Archive
A compelling new book chronicles a girl’s life at the Belchertown State School
Edward Orzechowski has done it again. He has written a second gripping, as-told-to account of life within the notorious and now long-closed Belchertown State School in western Massachusetts.
The launch of his new book, “Becoming Darlene,” is scheduled for November 23 at 1 p.m. at the Florence Civic Center in Florence, MA.
“Becoming Darlene” is about the life of Darlene Rameau, a former Belchertown resident, as related in a series of interviews with Orzechowski. It follows a similar pattern to that of Donald Vitkus, whose experience before, during, and after Belchertown, was the subject of Orzechowski’s first book, “You’ll like it Here.”

In each case, Orzechowski, a former COFAR Board member, has written the life story of a person who spent most of their childhood at the Belchertown school. When Donald was first sent there in the 1950s, and Darlene in the 1960s, that institution, like a number of others in Massachusetts, was a literal warehouse of abuse and neglect.
It is important to understand that the type of institution that Orzechowski describes in both of his books no longer exists today. Starting in the mid-1970s, while Darlene was still at Belchertown but Donald had long since left it, major upgrades in care and conditions began to be implemented at that and other similar institutions in Massachusetts. These changes were the result of a class action lawsuit first brought by Benjamin Ricci, the father of a former Belchertown resident.
The upgrades were overseen by U.S. District Court Judge Joseph L. Tauro. By the time Tauro disengaged from his oversight of the case in 1993, he wrote that the improvements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
As Orzechowski notes, Darlene became aware while she was still at Belchertown of the impact of Tauro’s involvement. Suddenly, and seemingly in one day, new, kinder staff appeared. Restrictions and beatings ended, Darlene says. But those changes still took many years to be fully implemented.
In 1996, Belchertown was closed for good. Today, only two large congregate care facilities remain in Massachusetts — the Wrentham Developmental Center and the Hogan Regional Center. Both centers must meet strict federal standards for care and staffing that were made possible by the federal litigation in Massachusetts and in other states starting in the 1970s.
At Belchertown, Darlene was a keen observer of nonstop human suffering, of wards filled with naked, neglected children, and reeking of urine and feces and infested with insects.
As was the case with Donald Vitkus’s story, much of the story about Darlene is about her attempts to cope in the “real world,” after having been discharged from Belchertown. For both Donald and Darlene, the transition was filled with trials and setbacks. Belchertown continued to affect both of their lives in sometimes tragic ways.
“Becoming Darlene” is a true story, but it reads like a novel. It is a page turner. It is at turns disturbing and heart breaking. But as with Orzechowski’s first book, one finishes this second book with a feeling of gratitude for Darlene and for the triumph of her spirit.
Update on our efforts to advocate for families in probate court
We reported last month about our efforts to help family members of persons with intellectual and developmental disabilities who have lost their guardianships and have found themselves legally outgunned in probate court.
In many cases, families can’t afford attorneys whose fees can run into the tens of thousands of dollars.
Even family members that do go into probate court with attorneys often feel outnumbered by the personnel arrayed against them there. Those opponents may not only include the attorney or attorneys for the Department of Developmental Services (DDS), but, in many cases, both the state-funded guardian appointed to replace the family member, and the state-funded attorney appointed to represent the intellectually disabled client.
In some cases, even the guardian ad litem (GAL), an attorney appointed to independently advise the judge, may take what appears to be a position against the family. We have seen cases before involving biased GALs.
In two cases in which we are currently involved, the GALs appear to have sided with DDS and with the state-appointed guardians and attorneys in seeking to remove the parents’ guardianships.
Probate judges open to allowing parents’ advocate to attend sessions
Last month, I contacted probate court clerks’ offices in Worcester and Woburn to see whether I could attend court sessions on behalf of the parents in those two cases. I received conflicting answers from the offices as to whether I, as a non-attorney, could appear as an advocate in the sessions.
However, when I did appear in court in those cases, the judge allowed me, in each case, to stay and stand at the counsel table alongside a mother who is seeking to regain her guardianship of her son.
In one of the two cases last month, Middlesex Probate Judge Thomas Barbar allowed me to speak on behalf of the mother, and then suggested that I “work with” her attorney as an advocate for her. It was encouraging, although it wasn’t quite clear whether I will be allowed to continue to address the judge directly in that case.
In the other case, Worcester Probate Judge Kathryn Bailey said she would allow me to be called as a witness for that mother when her case goes to trial, tentatively in February.
I came away from both sessions with a sense that my attending as an advocate from COFAR at least provided some independent weight to both parents’ positions before the court. Both sets of family members seemed to feel that way as well.
But the jury (no pun intended) may still be out on how effective a courtroom advocate, who is not an attorney, can be, and, perhaps ironically, whether I would be allowed to participate as an advocate if the person I am supporting does not have an attorney.
In that case, it seems possible that I might be seen as acting as the family member’s attorney, which would be illegal. I may, in those cases, only be allowed to attend the court session, and perhaps not speak.
A number of years ago, I tried to attend a probate court session in support of Stan McDonald, who had been seeking for years to regain guardianship of his intellectually disabled son. That case had been impounded, meaning the entire record was sealed from public disclosure, so the judge wouldn’t even let me in the courtroom. That was even though a previous judge had let me attend a previous court session in Stan’s case.
Supreme Judicial Court ruling may support non-attorney advocacy
But even in an impounded case, it seems it may be possible for an outside advocate to be called as a witness for a family member. Even in cases in which the parent or family member doesn’t have an attorney, I think it may be possible to argue that an advocate who is a non-lawyer can intervene as an “interested person.”
In a case known as “Guardianship of B.V.G.,” the Massachusetts Judicial Supreme Court held in 2016 that the grandfather of a young, intellectually disabled woman had the right to intervene in a probate court proceeding in order to gain permission to communicate with her.
Even though the grandfather was not B.V.G.’s guardian and wasn’t an attorney, he was an “interested person” within the meaning of the state’s Uniform Probate Code, according to the SJC. As such, he had the right to intervene in the probate court proceeding in order to remove restrictions on his contact with his granddaughter.
The SJC noted that the Uniform Probate Code (which is contained in the state’s general laws) allows anyone defined as an “interested person” to intervene in a guardianship proceeding in probate court. The high court concluded that an individual can be considered an interested person under the Probate Code simply by being interested in an incapacitated person’s well-being. As such, the grandfather of B.V.G. was clearly an interested person, the high court concluded.
So, I think I could argue that I should be allowed to intervene as an advocate in guardianship cases, based on the argument that I am similarly interested in the wellbeing of the incapacitated client.
DDS objects to our submission of information to the judge
In the two ongoing cases, I submitted written reports to the judges on behalf of the mothers, arguing for the return of their guardianships. It’s not clear if those reports have been accepted by the judges for consideration. In submitting the reports, I applied to “present information” to each judge, using a probate court application form that doesn’t specify that the presenter must be an attorney.
The application form further states that the “attached written statement (of information) is not evidence and that (the applicant) may be requested to testify at Court.”
