Baker administration continues Gov. Patrick’s misguided effort to close sheltered workshops
As the Legislature takes up Governor Baker’s budget for the coming fiscal year, it looks as though the battle over sheltered workshops for the developmentally disabled in Massachusetts is set to begin once again.
Supporters of these vital programs won a reprieve last year when the Legislature inserted protective language for the workshops in the current-year budget. The language prohibits the Department of Developmental Services from closing or cutting off funding for sheltered workshops as long as there are people who seek them or wish to remain in them.
The budget language temporarily thwarted the efforts of then Governor Patrick to close all remaining sheltered workshops in the state as of this coming June. But the protective language has been removed from Governor Baker’s proposed budget for fiscal 2016.
It appears that despite the fact that we have a new governor, it is the same DDS with the same administrators running it; and they will never back away from their ideological opposition to any program that serves more than a handful of disabled individuals in one location.
Sheltered workshops provide settings in which developmentally disabled people can do assembly jobs and other types of work. In the view of the now Baker administration, such settings of care “segregate” developmentally disabled people from their non-disabled peers, and supposedly prevent them from reaching their potential in the mainstream workforce.
Many families and guardians of workshop participants, however, want these programs to continue and depend on them to provide valuable skills and meaningful activities to the participants.
Last spring, after a lobbying campaign by advocates of the workshops, language was inserted into the current-year budget, stating that DDS “shall not reduce the availability or decrease funding for sheltered workshops serving persons with disabilities who voluntarily seek or wish to retain such employment services.” The protective language survived a House-Senate conference committee in June, largely due to the support of House Ways and Means Chair Brian Dempsey.
But Governor Baker’s budget has not only removed that language protecting the workshops, the budget proposes a $4 million increase in a separate DDS account to move people from sheltered workshops into DDS day programs, many of which do not provide work-related activities.
We support the continued operation of sheltered workshops for reasons given in an email sent to Dempsey last May by Richard Urban, who is a guardian of his brother Tom. In December 2013, DDS closed Tom’s sheltered workshop where he had been employed for most of his adult life. Richard noted that Tom’s “work ethic and paycheck (from his sheltered workshop program) were two constants that allowed him a place on a playing field of equality with his peers, family and friends.”
Since his “forced exit from his workshop,” Richard said, Tom “has grown distant, is very confused, and expresses continued sadness over his job loss. His identity, and work community, have been lost, through no fault of his own but by virtue of a policy shift for which I am at a complete loss to understand.”
We’re at a loss to understand it as well.
Two lawmakers support an independent evaluation of Andy McDonald
More than a year ago, we asked for an independent clinical evaluation of a now 47-year-old intellectually disabled man, who has not been permitted to visit his parents in their Sherborn home for the past 19 years because he has been deemed to be a danger to the community.
Finally, two state legislators are asking for the same independent evaluation of Andy McDonald. In a letter sent to the Department of Developmental Services on February 25, both Senator Richard Ross and Representative David Linsky further asked that the evaluation take into account the views of Andy’s father, Stan, and his step-mother, Ellen, who have been fighting for years for supervised visits home for him.
Not only is Andy prohibited from visiting the home he grew up in; Stan and Ellen are not even permitted to discuss the topic with him. Under the rules imposed by his DDS-funded group home, Andy, who has frequently expressed a longing to see his home again, is forbidden from mentioning his desire to do so. It seems like a violation of free speech; but then again, when you are under the control of both the DDS and probate court system, your right to self-determination becomes very limited.
That loss of self-determination may be appropriate in some cases; but the McDonald case shows how dysfunctional the system can get. The case is replete with questions about the validity of previous clinical evaluations of Andy and about a 2006 probate court ruling, which concluded that Andy was sexually dangerous and should never be allowed to return home.
In the 2006 ruling in which he denied Stan’s bid for guardianship of Andy, Middlesex County Probate Court Judge Edward Rockett stated that Andy had been arrested in 1990 for sexual assaults of three young girls who lived across the street in Sherborn. That was not true, however.
Andy was arrested in May 1990 for threatening an unidentified person during a telephone call, according to the district court record. The nature of the threats was not disclosed. In July of that year, he was arrested for disturbing the peace in downtown Sherborn and with assault for punching his stepmother, according to a police report. Both Stan and Ellen say the punch was accidental and occurred while Ellen was driving Andy to the police station after he was accused of disturbing the peace. “He was flailing his arms, not threatening me,” Ellen said in an email this week, “and his fist landed on me. It didn’t hurt me. It made a red mark that faded shortly after.”
