopment of those properties is to be expected…and there’s much to be celebrated in the improved lives of our citizens with developmental disabilities,” Orzechowski said. He added that, “Today Wrentham and Hogan provide much-needed services for their residents, and community settings are much more homelike.”
At the same time, Orzechowski said, “there’s an irony here. What happened in the twentieth century at Belchertown, what happened at Monson, Dever, Glavin, Wrentham and Fernald—eugenics, radiation experimentation, day-to-day abuse and neglect—cannot be erased and should not be forgotten.” He added that existing archives involving residents of the state school are scattered and disorganized.
Orzechowski is currently at work on a second book about another Belchertown state school resident named Darlene. He said that when he told her about what is left of the institution, she said, “It’ll be like we were never there, like we never existed.”
Supported Decision Making bill needs clarity and safeguards
We’ve recently expressed concerns about “Supported Decision Making” (SDM), a growing movement to restrict guardianships of persons with developmental disabilities and replace those guardians with “networks” of more informal advisors.
In that vein, a bill to promote SDM in Massachusetts (HD.666 in the House and SD.843 in the Senate) does little to alleviate our concerns.
We think SDM can hold promise for some high-functioning individuals, and we would support its adoption with adequate safeguards, particularly safeguards against the potential marginalization of family members.
The problem with the bill is that there appear to be few, if any, such safeguards in it, and the bill provides no standard for determining who might be eligible for an SDM arrangement.
Under SDM, individual guardians are replaced by teams or “network supporters,” who enter into written agreements with disabled individuals to help them make decisions about their care, finances, living arrangements and other areas. SDM proponents maintain that guardianship unduly restricts the rights of disabled individuals to make those decisions.
But the bill skirts the question whether everyone is really capable of making their own decisions in those very important areas. The bill states that, “with support, many people with disabilities can make their own decisions…” (our emphasis). That statement actually says very little.
What the bill does state explicitly is that under SDM, the developmentally disabled individual is the “decision maker” regarding their services and their financial and legal affairs.
But can someone with a profound intellectual disability, for instance, be considered capable of making their own decisions even with assistance from an SDM team? As one public advocacy organization put it in relation to SDM, is it possible for anyone to make their own decisions “if they do not have…an appreciation of the significance of the decision they are making or a reasonably consistent set of values?”
The bill simply doesn’t address those questions. As a result, it seems possible the assumption underlying the bill is that yes, many individuals are capable of making these decisions even if they have “significantly sub-average intellectual functioning,” lack the ability to communicate, and lack practical living and conceptual skills.
SDM proponents need to recognize that there are some individuals who do not have the cognitive skills necessary to make reasonable decisions. Those people need guardians.
It’s not sufficient to insert a vague statement into proposed legislation that “many people” are capable of making their own decisions. Where does that capability begin or end? What the bill needs to specify is a threshold level of cognitive ability, determined through research, above which SDM would be permissible and below which it wouldn’t.
The problem is that many SDM proponents refuse to recognize that such a threshold level even exists. The American Bar Association, for instance, rejects the use of a clinical standard or diagnosis of cognitive ability in determining whether an individual is capable of making their own decisions.
Little or no protection from conflicts of interest or exploitation
There is also nothing in the language of the bill to prevent human services providers from being placed on the SDM teams — a situation that would seem to set up a potential conflict of interest.
We have seen many cases, for instance, in which family members have made allegations of poor care or conditions in group homes, and the providers have not only ignored the families’ concerns, but have, in some cases, retaliated against the families. In too many of those cases, DDS has taken the side of the providers.
It’s not hard, in instances like that, to imagine the outcome if a representative of the provider and of DDS were on the individual’s SDM team. The family member would be consistently “outvoted” on decisions about the person’s care.
There is, moreover, no provision in the bill for preventing the exploitation of developmentally disabled persons other than a provision that anyone who has reason to believe that someone is being exploited can report that to the Disabled Persons Protection Commission (DPPC). There is not a requirement, however, that the DPPC actually investigate such a complaint or that the DPPC not refer the complaint to another agency such as the Department of Developmental Services for investigation.
There is also no provision in the bill that would provide for regular auditing or other oversight of SDM agreements.
In addition, there is a provision in the bill that appears to offer SDM as an alternative to guardianship even for children. The bill appears to imply that even children with intellectual disabilities would be considered eligible to make their own financial and legal decisions. We’re not sure that even children of normal cognitive ability have that legal right under most circumstances.
Unfortunately, it appears to us that many proponents of the SDM movement do not want to adopt safeguards or standards, possibly because that process could lead to debate and disagreement that might slow the SDM movement down. We think taking the time to resolve disagreements and adopting standards would ultimately be the best way forward for SDM and for the disabled individuals it is intended to help.