However, in the Worcester Probate Court hearing, the DDS attorney filed a motion objecting to my submission of information in the case. John Geenty Jr., a DDS assistant general counsel, asserted in his motion that I have “no expertise”; that I have “no first-hand knowledge of the evidence” in the case, and that I was “trying to provide legal representation without a law license.”
During the court session, Judge Bailey allowed me to respond verbally to Attorney Geenty’s assertions. I noted that I have had more than 20 years’ experience in analyzing guardian cases and advising families and guardians in those matters, and that I was not claiming to be an attorney. The judge didn’t contradict me, and then said she would allow me to be called as a witness for the mother. As noted, it is not clear that the judge will consider the information that I submitted.
In the second case in Middlesex Probate Court, I submitted a rebuttal to the Guardian ad Litem’s report in that case, which had found the mother unfit to remain as her son’s guardian. I argued that the GAL’s report was deficient in not having included any interviews of clinicians or other witnesses who were supportive of the mother. As noted, it isn’t clear yet whether the judge in that case will take my report into consideration.
Difficulties in getting legal representation
We are, meanwhile, exploring other options for families such as contacting attorneys that provide pro bono representation.
As we previously reported, we have been trying to help a DDS client who told us she had been placed involuntarily under the guardianship of a DDS-funded provider agency. In that case, the client had asked that a longtime friend and former caregiver of hers become her guardian.
However, in December 2022, the Bristol Probate and Family Court appointed the Cooperative for Human Services, a corporate DDS provider, as the client’s guardian. The Cooperative has reportedly assigned an employee of the organization to provide guardianship services to the client, but the client told us she doesn’t even know who that appointed guardian is and has never met her.
Last month, I emailed four legal advocacy organizations to request that they represent the client in getting the guardian she wants.
I did receive a response on Wednesday (November 6) from the executive director of the Easthampton-based Center for Public Representation (CPR), who expressed interest in meeting with the client and “exploring the kind of help she is seeking.” We are trying to arrange that meeting now.
Two other legal advocacy organizations — the Boston-based Disability Law Center (DLC) and Brockton-based South Coastal Counties Legal Services — stated that they either don’t or can’t handle guardianship cases, while a third — the National Center on Law and Elder Rights — hasn’t responded to us.
As we stated before, the DDS-probate court system appears to be broken in that it doesn’t respond well to families of DDS clients. It particularly doesn’t respond well to families that aren’t represented by attorneys. But we are hopeful that there are other ways in which we can help.
If anyone has any additional insights into these matters, please feel free to share them with us.
Federal IG report finds safety deficiencies at the Wrentham and Hogan Centers, but misses the big issue – What about the group homes?
A federal investigative agency has reported deficiencies in safety and emergency preparedness in Massachusetts’ two developmental centers for persons with intellectual and developmental disabilities.
The October 2024 report by the Inspector General with the U.S. Department of Health and Human Services alleged 44 deficiencies related to life safety and emergency preparedness at the Wrentham Developmental Center and the Hogan Regional Center.
The IG’s report, however, raises a number of questions, in our view. First, will the IG similarly examine safety policies in the much larger, corporate-run group home network in Massachusetts?
The number of privatized, yet state-funded group homes has grown exponentially as developmental centers, also known as Intermediate Care Facilities (ICFs), have been closed over the past decade.
Secondly, why did the IG not address the quality of care in the ICFs and the group homes? It is in the group home system today that the most serious problems of abuse and neglect are endemic.
Thirdly, why not investigate the lack of access to ICFs for people needing residential care, and the misguided efforts to close them?
Finally, how serious were the safety deficiencies at Wrentham and Hogan that the IG’s report identified? The report did not appear to provide sufficient detail to answer that question.
No discussion of seriousness of deficiencies
The IG report stated that as a result of the deficiencies, “the health and safety of residents, staff, and visitors at the two ICFs are at an increased risk of injury or death during a fire or other emergency.” The question is how much of an increased risk?
The deficiencies included such things as fire extinguishers that had not been inspected on a monthly basis; placement of oxygen cylinders in hazardous storage areas; exits in some buildings that were obstructed, sprinkler heads that were “blocked or obstructed” in some instances; portable space heaters that were improperly placed in residential areas; and holes in some ceilings and walls.
While some of those things sound potentially serious, a problem with the report was that it gave few if any details about them. For instance, what else was contained in the hazardous storage areas? How were the sprinkler heads blocked, and how many were blocked?
Strangely, the report never named either of the two Massachusetts ICFs, so it never specified which of the deficiencies were found in which of the two facilities.
The report noted that the portable fire extinguishers that had not been inspected monthly were found in one of the ICFs, although, as noted neither of the ICFs was named in the report. The report also didn’t say how many fire extinguishers in that facility had not been inspected, or how many months had gone by without inspections.
The report didn’t explain what it meant by blocked or obstructed sprinkler heads. In a photograph that was included in the report, it didn’t appear that the sprinkler in the photo was broken, but rather that the sprinkler had been installed in the ceiling of a closet, and that it was partially blocked by objects placed underneath it.
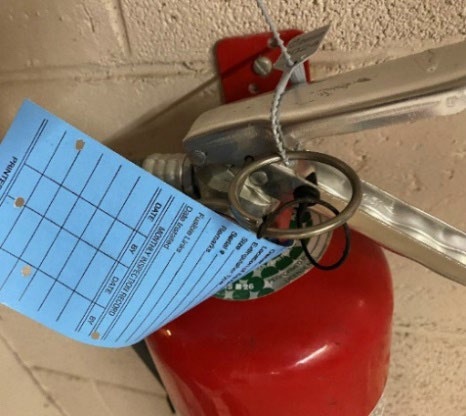
Fire extinguisher with the monthly inspection tag not filled out. From IG report.
Also, many of the deficiencies involved failures to provide documentation. It’s hard to judge the seriousness of some of those findings, particularly because some of them seemed ambiguous. For instance, the report stated that, “Both ICFs did not have a formal communications plan that was updated at least every 2 years.”
What is a “formal” plan versus an informal plan, and does this mean the facilities had no plan at all? There was no explanation or details provided about that.
The report also stated that “one ICF did not have policies and procedures that address the facility’s emergency preparedness plan and identified hazards within the facility’s risk assessment.”
What exactly does that mean? Did it mean that that particular ICF did have an emergency preparedness plan, but didn’t have “policies and procedures that address” the plan? Don’t plans refer to policies and procedures?
Robert Goldstein, commissioner of the Massachusetts Department of Health, which inspects the ICFs annually, responded to the IG report, stating that the majority of the audit findings were “immediately corrected” by the staff of each of the facilities.

Deficiency identified as “obstructed sprinkler head.” From IG report.
It’s also not clear to us why the federal IG singled out the Wrentham and Hogan Centers for this inspection report. We understand that the IG conducts investigations when it is requested to do so by an elected official. Who would have wanted such an investigation done just about the Wrentham and Hogan Centers, and why?