There is no indication in the police reports that Andy ever sexually assaulted anyone.
In his ruling, Rockett also cited a statement by the clinical director of Andy’s group home that Andy had told him he had had sexual fantasies about children. But Rockett acknowledged in his ruling that there was testimony in the court case that Andy “will always say what he thinks other people want to hear. This causes his statements to be very inconsistent.”
As we noted in a previous post about this case, Andy was committed to McLean Hospital in Belmont immediately after the July 1990 threatening and disturbing-the-peace incidents. In the years following, he was subjected to a series of inappropriate residential placements and treatment, in many cases because a series of court-appointed guardians, state agencies, and providers made the wrong decisions regarding his care.
Most of the decisions about placement and treatment of Andy were made without the consent of Stan, who had agreed to the appointment of a guardian for Andy in 1986 as part of the settlement of a longstanding custody battle over him with his former wife. Andy has had a series of court-appointed guardians since, and Stan has never been able to regain that guardianship. His attempts in probate court to do so have been opposed by DDS.
Andy has not exhibited any significant behavioral problems in a decade and has been taken on community outings to many places other than his home without any behavioral incidents, according to Stan and to notations in Andy’s clinical care plan. But that record of good behavior does not appear to have changed the position of either the probate court, DDS, or Andy’s current court-appointed guardian that he must never be allowed to go back to his hometown.
That ban on visits to Andy’s boyhood home combined with his group home’s policy that he must not even discuss his desire to visit his parents there amounts to psychological abuse, Stan maintains. Moreover, the situation raises concerns in Stan’s and Ellen’s minds about Andy’s future and what will happen when they are no longer able to travel from Sherborn to visit him in his group home in Northborough. Stan is 79 years old.
In 2000, Ronald Ebert, a psychologist, recommended that the staff of Andy’s group home try a “trial visit” to the Sherborn Inn to hear Stan, an acclaimed jazz musician, play in his band if it could be demonstrated that the persons Andy was accused in 1990 of threatening no longer lived in town. In fact, Stan says, those persons had moved away as of that time. “If such visits can be managed successfully, there is no reason why they could not be built into his visit schedule…,” Ebert wrote. But Ebert’s recommendation was never heeded.
As is the case with he parents of Sara Duzan, who were denied all contact with their daughter for several months, Stan and Ellen McDonald have found themselves trapped in a Twilight-Zone-like situation imposed on them by the state’s dysfunctional human services and probate court system. It’s long past time to bring in someone with a truly independent view to take a new look at this case.
Budget reductions falling heavily on state-run services for the disabled
During a conference call on Wednesday with advocates for the developmentally disabled, Department of Developmental Services Commissioner Elin Howe didn’t have much good news about the potential impact of Governor Baker’s proposed Fiscal Year 2016 budget.
The budget is bad news for DDS accounts, particularly state-operated services.
“These are huge and difficult reductions,” Howe said.
Baker is dealing, of course, with a projected budget shortfall in the coming fiscal year, and it looks as though people with intellectual and developmental disabilities are among those who will pay a price for that shortfall. Howe said DDS is assuming departmental layoffs will not be necessary if the Legislature accepts Baker’s early retirement proposal for state workers. If that doesn’t happen, measures such as layoffs may be needed, she said.
Just about every DDS account is being funded lower than what DDS had asked for. Howe said the governor’s budget required a total of $27 million in reductions from DDS funding requests, but DDS has been able to reduce the hit by $8 million by using some federal revenues as an offset to the total reductions.
As usual, state-operated services may be taking the brunt of the reductions. Howe noted that Baker was proposing a $2.6 million reduction from the DDS request in the state-operated group homes line item. Under Baker’s budget, the line item would be increased by $5.1 million, from current-year spending (from $209.6 million to $214.7 million). But that amount is below what DDS considers necessary to maintain current services.
Exactly what the state-run group home line item reduction means is unclear. Howe said DDS is not projecting “reductions in services to people,” but rather there will be “changes in staffing.” Among other things, DDS has been working to reduce the use of overtime in state-operated group homes, she said.
In January, we sent a letter to Kristen Lepore, Baker’s new secretary of administration and finance, asking that the new administration consider making the funding of state-operated care for the developmentally disabled a priority. For too long, as we noted, state government has been divesting itself of its responsibility to provide care for the most vulnerable of its citizens, and has failed to adequately monitor and control the handover of human services to state-funded corporate providers.
Baker’s first budget does not appear to address that situation.
In addition to the shortfall in funding for state-operated care, Howe said the state-run developmental centers line item would be funded under the governor’s budget at $2 million less than what DDS was requesting. This account would be cut from the level of spending in the current fiscal year as well, under Baker’s budget.
In addition, DDS service coordinators, Howe said, were being funded at a level $1.8 million below what DDS had requested. The DDS administrative line item, which funds the service coordinators, would be increased under Baker’s budget, but not by enough to maintain current services.
Corporate provider-run care does not come through unscathed in the governor’s budget, but the overall imbalance in funding between state and provider-operated care will remain.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. In fiscal 2014, then Governor Patrick and the Legislature increased the provider line item by more than $140 million –or more than 16 percent—in FY 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
The provider residential account subsequently received a supplemental budget increase in the current fiscal year of $44.7 million, even as both Baker and his predecessor, Patrick, were cutting spending across the board to deal with a projected current-year budget deficit.
Baker has proposed another $33.6 million increase in the provider residential line item for fiscal 2016, but DDS and the providers apparently wanted $4 million more than that.
Among the other DDS line items:
- Baker has proposed an increase in funding for the day program line item that is $9.7 million lower than what DDS wanted. The line item would be increased by $2.8 million under Baker’s budget proposal.
- Respite and Family Supports would be funded at a level $5 million below DDS’s request. Under Baker’s budget, the line item would be increased by $7.4 million, but this line item has been continually underfunded in recent years. It was cut in the current year by $2.5 million in light of the projected budget deficit.
- The transportation line item would receive a $3.5 million increase under Baker’s budget, but that increase was $3 million below what DDS wanted.
- The Autism and Turning 22 accounts would be level-funded, which amounts to a cut when adjusted for inflation.
- A long-time revenue account of $150,000 from sales from the dairy barn at the Templeton Developmental Center would be eliminated. The money has been used for program needs at the Center.
The fiscal 2016 budget is now before the Legislature, specifically the House Ways and Means Committee. We understand that this is a fiscally difficult time for all state programs. When it comes to the DDS budget, though, this may be a good time to rethink some longtime funding priorities. We hope key legislators will do just that in coming months.
Abuse investigation agency faces ‘shameful’ shortfall in funding
A COFAR Special Report
Due to a chronic lack of funding and a maze of legal constraints, the state’s only independent agency charged with investigating abuse and neglect of disabled individuals is able to undertake less than 2 percent of such probes, according to data reviewed by COFAR.
The Disabled Persons Protection Commission’s data show that between fiscal years 2004 and 2014, the agency investigated an average of 101 cases each year, or 1.5 percent of the average number of abuse and neglect complaints investigated.
An average of 6,836 cases per year – or more than 98.5 percent of them – were assigned or referred to other agencies to investigate, with the Department of Developmental Services chief among them.

Source: DPPC
“The DPPC may have one of the most important missions of any agency in state government,” said COFAR Executive Director Colleen Lutkevich. “Yet, it is barely permitted to operate. It’s a shameful situation.”
The impact of the agency’s lack of adequate funding appears to have changed little since The COFAR Voice published an in-depth look at the agency in 2004. At that time, the newsletter noted that between 1999 and 2003, the number of agency personnel investigating abuse and neglect complaints had dropped, due to budget cuts, from seven investigators to three.
A follow-up review by COFAR this year of DPPC reports and budget documents shows that in the decade between fiscal 2004 and 2014, neither the governors involved nor the Legislature demonstrated a consistent commitment to the DPPC or its mission. In a number of years, the agency’s budget was cut, resulting in the need for layoffs of investigators and other personnel, despite rising caseloads.
Among the results of the lack of funding is that the DPPC has been able only to increase its investigative staff from three in 2004 to six currently; and some of those investigators have other duties and are not available to work on investigations full time, according to Emil DeRiggi, deputy executive director of the agency. The investigative staff actually appears to be smaller than it was in 1999, which seven investigators were employed.