The report itself noted that there are approximately 5,400 Medicaid-certified ICFs in the U.S., and that Massachusetts has just two of them. Four others were closed in this state between 2012 and 2015.
The IG noted that its report on the Massachusetts ICFs is the first in a planned series of audits that will similarly assess compliance with federal “life safety, emergency preparedness, and infection control requirements for ICFs.” So, it does appear that the IG will be conducting similar searches for fire extinguishers without inspection tags and blocked exits in ICFs in other states.
Hopefully, those coming reports will provide more explanatory details about the deficiencies that will surely be found. It would also be nice if the IG were to expand the scope of its investigations to include the broader questions why ICFs around the country are being closed, and what the quality of care is in the group home systems.
We are not holding our breath in anticipation of those broader investigations.
High-profile legal advocacy organization won’t help DDS families in guardianship cases
We have been dealing lately with several cases in which family members of persons with intellectual and developmental disabilities have lost their guardianships and have embarked on difficult quests to obtain legal representation in probate court.
For many, getting an attorney is prohibitively expensive. Even for those who can afford it, finding attorneys with experience in going up against the Department of Developmental Services (DDS) can be frustrating.
For some time now, we have been exploring options for those families who find themselves pitted against both DDS and the probate court system.
One lesson we’ve learned so far is perhaps not to rely on entities that bill themselves as legal advocacy organizations that fight for rights under guardianship.
A case in point concerns two Massachusetts-based and one national legal advocacy organizations that we recently contacted to request free legal help for a woman who receives DDS services and who told us she was placed involuntarily under the guardianship of a DDS provider.
Earlier this month, I emailed the Boston-based Disability Law Center (DLC), the Easthampton-based Center for Public Representation (CPR), and the National Center on Law and Elder Rights (NCLER) to ask whether any of them would represent this person.
All three are legal organizations that maintain that they advocate for the rights of people with disabilities. The CPR and NCLER have so far not responded to me. The DLC did respond, saying they don’t actually handle guardianship cases.
I had emailed the DLC on October 3, the CPR on October 10, and the NCLER on October 17.
The DLC describes itself on its website as a part of “a national network of disability rights agencies investigating abuse and neglect and providing legal representation and other advocacy services to people with disabilities.”
We are, meanwhile, exploring other options for families such as contacting attorneys that provide pro bono representation. And we have begun examining the possibility of having non-attorneys represent family members as advocates in probate court.
Last week, I contacted probate court clerks’ offices in Worcester and Woburn to see whether I could attend court sessions on behalf of two different families that are currently caught up in guardianship battles in those courts. I received conflicting answers from those offices as to whether I, as a non-attorney, could attend those sessions.
Response from the Disability Law Center
As noted, I emailed the DLC on October 3, asking whether that agency might be able to provide legal assistance or representation to the woman who has been placed involuntarily under the guardianship of an organization funded by DDS.
I noted in my email that we understand that the DLC has advocated for the rights of persons under guardianship and for limitations on guardianships where possible. For example, an online DLC brochure on “self-determination” states that:
A person has the right to have the (probate) Court limit a guardianship as much as possible. A person under guardianship has the right to have a guardian who considers the person’s expressed preferences and acts in the person’s best interests. A person has the right to be present and participate in the guardianship hearing. This includes giving the Court evidence and asking questions. A person under guardianship has the right to ask the Court to remove the guardian. (our emphasis)
I stated in my email to the DLC that it appears that at least some of the woman’s rights, as enumerated by the DLC, are being violated under the current guardianship arrangement. She was placed under a full guardianship, yet the guardian is someone who does not appear to be considering her expressed preferences.
I’ll give the DLC some credit for having responded to me. On October 7, Nancy Murphy, the managing attorney for the DLC’s Intake Unit, wrote back to say that the DLC “does not handle guardianship cases.” She added that, “This is to avoid duplicating work that other organizations and the private bar do.” However, she didn’t identify any other such organizations.
Murphy added that, “Our focus areas allow us to better use our very limited resources on our core mission of monitoring and investigating abuse and neglect.”
The DLC has told us before about their limited resources even though they received some $4.3 million in federal, state, and other revenue in Fiscal Year 2023, according to the organization’s 2023 tax filing available on the ProPublica Nonprofit Explorer website.
I wrote back to Murphy, stating that it was disappointing to learn that the DLC does not handle guardianship cases and that such cases are not part of the DLC’s core mission. I noted that we would hope that the DLC recognizes that guardianship is central to the question of the quality of the care of individuals with intellectual and developmental disabilities.
I also pointed out that it appears that the DLC would have a role in implementing pending legislation, which would authorize “Supported Decision Making” (H.4924 and H.4949) as an alternative to guardianship in Massachusetts. The DLC wants to take on this role, as we understand it, because the DLC considers that guardianship “takes away an individual’s personal decision-making rights and responsibilities.”
Yet, I noted, when there is a clear case of an individual whose personal decision-making rights and responsibilities have been taken away by the appointment of a state-funded guardian, the DLC is not interested or has too little resources to advocate for that individual’s rights and responsibilities.
The Center for Public Representation
As noted, I requested legal assistance from the CPR for the DDS client on October 10, and have not received a response as of this date.
The CPR’s 2023 tax filing describes the organization as “providing legal assistance, counsel, and representation to institutionalized, low-income individuals with mental illness or other disabilities at no charge.” In the tax filing, the CPR describes its mission as seeking “to improve the quality of lives of people with mental illness and other disabilities through the systemic enforcement of their legal rights while promoting improvement in services for citizens with disabilities.”
According to the tax filing, the CPR received just over $1 million in revenue in 2023.
We have noted that the CPR’s website states that the organization has developed a partnership with more than a dozen law firms “to directly represent thousands of individuals with disabilities” on a pro bono basis. We will attempt to contact those organizations in coming weeks.
The National Center on Law and Elder Rights
The NCLER describes its mission on its website as providing “the legal services and aging and disability communities with the tools and resources they need to serve older adults with the greatest economic and social needs.”
I stated in my October 17 email to the NCLER that we understand the organization is dedicated to protecting and enhancing the rights of persons under guardianship. As the NCLER noted in a paper on guardianship, “When a person asks for the return of their rights (under guardianship), they very likely have the capacity to make choices—especially with appropriate supports.”
The NCLER appears to be a government organization and therefore doesn’t file a tax form, which would list its revenue. So, unfortunately, there appears to be no available information about that.
As we have seen repeatedly, people need legal representation when appearing in probate court, just as in any courtroom setting. Without it, they are hopelessly outgunned and outmaneuvered.
Unfortunately, the combined DDS and probate court system in Massachusetts won’t help families unless they have the money to hire experienced attorneys. Today, that combined system appears to be broken.
DDS provides heavily redacted documents concerning one-time calculation of vacancies in state-operated group homes
The Department of Developmental Services has provided us with almost completely redacted documents concerning a calculation it made that there were approximately 91 vacancies in its state-operated group homes as of June of 2023.
That month in 2023 was apparently the one and only time that DDS ever attempted to determine the number of vacancies in the homes. The Department, however, is either unable or does not want to explain how or even why the vacancy rate was calculated on that one occasion.