The DPPC is the only state agency in Massachusetts whose mission is devoted exclusively to preventing and investigating abuse and neglect of disabled persons. Other agencies that undertake those investigations also employ or fund caregivers who provide a wide range of services to the same individuals. This appears to cause potential conflicts for those agencies by requiring them to investigate their own services.
According to DeRiggi, the DPPC maintains an oversight responsibility over investigations it assigns to other agencies. However, the DPPC’s lack of funding appears to limit its oversight capacity.
The DPPC’s oversight officers, whose job includes monitoring cases assigned to other agencies, have seen their caseloads rise steadily. As of fiscal 2004, there were seven oversight officers at the agency, according to the annual report for that year. As of fiscal 2014 – a decade later – the number of oversight officers had grown only by one, to eight. Yet the total number of abuse and neglect complaints called in to the DPPC in fiscal 2014 was more than 3,000 higher –or more than 50 percent greater – than the number in fiscal 2004.
Lack of statutory authority
The DPPC’s enabling statute (Massachusetts General Laws chapter 19C) permits the agency only to investigate cases involving victims between the ages of 18 and 59. As the DPPC’s website describes it, the agency “fills the gap” between the Department of Children and Families (which investigates abuse of children through the age of 17) and the Executive Office of Elder Affairs (which investigates abuse of persons over the age of 60).
This situation involving individuals with developmental disabilities is further complicated because the Elderly Affairs agency is prohibited by statute from investigating abuse cases involving elderly persons in long-term care facilities such as developmental centers and group homes. The result is that the Department of Developmental Services has become, by default, the only agency with authority to investigate complaints of abuse or neglect of individuals over the age of 60 with developmental disabilities living in those residential facilities. DDS, however, faces a conflict of interest because it is frequently in the position of investigating charges of abuse and neglect in facilities either run by its own staff or by contractors it funds.
Perry case illustrates need for an independent investigatory agency
The case of the 2013 death of Dennis Perry, an intellectually disabled man, at the Templeton Developmental Center, illustrates the need for abuse investigations to be conducted by independent agencies such as the DPPC.
Perry, who was 64, died in September 2013 after having been allegedly shoved into the side of a boiler at the developmental center’s dairy barn by Anthony Remillard, a resident of the center, who had a history of violent behavior. As COFAR noted in a blog post, the DPPC was prevented by statute from investigating Perry’s death because he was over 60. The Executive Office of Elder Affairs was similarly prevented from investigating the matter because it occurred in a long-term DDS care facility. The investigation, as a result, fell by default to DDS.
The DDS investigation report raised a number of questions about its thoroughness. The report and related correspondence, dated in August 2014, concluded that there was no evidence that the staff at the Templeton Center could have prevented Remillard’s alleged “spontaneous and unpredictable assault” on Perry.
The DDS report, however, appeared to have failed to address a number of key questions about the Perry case, including whether it was appropriate for Remillard to have been admitted to the Templeton Center in the first place, and whether the overall level of supervision at the Center or of Remillard himself was adequate. The report merely examined the actions of staff caring for Remillard in the moments prior to, and during, the alleged assault.
Recognizing the need for independence in investigating the abuse of all persons in DDS facilities, the DPPC proposed legislation as long ago as 1992 that would have allowed it to investigate reports of abuse of elderly persons living in facilities operated or contracted by DDS. However, neither that bill nor similar bills filed in the following two years were enacted. The DPPC tried again in 2000, but that bill failed as well, and the agency hasn’t tried again since, according to DeRiggi.
Lutkevich does not believe legislation to give the DPPC more statutory authority to investigate a wider range of cases would have failed to gain passage in the Legislature had there not been behind-the-scenes opposition to it. That opposition, she maintains, has most likely come from DDS, the agency with the most political turf to protect in matters regarding abuse and neglect investigations.
“If DDS had wanted those bills to go forward (to give the DPPC more investigative authority), they would have,” Lutkevich contended.
A critical mission thwarted by underfunding
COFAR President Thomas Frain similarly said he believes DDS is largely responsible for keeping the DPPC in a state of perpetual underfunding in order to prevent it from having the fiscal resources to investigate more cases in the DDS system.
“DDS has enormous influence and sway over the Legislature,” Frain maintained. “Historically, the Legislature has not gone against DDS. If DDS was in favor of adequate funding for the DPPC, its funding situation would improve overnight.”