In July of this year, we reported that DDS had finally clarified, after we had filed an appeal for records from the Department, that it doesn’t track the number of vacancies in its state-operated group home network.
However, in September 2023, the Department stated that it could, in fact, provide us with the number of vacancies as of that one date. The vacancies were within a network of group homes that then had close to 1,000 residents. (As of this past June, the total number of residents had dropped to 986.)
About two months later in 2023, DDS stated that the number of 91 vacancies was only “an approximation” that had been determined in a one-time “exercise” that DDS employees had participated in. Since then, “no similar exercises have been conducted,” a DDS attorney stated.
That explanation, however, only appeared to raise the question why DDS attempted on one occasion, but never again, to determine the number of vacancies in its group-home network.
Even though thousands of people with intellectual and developmental disabilities are waiting for residential placements and other services from DDS, why would the Department not have a continuing interest in knowing whether its state-run network has available beds for them?
Based on those questions, we filed a new Public Records Request with DDS on July 12 of this year, seeking all documents relating to the Department’s exercise, which had resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.
We hoped some of those documents might shed light on why the exercise had been conducted.
In a response on August 9, DDS provided records that it described as “documents that DDS employees relied upon to identify the approximate number of state-operated group home vacancies as of June 30, 2023.”
However, the documents appeared to provide no information regarding the nature or scope of the exercise or the reasons for conducting it.
One of the documents provided, labeled “Southeastern Residential Services — 6/15/23 — Temporary Moves,” was filled with text boxes containing information that had been entirely blacked out. There was no readable information in the document other than the words “Medical Respite” below one of the redacted text boxes. I’ve reproduced that document here:
DDS document provided to us concerning group home vacancy calculation
Another heavily redacted document, labeled “Metro Residential Services Caseload List July 2023,” appeared to contain only the names and positions of DDS employees.
Another document, referred to as ‘Central West Region Vacancy Tracker,’ appeared to be an undated spreadsheet with columns containing the names and phone numbers of DDS employees.
There were approximately 70 listings of the word “vacancy” in a separate column in the spreadsheet that appeared to contain the redacted names of residents of group homes in that region. There was no apparent summary information in that or any of the other documents.
In particular, there was no reference in any of the documents to the total of 91 vacancies that the exercise reportedly identified. None of the documents contained any identifiable connection to the exercise or the subject of the exercise — the number of vacancies in the group homes.
As a result, we appealed on August 26 to the state supervisor of public records, asking that DDS be ordered to clarify whether it did or did not possess records that specifically described the nature or scope of the one-time, vacancy-determination exercise.
On September 6, the supervisor of public records stated that in a phone call between a staff attorney of the Public Records Division and an attorney for DDS that same day, “the Department confirmed that it provided all records responsive to (our) request.”
The public records supervisor added that, “The Department further confirmed that the exercise in question was an informal exercise that provided an estimate for vacancies, and that the records provided to (COFAR) were used in determining the approximate numbers.”
The supervisor, in other words, was satisfied with the Department’s response. Because the exercise was “informal,” whatever that means, DDS was apparently not required to maintain or provide any documents that might shed any light on it. Our appeal was denied.
As we’ve said before, the fact that the administration does not even track the vacancy rate in state-operated group homes is evidence, in our view, that the administration does not view state-run residential services as a viable option for waiting clients. DDS, in fact, is letting the state-run system die by attrition.
In light of all of that, we think it would be helpful to know why the Department decided at one point a few years ago to conduct an informal exercise to determine the approximate vacancy rate as of one particular date.
Was it because a number of DDS officials have been telling families, as we have heard, that there are no vacancies in state-operated group homes, and the Department had no idea if that information was correct? If so, the exercise showed that there were, in fact, vacancies in the residences.
Unfortunately, it doesn’t appear that the fact that the exercise indicated the existence of an approximately 10 percent vacancy rate in the state-run homes has persuaded the Department to admit more people to those residences.
So why did DDS conduct that one-time exercise? It appears we may never know the answer to that question.
Key lawmaker and disability advocates acknowledge serious problem with state’s Abuser Registry
The original sponsor of the legislation that established an “Abuser Registry” in Massachusetts said it may be time to “fine-tune” the legislation in light our recent report that a potentially significant number of abusive care providers are able to avoid placement of their names in the Registry.
The Registry, which is managed by the Disabled Persons Protection Commission (DPPC), is intended to prevent care providers who have abused persons with intellectual and developmental disabilities (I/DD) from continuing to work for the Department of Developmental Services (DDS) or for any agency funded by DDS.
News Service alone discusses COFAR report that Registry has a possible loophole
The remarks of state Senator Patrick O’Connor, the sponsor of the Registry legislation, and other disability advocates about our findings were reported late last month by the State House News Service. The News Service covers political and governmental issues and events involving the state Legislature and the state administration.
The Registry, which was created under “Nicky’s Law,” has now been in operation for just over three years.
In July, we reported on DPPC data concerning substantiated abuse allegations against care providers since the Registry’s inception. We found that in only a minority of those cases did the DPPC conclude that those persons’ names should be placed in the Registry.
Under Nicky’s Law, care providers, who have been found after DPPC or DDS investigations to have committed abuse, can petition the DPPC to overturn both their abuse substantiations and the placement of their names in the Registry.
We found that of 161 petition decisions, the DPPC affirmed abuse in 132 cases, and reversed abuse substantiations in just 29 cases.
However, even among those 132 cases in which abuse was affirmed through the petition process, only 47 — or 36% — of those providers ended up in the Registry. In contrast, in 85 — or 64% — of those cases, the DPPC determined the abuse was not “Registrable.”
The fact that abuse was not Registrable in most of the substantiated abuse cases appears to be due to a possible loophole in the Registry regulations. The loophole allows DPPC to conclude that an abuse incident was “isolated” and “unlikely to reoccur,” or that the provider is “fit” to continue to provide services to people with I/DD.
As I noted to the State House News Service reporter who had interviewed me for her article, it is difficult, due to the confidentiality of DPPC investigations, to understand the logic behind the DPPC’s decision-making. There seems to be a built-in incentive in the regulations to care providers to petition to overturn any abuse substantiations against them by the DPPC or DDS.
DLC says they have concerns based on our report
The News Service reported that the Disability Law Center (DLC), a federally funded legal advocacy organization in Massachusetts, had previously questioned whether the Abuser Registry regulations were too lenient toward abusive care providers, and whether the regulations may have even gone beyond the scope of Nicky’s Law.
The News Service article quotes Rick Glassman of the Disability Law Center as saying COFAR’s findings are “concerning” to him.
Nicky’s Law sponsor says ‘time to fine-tune’ law
State Senator Patrick O’Connor, the original sponsor of the legislation that led to Nicky’s law, told the News Service that he is worried by our findings and that it “may be time to fine-tune Nicky’s Law.” O’Connor said he intends “to learn more from DPPC about cases in which providers are permitted to stay employed despite committing abuse.
“It’s definitely a cause for concern,” O’Connor added, “and I will for sure be calling for meetings with DPPC to try to get specific examples of why this is happening on both ends to try to figure out how we can make the law better.”
Legislator says COFAR is “inaccurate,” but gives no specifics
State Representative Jay Livingstone, House chair of the Legislature’s Committee on Children, Families and Persons with Disabilities, defended the impact of the Registry to the News Service. Livingstone also alleged that “COFAR’s information is typically not accurate.” He provided no specifics in the News Service article to support that claim.
A month prior to the publication of the News Service article, I sent an email to Livingstone and to State Senator Robyn Kennedy, Senate chair of the Children and Families Committee, and close to 50 other legislators, calling their attention to our report about the Registry.
I have not received a response to date from any of them. Livingston, in particular, didn’t respond to my email. If he has questions about the accuracy of our report, he hasn’t let us know them.
Family member dissatisfied with DPPC investigations
One family member of an individual with I/DD was quoted in the News Service article as saying the DPPC’s investigative process in general isn’t working.
“There’s a lot of cases where these people (abuse investigators) are not doing their jobs,” Jeanne Cappuccio, whose daughter has an intellectual disability, said. “You complain, you file a complaint and it gets screened out. It reinforces that … it’s OK to treat people with disrespect, and it’s OK to be abusive, and it’s OK to mistreat.”
DPPC makes questionable claim about Registry placements
In comments to the News Service, Andrew Levrault, DPPC’s deputy general counsel, defended the Registry’s record and regulations. “We think it (the Registry) has really lived up to its goal to bridge that gap between individuals who would have otherwise had a clean CORI (Criminal Offender Record Information)…(and are now subject to a process) which prevents them from working in the field where they really shouldn’t be because of past abusive conduct,” he said.
Levrault said the instances in which individuals are kept off the Registry include cases in which there is “an opportunity for re-training, including for those who make medication errors.” He maintained that, “In cases of intentional physical or sexual abuse, those providers will be put on the Registry.”
It does not appear, however, that there is anything in the Registry regulations that requires the DPPC to place care providers’ names in the Registry in all cases in which the agency has affirmed allegations of intentional physical or sexual abuse against them.
Our recommendations
We have made a number of recommendations for tightening the Registry regulations, including requiring the DPPC to consider several factors listed in the regulations for determining whether a substantiated incident of abuse really is isolated and whether the care provider really is fit to continue to provide services.
Right now, the regulations say only that the DPPC “may” consider factors such as previous incidents of abuse and the provider’s previous work history.
We also think DPPC should be required to consider impact statements from the victims and their families when considering petitions by care providers to avoid placement in the Registry.
Also, the regulations should explicitly require that the DPPC place care providers in the Registry in all cases in which the agency has affirmed allegations of intentional physical or sexual abuse. Levrault claimed that his already happening, but the regulations don’t appear to support his statement.
The question that remains is how can we ensure that needed changes will happen?
At least some of the lawmakers and advocates interviewed by the State House News Service said the right things about the need to look into our concerns and fine-tune the law.
But at this point, there is little to hold lawmakers and other officials accountable or to ensure that they follow through on their promises.
It is becoming clearer every day that the media is no longer interested in playing that role. The media and our political and governmental leaders are today all part of the same club.
Supported Decision Making bills give key role to state’s banking lobby
A redrafted version of Supported Decision Making (SDM) legislation, which appears to be close to enactment in the state Legislature, would give a major banking lobbying organization a key role in implementing SDM in Massachusetts.
The latest SDM bills (H.4924 and H.4949), which are actually identical drafts, have been sent to the House Rules and House Ways and Means Committees respectively, and either one of those bills appears to be a step away from enactment on the House and Senate floors.
Each bill specifies in the latest redraft that the Massachusetts Bankers Association would be involved both in developing a training program on the rights and obligations of SDM supporters, and in studying the feasibility of a state registry of all existing SDM agreements in the state.
SDM appears in our view to hold a potential to overturn guardianships of persons with intellectual and developmental disabilities (I/DD).
The legislation would authorize written agreements to replace guardians of persons with I/DD with informal teams of “supporters” or advisors. The supporters would provide those individuals with “decision-making assistance” about their care and finances.
On August 15, I sent emails to the Senate president, House speaker, and chairs of the Children, Families, and Persons with Disabilities Committee, Judiciary Committee, Rules Committee, and House Ways and Means Committee, expressing concern that the redrafted legislation contains a number of flawed provisions.
In a subsequent email last week (August 22), I sent a follow-up email to the co-chairs of the Children and Families Committee, arguing that the legislation also fails to address a potential conflict of interest involving the Mass. Bankers Association.
We maintain that the redrafted legislation would also introduce conflicts between SDM supporters and guardians; does not direct the probate court to resolve those conflicts; and does not direct the Disabled Persons Protection Commission (DPPC) to enforce a provision against coercion in signing SDM agreements. The legislation also does not provide any means of enforcing a new provision against conflicts of interest held by SDM supporters.

Mass. Bankers role
In an emailed response on August 20 to my first email, State Representative Jay Livingstone, House chair of the Children and Families Committee, maintained that the Mass. Bankers Association was added to the legislation because, “Financial institutions may be requested to accept the (SDM) agreements. The Mass. Bankers Association’s expertise may be helpful to represent those interests,” he added.
The Bankers Association is one of five non-governmental organizations given roles by the legislation in developing SDM, including the Arc of Massachusetts, the Disability Law Center, the Mass. Medical Society, and the Mass. Health and Hospital Association.
Livingstone also responded to a number of my other concerns, as I’ll discuss below. Unfortunately, our concerns about the legislation have not been assuaged.
With regard to the Mass. Bankers Association, we are concerned that banks and other financial organizations may have interests in financing or investing in the development of care facilities or corporate provider organizations, and that those financial interests could then assume a prominent role in SDM training programs or even agreements under the legislation. There is no provision in the legislation to prevent conflicts of interest involving banking, investment firms, or other financial interests in SDM arrangements.
For instance, the Mass. Bankers Association listed (H.4977), which will provide millions of dollars to finance Accessory Dwelling Units (ADUs), as a bill it was tracking this year. The bill has since been signed into law. The Arc of Massachusetts describes the development of ADUs as “one of its priorities over four sessions.” ADUs may well be a subject of consideration by SDM supporters.
We think it would be more appropriate to select a neutral individual who might be a faculty member of a university business school or economics department as an SDM training consultant, rather than selecting a member of the Mass. Bankers Association.
Major changes to Uniform Probate Code
Both SDM bills (H.4294 and H.4949) were reported favorably late last month by the Children, Families, and Persons with Disabilities Committee and are now in the House Rules and House Ways and Means Committees respectively. This legislation would make significant changes to the Massachusetts Uniform Probate Code (M.G.L. c. 190B), and yet the legislation has not been voted on favorably by the Judiciary Committee.
We are concerned that this redrafted legislation, which has not had a public hearing, could be enacted without a roll call vote in informal House and Senate sessions at any time.