As the DPPC’s website notes, the agency’s mission is “[t]o protect adults with disabilities from the abusive acts or omissions of their caregivers through investigation oversight, public awareness and prevention.” The DPPC also arranges for protective services when abuse has been substantiated and provides training and education for service providers, law enforcement agencies and others.
As noted, however, the DPPC’s funding level leaves it unable to carry out its mission fully or effectively fill the gap between the Children and Families and Elder Affairs agencies.
Budget woes have affected staffing
As of fiscal 2014, the staff of the DPPC included four individuals in its administration and finance office, five in its hotline intake unit (with a contracted provider operating the hotline after hours), five in its investigations unit, eight in an oversight unit, two in outreach and prevention, one in information and technology, four in document retention, and two in a legal unit. As noted previously, not all of those staff positions are full-time. That total number of staff was lower in fiscal 2014 than it had been in fiscal 2010.
The DPPC’s budget does not include a five-member Sate Police Detective Unit assigned to the DPPC, which reviews every report to the hotline to determine if a criminal investigation is necessary.
The DPPC’s total funding rose from $2 million to $2.8 million in inflation-adjusted (fiscal 2015) dollars between fiscal 2004 and 2014 – a 37 percent increase over that period. But budget cuts between fiscal 2009 and 2012 necessitated overall staffing reductions, according to agency annual reports and other records. It’s not clear that the agency ever recovered from those reductions.
The agency’s funding level has risen and fallen in the past decade, reflecting the state’s fiscal outlook. In fiscal 2009, funding had actually been increased from the previous year by $204,000, the largest increase the agency was to receive until the current fiscal year. DPPC Executive Director Nancy Alterio stated in the agency’s fiscal 2009 annual report that as a result, DPPC was able to increase its investigation staff by 50 percent, from four to six investigators, “in addition to addressing other caseload challenges in the oversight unit.”
In addition, the number of “overdue” investigations in fiscal 2009 decreased from over 900 to 578, Alterio said. Overdue investigations are those taking more than 30 days to complete. But in the annual report, Alterio also warned that those gains in staffing might be reversed in fiscal 2010.
That warning came true. The DPPC budget was subsequently cut each year from fiscal 2009 through 2012, dropping from $2.6 million to $2.3 million in inflation-adjusted dollars. It was only in the current and past two fiscal years that some of that lost ground was made up in the form of increased funding, bringing the budget to $2.8 million in fiscal 2014.
While fiscal 2009 did mark the beginning of three years straight of budget cuts, the number of overdue investigations did continue to drop to a low of 465 in fiscal 2012, according to DPPC data. But after that, the number of overdue investigations began to rise again, back to more than 600 in fiscal 2014. In fiscal 2010, Alternio noted that about 85 percent of investigations were not completed in 30 days.
In fiscal 2010, the DPPC was forced to reduce its total workforce from 32 to 28 Full Time Equivalent (FTE) staff. Yet at the time, the agency was facing an average annual increase in abuse reports of 4 percent, stretching over the previous 10 years, according to Alterio. Between fiscal 2004 and 2014, an average of 2,100 abuse and neglect complaints a year have been “screened in” by DPPC for investigation.
The DPPC received a relatively small increase in funding in fiscal 2013 of about $86,000, but it was not enough to prevent an additional layoff and reduction in the total staff to 27.4 FTEs.
“Each fiscal year, operating expenses increase and therefore additional funds are necessary just to maintain operations at the same level from year to year,” DeRiggi wrote in response to an emailed question.
A ray of hope in the current fiscal year
The current fiscal year opened last July on a slightly more positive note for the DPPC. For the first time, the agency received a funding increase of more than 10 percent. The Legislature approved a $362,000 increase in agency funding, bringing the DPPC’s budget to $2.8 million.
According to DeRiggi, the budget increase was projected, among other things, to allow a seventh investigator to be hired in the current fiscal year. That 13 percent increase in funding in inflation-adjusted dollars had not been in the budget submitted in January 2014 to the Legislature by former Governor Deval Patrick. Patrick had proposed only a $48,000 increase for the DPPC, which would have been less than two tenths of a percent if adjusted for inflation. It was apparently in the Senate that the larger increase was approved.
Asked if there was a particular legislator who had sought the 13 percent increase for the DPPC, DeRiggi said he and agency staff were not aware of who that might have been. “Hopefully this year’s proposed allocation is a reflection of an understanding of the seriousness of the issues DPPC investigates, but we are not certain of why it came about,” he said.