Sets up conflict between SDM supporters and families and guardians
Under the redrafted legislation, it appears that an individual under a full guardianship could also sign an SDM agreement. In that case, we asked the legislators, what would the resolution process be if there were a dispute between the SDM team and the guardian?
In his August 20 response, Rep. Livingstone stated that, “Once an individual becomes subject to a full or plenary guardianship, they could not sign an SDM agreement. An SDM agreement is an alternative to guardianship.“
But that does not appear to be the case. There doesn’t appear to be any language in the legislation that would preclude signing an SDM agreement if there is a full or plenary guardianship.
At another point in his response, in fact, Rep. Livingstone stated that, “If the (probate) court that created the guardianship left a SDM agreement in place in whole or in part, the court should work out the roles and responsibilities of each. If there was a conflict (between a guardian and SDM supporters), the parties could go back to court to resolve the issues if they could not work them out themselves.”
However, as I replied to Livingstone, the legislation doesn’t require the court to work out the roles and responsibilities of each party. Further, having the parties “go back to court to resolve the issues” would automatically place the guardian at a disadvantage, in our view, if, as is likely, the supporters would outnumber the guardian in any court proceeding.
Questionable access to medical records
The legislation states that an intellectually disabled “decision maker” may provide a supporter with access to their medical records, including confidential health information, and with access to psychological, financial and other records. The legislation later states that the SDM agreement must “specifically reference” a supporter’s access to medical records etc.
To us, this raises the question: If the decision maker is under a full or plenary guardianship, why would it be necessary for SDM supporters to have access to these records unless the supporters’ authority were equal or greater than the guardian’s authority?
Questions about confidentiality
In granting access to confidential records to SDM supporters, the legislation states that a supporter “shall keep confidential any information obtained in the process of assisting the decision-maker.”
To us, this raises the question: Does this provision require a supporter to decline to disclose such information to either the guardian or to other supporters?
Livingstone responded that an individual supporter would be required to keep such information completely confidential “unless directed to (reveal it) by the decision-maker.”
This is a particularly troubling provision in that it could be used by SDM supporters to marginalize family members or guardians by keeping them in the dark regarding important aspects of an individual’s health or medical care.
Weak conflict of interest provision
The redrafted legislation states that a supporter “shall not participate in any life decision in which they have a conflict of interest.” This includes, the legislation states, “any decision in which the supporter, his or her immediate family or partner, a business organization in which he or she is serving as officer, director, trustee, partner or employee has a financial interest or other direct and substantial interest in the outcome.”
Such a provision is better than nothing, which was the case under previous versions of the SDM legislation. But even under this provision, an employee of a provider serving the individual could nevertheless serve as an SDM supporter and participate in life decisions in which the provider doesn’t have a direct financial interest.
In our view, this provision does not fully protect individuals with I/DD against conflicts of interest. The legislation doesn’t provide for enforcement of this provision.
Also, whether a specific conflict of interest exists in a particular matter could be open to interpretation. We believe employees of providers that offer services to SDM “decision makers” should not be allowed to participate in SDM agreements period.
No enforcement of anti-coercion provision
The legislation states that “evidence of undue influence or coercion in the creation or signing of a supported decision-making agreement shall render the supported decision-making agreement invalid.”
But who would determine whether there was evidence of this?
Livingstone responded that, “An interested party would need to report alleged undue influence or coercion in an SDM agreement’s creation or signing to the Disabled Persons Protection Commission, the Elder Abuse Prevention Hotline or the court for any further action.”
The problem is the legislation does not state that the Disabled Persons Protection Commission (DPPC) should investigate allegations of undue influence or coercion in the signing of an SDM agreement.
The DPPC’s enabling statute (M.G.L. c. 19C) requires the DPPC to investigate allegations of abuse or neglect that causes significant physical or emotional injury. The DPPC’s regulations (118 CMR 2.02) state that serious emotional injury can result from coercion; but it is unlikely that the regulations contemplate the type of coercion referred to in the SDM legislation.
The often subtle coercion that would be involved in the signing of an SDM agreement would be unlikely, or at least would not necessarily result in emotional distress to the signer. As a result, even if such an allegation of coercion was made to the DPPC, it isn’t clear that the agency would be statutorily required or authorized to investigate it.
Similarly, there is no way to enforce other feel-good provisions in the legislation, such as one stating that a supporter must “respect the values, beliefs, and preferences of the decision-maker, act honestly, diligently, and in good faith; act within the scope identified by the decision-maker, (and) support and implement the direction, will, and preferences of the decision-maker.”
Termination provision unworkable for persons who are unable to communicate
The legislation states that the decision-maker “may amend or terminate a supported decision-making agreement at any time…”
But what would the process be for termination if the decision-maker were unable to communicate?
Livingstone stated that, “If the decision-maker became incapacitated while the SDM agreement was valid, the bill provides that the agreement would be terminated.”
The problem is that “incapacitation” is not defined in the legislation. Any individual under guardianship is considered under the Probate Code to be incapacitated (see M.G.L. c. 190B, s. 5-303). This, in fact, goes to a key problem we have repeatedly identified with the SDM legislation. The legislation does not provide a standard level of capacity of an individual below which SDM would not be feasible.
Additional burden of proof
As we have repeatedly pointed out to the legislators, all of the versions of the SDM legislation would add to the burden of proof that a petitioner already faces in probate court in order to become a guardian. Thus, we think that this legislation may predispose probate court judges to deny guardianship petitions in favor of SDM agreements.
The legislation specifically would require anyone petitioning in probate court to become a guardian to state why a more limited guardianship or an SDM agreement was “inappropriate.”
Perhaps the major concern we have also repeatedly raised about the SDM legislation is, as noted, that it doesn’t specify a level of functioning or decision-making capacity below which an SDM arrangement would not be considered feasible. There is no consideration in the legislation as to whether persons with low levels of cognitive functioning are capable of making and appreciating life-altering decisions.
As a result, under the SDM legislation, anyone can sign an SDM agreement, no matter how low their cognitive functioning might be, and then be labeled the “decision maker” in that agreement. That aspect of the legislation alone shows that it is not based in reality.
For all of these reasons, we hope lawmakers do not enact this legislation in the remainder of the current legislative session. SDM may work for some high-functioning individuals. But it needs to go back to the drawing board in Massachusetts.
SDM legislation once again close to final passage in questionable procedural move
Legislation that would authorize Supported Decision Making (SDM) as an alternative to guardianship of persons with intellectual and developmental disabilities (I/DD) in Massachusetts is once again close to final passage in the state Legislature.
This time, the circumstances surrounding the legislative process involving the bill are particularly troubling.
SDM involves enacting written agreements to replace guardians of persons with I/DD with informal teams of “supporters” or advisors. The supporters then provide those individuals with “decision-making assistance” about their care and finances.
On July 29, with two days to go in the formal 193rd legislative session, the Children, Families, and Persons with Disabilities Committee referred two newly revised, identical SDM bills — H.4924 and H.4949 — to the Rules Committee.
Although the 193rd legislative session is now formally over, we understand that either or both of the redrafted bills can be referred at any time until the end of the year to either the House or Senate floor for final enactment. Once referred, the legislation could be enacted in “informal sessions” unless there is an objection from a lawmaker.
During informal sessions, there are usually only a few legislators present, and no roll call votes are taken.
Yet, the redrafted legislation appears to make major changes to the Massachusetts Uniform Probate Code (M.G.L. c. 190B), a set of provisions governing the probate court system.
Prior to July 29, the Children and Families Committee had delayed taking action on an earlier version of the legislation for more than a year.
In our view, guardianship is the most important legal protection family members have to ensure adequate care and services for their loved ones with I/DD.
In an email I sent last week (August 8) to key legislators, I said that legislation imposing arrangements that weaken guardianship also weakens the decision-making rights of families.
I noted that the redrafted legislation doesn’t address specifc oncerns we had previously raised about SDM with those legislators. While SDM may be appropriate for high-functioning individuals, it may expose lower functioning persons to financial exploitation and reduce the input family members have over their care and services.
Arrangements that weaken guardianship further violate the spirit of the federal Developmental Disabilities Assistance and Bill of Rights Act, which states that family members of persons with I/DD are the “primary decision-makers” in their care and services.
No vote by the Judiciary Committee
In addition to the lack of a roll call vote if the redrafted SDM bills are now taken up in the House or Senate, it appears the bills have not been voted on by the Legislature’s Judiciary Committee. The Judiciary Committee has jurisdiction over legislation pertaining to the courts in Massachusetts and the Probate Code.
Also, there has been no public hearing on the redrafted legislation, which appears to be substantially different from an earlier version of the measure. The Children and Families Committee did hold a public hearing on the earlier version in September 2023.
A staff member of the Children and Families Committee told us that the Judiciary Committee was involved with the Children and Families Committee in drafting H.4924 and H.4949. However, there is no indication on the Legislature’s website that the redrafted legislation was actually voted on favorably by the Judiciary Committee.
Committee co-chair says “plenty of time” for our concerns to be considered
In a response to my August 8 email, Representative Jay Livingstone, House chair of the Children and Families Committee, maintained that, “There is plenty of time for this bill and your (COFAR’s) comments to be considered.”
We hope that is the case, although we had raised concerns about the SDM legislation with the Children and Families Committee last year.
Livingstone also said there was “still a possibility” of a roll call vote on the redrafted legislation this year because the Senate president and House speaker have agreed to call a special session at some point before the end of the year. Nevertheless, it isn’t clear whether the SDM bills would be taken up during that special session if they are enacted this year.
Livingstone further acknowledged that the Judiciary Committee has not voted on either H.4924 or H.4949.
Redrafted legislation raises questions
In one respect, we think the redrafted legislation might be better than the earlier version of the measure.
Apparently based on a concern we raised last year, the redrafted legislation (H.4924 and H.4949) would prohibit an SDM supporter from having a conflict of interest involving their employer.
However, it isn’t clear that the redrafted legislation would completely rule out human services provider employees from serving as SDM supporters. Those individuals would be prohibited only from participating in specific “life decisions” in which they or their employers had a financial interest.
Moreover, we think the redrafted legislation as a whole would still weaken guardianship because it would set SDM up in the Probate Code as an alternative to guardianship. Under the redrafted legislation, anyone petitioning in probate court to become a guardian would have to state why either a more limited guardianship or an SDM agreement was “inappropriate.”
That SDM provision would add to the burden of proof that a petitioner already faces in probate court in order to become a guardian. Yet, an SDM agreement itself apparently doesn’t require similar court approval. Overall, we think that this legislation may predispose probate court judges to deny guardianship petitions in favor of SDM agreements.
Another concern we have about the SDM legislation is that it doesn’t specify a level of functioning and decision-making capacity below which an SDM arrangement would not be considered feasible. There is no consideration in the legislation as to whether persons with low levels of cognitive functioning are capable of making and appreciating life-altering decisions.
For all of those reasons, we think this is not the time to enact this legislation. We hope legislative leaders will recognize the need to go back to the drawing board in the next legislative session, and address the concerns we have raised.
Healey targets state-operated group homes for cut in proposed FY ’25 funding
In signing a $58 billion state budget this week for the newly begun Fiscal Year 2025, Governor Maura Healey has cut $401,000 in proposed funding for state-operated group homes.
That was one of two cuts that Healey made in Department of Developmental Services (DDS) line items in the budget plan sent to her by the Legislature. The governor also cut $1 million in proposed funding for the Autism Division.
Left untouched by Healey was $1.69 billion in funding for DDS’s separate corporate provider-run group home line item, and $390 million in a separate reserve fund for the providers.
Healey’s cut in proposed funding for the state-operated group homes still allows for a 4% increase in the funding of that line item over the previous fiscal year. But that increase will now be $2.4 million less than the increase the governor herself had proposed when she submitted her budget to the Legislature in January.
The Legislature itself had cut Healey’s proposed funding of the state-operated group homes by $2 million. Healey has now reduced that amount by an additional $401,385.
It’s unclear what the impact will be of the lowered funding increase for the state-run homes and whether it might result in cuts in staffing. It is also unclear why Healey targeted just the state-operated group homes and the Autism Division for cuts out of DDS’s total $2.9 billion budget.
Healey stated with regard to the state-operated group home line item cut that she was reducing it to $330.7 million, which is “the amount projected to be necessary.” In signing the budget, she said that, “Due to operational efficiencies, savings will be achieved (in state-operated group homes) without impacting services to clients.”
Healey’s statement, however, did not specify what those operational efficiencies were.
We have long raised concerns that a succession of administrations has been allowing the state-operated group home system to die by attrition.
We reported yesterday, in fact, that not only do there appear to be vacancies in the state-run group home system, but DDS has now acknowledged that it doesn’t keep track of those vacancies. All of these things appear to be signs that the administration does not view state-run residential services as a viable option for thousands of waiting clients.
Healey has reportedly cited “fiscal prudence” as the reason for making a total of $317 million in cuts in the Fiscal 2025 budget prior to signing it. At the same time, however, her budget increases spending overall by 3.1% over last year’s budget.
The Boston Globe reported that Healey also cut $192 million from the MassHealth managed care program, “due, in part, to ‘anticipated utilization,’ or how much the state expects people to make use of the services.”
DDS finally acknowledges it doesn’t keep track of whether there are vacancies in state-operated group homes
For almost a year, we had been trying to clarify with the Department of Developmental Services (DDS) whether there are – and we suspect there are – continuing vacancies in the Department’s network of state-operated group homes.
Finally, in a clarification issued earlier this month in an appeal we filed with the state public records supervisor, a DDS attorney stated flatly that, “DDS does not track state-operated group home vacancies.”
While it’s helpful to know it would be a waste of time to continue to ask DDS for information it clearly says it doesn’t have, the Department’s clarification still raises a number of questions. First, why doesn’t DDS track what appears to be basic information about its state-operated group home network?