But given that the outgoing Patrick administration and incoming Baker administration have projected a budget deficit in the current fiscal year that could run higher than $700 million, it is once again possible that the DPPC’s budget will be cut, requiring another cycle of staffing reductions.
And despite the funding increases that the agency received starting in fiscal 2013, it has not been able to restore all of its functions and services that were cut in preceding years. For instance, in April 2009, the DPPC was forced to eliminate a service to human services providers under which it would search its database to see whether prospective employees had been charged with abuse. That service has not since been restored.
(Upcoming post: A case in which the DPPC got sidetracked from its mission)
Public Health Department needs to release report on death of developmentally disabled man
The Department of Public Health has completed an investigation of the case of a developmentally disabled man who died en route to Lowell General Hospital in February 2012 after having been turned away from the hospital twice without any significant treatment.
We may never know, however, what the result of the investigation is. The Department, citing the deceased man’s privacy rights, won’t release the report.
We are appealing this denial to the state’s Public Records Division, arguing that the potential public interest in knowing what happened in this case outweighs the privacy rights of a deceased individual. Our view is that the real potential wrong to this person was done when he was denied treatment by the hospital. The public, we think, deserves to know what happened here and so do persons with developmental disabilities and their families and guardians.
This case suggests possible inadequate training of health care personnel in the treatment of developmentally disabled persons, which is an issue of concern to advocates for the disabled and to many policymakers.
The National Council on Disability, with which we have had our disagreements, maintains that:
The absence of professional training…for health care practitioners is one of the most significant barriers preventing people with disabilities from receiving appropriate and effective health care.
The man was a former resident of the Fernald Developmental Center. He had been living in a group home in Chelmsford and was attending a day program in Lowell on the morning of February 6, 2012, when the staff at the day program made the first call to 911 to take him to the hospital. He had reportedly been having difficulty breathing and was sweating profusely. The hospital released the man shortly after his arrival, however, and sent him back to his group home, according to sources.
By about 8 a.m. the following morning, the man was slumped over in his wheelchair and sweating heavily, a source said. A group home staff member called 911 shortly afterward.
A Disabled Persons Protection Commission (DPPC) complaint form stated that the man was observed at the hospital on the morning of February 7 to be sweating profusely, but his vital signs were good when he arrived. According to the complaint form, the man was sent home with a prescription (the name of which was redacted). According to sources, this was the second time he had been sent away by the hospital.
The DPPC complaint form stated that shortly after arriving back at the group home, the man began to vomit and then lost consciousness, and that the staff began mouth-to-mouth CPR until paramedics arrived. The group home received a call from the hospital later that afternoon that the man had died.
Because the man’s death appeared to have been connected with his treatment or lack of treatment by the hospital, the DPPC referred the case to the Department of Public Health for investigation.
Did the apparent failure of Lowell General Hospital to properly diagnose this man’s illness and provide him with adequate treatment result from a lack of training in disability issues? Did the Public Health Department consider that question in their investigation of this case? Unless the Department releases its report, we will never know the answers to those questions.
While the Public Health Department’s position is that a state law [(M.G.L. c. 66A, s. 2(k)] prohibits them from releasing medical information about an individual, even if that person is deceased, we are not in agreement with their interpretation.
First, there do not appear to be consistent policies among state agencies in releasing investigative reports on deaths of developmentally disabled persons. The Disabled Persons Protection Commission (DPPC) has released a number of these reports to us after redacting what they considered to be identifying information.
Secondly, while we have blogged about this case, we have never used the name of the individual involved or tried to publicly identify him. A Department of Public Health attorney wrote to us, though, that even if we did not use the individual’s name in a blog post about the investigative report, “it is possible for someone to utilize the information that is available (age and date of death) and potentially come up with the patient’s name.” While that is possible, we do not understand why anyone would do that in this case. It seems farfetched.
Third, even if it were true that someone might reveal the identity of the individual involved, there appears to be case law that limits privacy rights of deceased individuals. A Hofstra Law Review article notes that “while postmortem medical confidentiality exists, it is much narrower than the privacy protections guaranteed to the living.” In Massachusetts, case law involving privacy rights after death does not appear to have been settled. (See Ajemian v. Yahoo!, Inc.)