Secondly, even though thousands of people with intellectual and developmental disabilities are waiting for residential placements and other services from DDS, why would the Department not have any interest in knowing whether its state-run network has available beds for them?
One troubling answer to those questions is that the Healey administration does not view state-run residential services as a viable option for those thousands of waiting clients. This is borne out by evidence that DDS is letting the state-run system die by attrition.
DDS does not generally inform people seeking residential placements of the existence either of its network of state-run group homes or of its two remaining state-run congregate residential centers – the Wrentham Developmental Center and the Hogan Regional Center. Instead, the Department directs those people to its much larger network of state-funded group homes that are run by corporate providers.
In many cases, families have told us that when they have asked about placements in state-operated group homes, DDS has stated that there are no vacancies in such homes in their area. That is despite the now-apparent fact that DDS doesn’t actually know whether there are vacancies or not.
Ambiguous statements about information on vacancies
For close to a year, DDS provided ambiguous responses to requests we made under the Public Records Law for information on the number of vacancies in the state-operated group home network in recent years.
In September 2023, I first filed a Public Records request with DDS, asking for “the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.” I also asked for data on the census, or number of residents in the state-run group-home system, and the capacity, or total number of available beds in the system.
DDS responded that it did not have “any responsive records pertaining to the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.” However, the Department added in that same response that, “The Department can provide the number of vacancies in state-operated group homes as of June 30, 2023, which is 91.”
Given that the Department was both saying it didn’t have information on the number of vacancies each year, but did have that information with regard to a specific date, I appealed to the public records supervisor. The public records supervisor agreed that it was unclear whether DDS did or did not have information about those vacancies.
DDS then responded with a statement that only appeared to add to the confusion. The Department stated:
Vacancies are not tracked by the Department independently from the capacity and census data provided above. Vacancy numbers are more complicated as they are dependent on a number of real time factors, including but not limited to the temporary placement needs of individuals, staffing, and other group home demographics.
Finally, this past July 10, after I had requested information on the number of vacancies through April of this year, DDS issued the following clarification:
DDS does not have in its possession, custody, or control the state-operated group home vacancies on the specific dates requested because DDS does not track state-operated group home vacancies. (my emphasis)
One-time “exercise” to determine vacancy number
In its July 10 response, the Department also sought to explain how it had come up with the number of 91 vacancies as of June 30, 2023, despite not tracking vacancies.
DDS stated that prior to my original Public Records request in September 2023, “DDS employees participated in an exercise which resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.”
However, since then, “no similar exercises have been conducted,” the DDS response stated.
That explanation, however, only appears to raise further questions.
Why, for instance, did DDS attempt on one occasion, but never again, to determine the number of vacancies in its group-home network?
Based on questions like that, I filed a new Public Records Request with DDS on July 12, seeking all documents relating to the Department’s exercise, which resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.
DDS stated that it will provide a response to my request as of Friday of this week (August 2).
DDS data on census and capacity raise further questions about possible vacancies
Despite the lack of data about vacancies, the data DDS has provided about the census and capacity of the state-operated homes implies to us that vacancies do exist in the group-home network.
As the chart below shows, the capacity in the state-operated group home system was close to 1,150 in the just-ended Fiscal Year 2024 (as of June 30). But the total census was only 986.
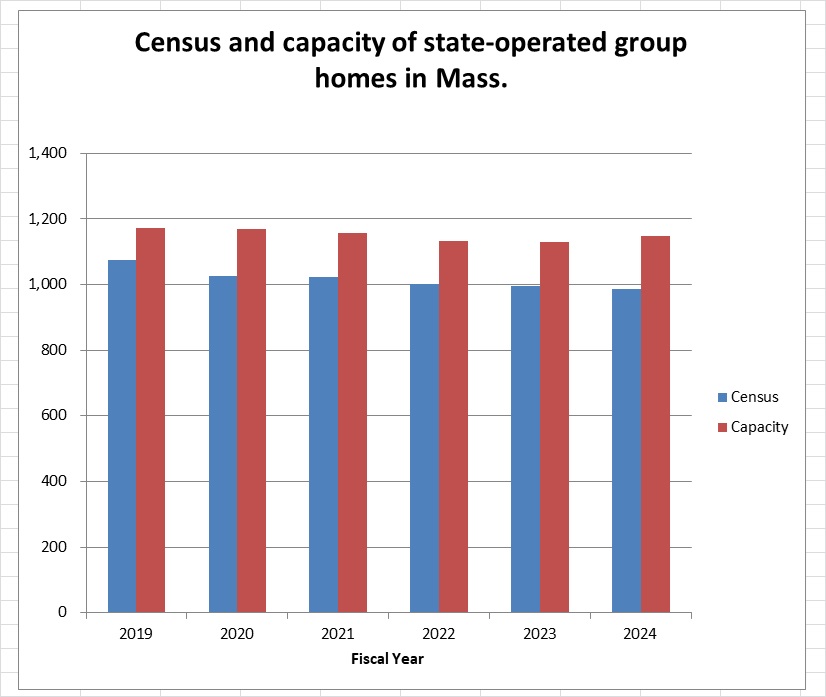
Source: DDS
The capacity as of June 30 was 16.4% higher than the census, implying that there were as many as 162 vacant beds in the state-run group home system that year.
The chart further shows that while the census (depicted by the blue columns) has steadily declined in the homes since Fiscal 2019, the capacity (red columns) declined through Fiscal 2022, and then began to rise in 2023 and 2024.
The gap between the census and capacity of the homes since Fiscal 2019 can be seen in the differences in the heights of the blue (census) and red (capacity) columns in the chart. That data appear to imply that the number of vacancies in state-operated homes has been rising since Fiscal 2022.
DDS, however, states, as noted, that it cannot confirm the number of actual vacancies in the homes because it doesn’t track them. The Department also maintains that vacancy numbers are “more complicated” than the difference between a group home’s census and its capacity.
DDS stated that the number of vacancies in group homes is “complicated” because it is “dependent on a number of real time factors, including but not limited to the temporary placement needs of individuals, staffing, and other group home demographics.”
It’s not clear to us what DDS actually means by that statement. It is not clear why the number of vacancies, for instance, would depend on staffing in the homes. In that case, it would seem that capacity would also depend on staffing. Yet, DDS was able to provide us with data on that capacity.
DDS’s reference to the temporary placement needs of individuals would appear to imply that the total census in the homes also changes over the course of the year due to temporary placements of certain individuals. Yet in that case as well, DDS was able to provide us with data on the census in the group homes.
It is unclear why DDS is able to track both the census and capacity of the homes, yet can’t or doesn’t track the number of vacancies. All three of those variables – census, capacity, and vacancies – would appear to depend on either staffing or temporary placements. Why are vacancy numbers more complicated than either census or capacity numbers?
The DDS data on the state-operated group homes raise many questions, as we’ve said. Unfortunately, DDS has repeatedly declined to answer our questions about the data.
We hope that the additional records DDS is scheduled to provide us about the one-time exercise it conducted will shed a little more light on the important vacancy question.