Finally, the privacy statute cited by the Public Health Department [(M.G.L. c. 66A, s. 2(k)] states only that the Department must:
maintain procedures to ensure that no personal data are made available in response to a demand for data made by means of compulsory legal process, unless the data subject has been notified of such demand in reasonable time that he may seek to have the process quashed.
This seems to imply that the person involved has to be living. And, as attorney Steve Sheehy notes in a comment to this post below, at most this statute would require notice to the deceased person’s executor or representative.
Prior to filing our appeal, I asked the Public Health Department attorney whether it might be possible to provide us with a copy of the investigative report with explicit personal data or medical information redacted. As I noted, our interest is whether the Department has investigated or commented on the hospital’s procedures for training staff to treat persons with developmental disabilities.
To the extent that the Department’s report addresses hospital policies and procedures in this case, it would probably not be necessarily for us to know specific medical details about this individual. To date, I have not received an answer from the Department to my query.
Unfortunately, this is not an isolated case of apparent institutional secrecy. When it comes to deciding whether to make public reports of potential mismanagement by human services or health care facilities, the natural instinct of public managers and administrators seems to be to keep it all secret and cite privacy rights as the reason. That has certainly been the practice at the DPPC, but at least, as noted, the DPPC has released redacted reports.
We hope the Public Records Division, which is part of the office of Secretary of the Commonwealth Bill Galvin, will make the right decision and order the Public Health Department to make known the results of its investigation of this troubling Lowell General Hospital case.
Compensation of provider executives in MA reaches $100 million
More than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation, according to our updated survey of the providers’ nonprofit federal tax forms.
By our calculations, state taxpayers are on the hook each year for up to $85 million of that total compensation.
We reviewed the federal tax forms for some 300 state-funded, corporate providers, most of which provide residential and day services to persons with developmental disabilities.
The following is a summary chart of our latest survey results (click on the chart to enlarge):

For the complete survey chart, click here.
We first released our survey about a year ago, when we found that more than 550 executives working for some 250 state-funded corporate providers of services to people with developmental disabilities in Massachusetts received a total of $80.5 million in annual compensation.
COFAR has also previously raised concerns that increasing amounts of money going to provider executives have not translated into higher pay for direct-care workers in Massachusetts.
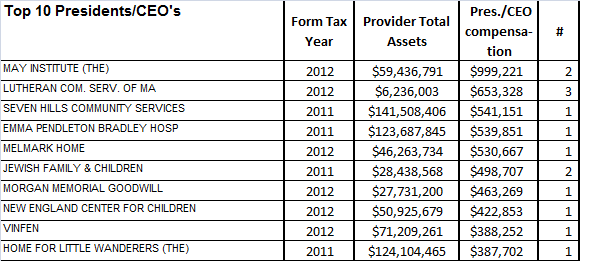
The latest survey reports on 635 executives who received total annual compensation of $102.4 million and average annual compensation per employee of $161,231. The survey was based on provider tax forms filed in either the 2011 or 2012 tax years. Those tax forms are available online at www.guidestar.org.
The survey sample included 100 CEO’s and presidents, making an average of $210,227 in salaries and benefits; and 107 executive directors receiving an average of $130,835 in compensation. As the chart above shows, the survey also included 67 chief financial officers, 31 chief operating officers, 100 vice presidents, 110 directors, and 120 other officers, all earning, on average, over $100,000 a year.
A state regulation limits state payments to provider executives to $158,101, as of fiscal year 2013. Money earned by executives above the state cap is supposed to come from sources other than state funds.
Based on this regulation, we calculated that provider executives are eligible for up to $85 million a year in state funding to cover those total salary and benefits costs. Our calculation was based on identifying the companies paying executives at or above the state threshold of $158,101, and assuming that amount as the maximum state payment for each of those companies’ executives.
Among the top-paying providers in our latest survey was the May Institute, which paid two employees a total of $999,221 in the 2012 tax year. Both employees were listed as president and CEO of the provider. The May Institute’s federal tax form shows that one of the two employees, Walter Christian, worked for the company until December 2012 and received a total of $725,674 in salary and benefits in that tax year, which started on July 1, 2012. Christian was replaced as president and CEO by Lauren Solotar, who received a total of $273,547 in that same tax year, which ended on June 30, 2013.
Despite the regulation capping compensation payments by the state, the state auditor reported in May 2013 that the state had improperly reimbursed the May Institute, a corporate provider to the Department of Developmental Services, for hundreds of thousands of dollars paid to company executives in excess of that cap. COFAR had previously reported in 2011 that the state may have paid Christian and other executives of the May Institute more than the state’s regulatory limit on individual executive salaries.
The following charts show the top earning presidents/CEO’s and executive directors in our latest survey and the number of those executives holding each title in each company:

Most of the providers surveyed are under contract to the Department of Developmental Services, which manages or provides services to people with intellectual disabilities who are over the age of 22. The providers operate group homes and provide day programs, transportation and other services to tens of thousands of intellectually disabled persons in the DDS system.
As we have noted, the state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in fiscal 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
More financial information about nonprofit corporate providers, including compensation of executives, can be found at www.guidestar.org.
It’s time to put a priority on state-operated care for the developmentally disabled
Here’s our letter to the Baker administration, asking them to put a priority on state-operated care for the developmentally disabled:
Kristen Lepore
Secretary
Executive Office of Administration and Finance
State House, Room 373
Boston MA, 02133 January 12, 2015
Dear Secretary Lepore:
We are writing to urge you to consider making the funding of state-operated care for the developmentally disabled a priority of the Baker administration.
For too long, state government has been divesting itself of its responsibility to provide care for the most vulnerable of its citizens, and has failed to adequately monitor and control the handover of human services to state-funded corporate providers.
The state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue. This has led to a gross imbalance in the Department of Developmental Services budget. The chart below depicts this imbalance.
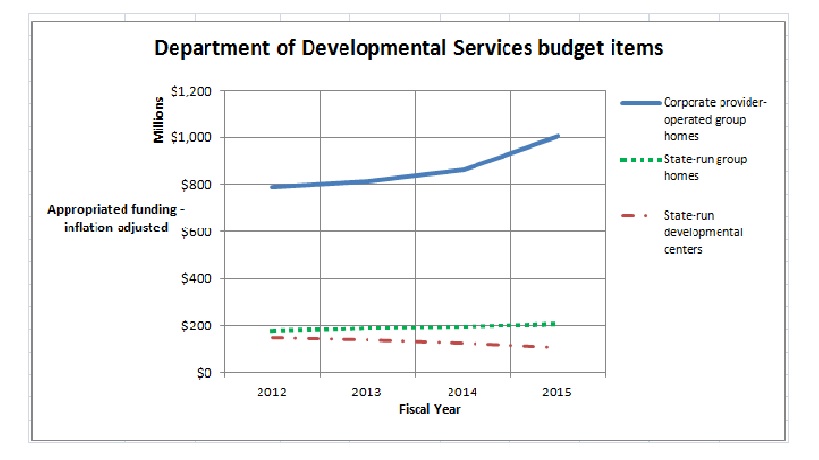
As the chart shows, funding to DDS corporate residential providers (line item 5920-2000) rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in FY 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
The state-run developmental center line item (5930-1000) was cut in the current fiscal year by more than 13 percent in inflation-adjusted dollars, while the state-operated group home line item (5920-2010) was raised by less than 7 percent.
We have calculated that if the increase in the provider residential line item had been reduced by just 2.1 percent – to a 14.7 percent increase – as much as $18 million could have been redirected to the state-operated group homes, DDS service coordinators, the Autism Division, Turning 22 program, Respite and Family Supports, and the remaining developmental centers in the state.
But the previous administration was not satisfied even with a $140 million increase in funding for the corporate provider line item. In late November, despite a projected $329 million budget deficit in the current fiscal year, the Patrick administration proposed a supplemental budget increase of $42 million in the provider residential line item. While the administration made more than $200 million in emergency “9C” cuts and proposed additional cuts to address the projected deficit, it included the $42 million in proposed supplemental funding for the DDS corporate residential line item in the same bill (H. 4536) proposing mid-year cuts in local aid and other accounts.
In addition to the erosion of critical state-funded care, the state’s priority of boosting funding to corporate providers has created a poorly monitored system of DDS contractors that has financially benefited provider executives. Our own survey of the DDS provider system has shown that the state has provided between $80 million and $90 million a year to a bureaucratic layer of corporate CEO’s, vice presidents, executive directors, and other executives. At the same time, wages of direct-care workers in provider residences have been flat or have declined in recent years.
State-operated group homes and developmental centers
We believe the misplaced priority on funding of corporate providers ignores the wishes of family members and guardians around the state for more choice and availability in state-operated care. DDS data show that close to 42 percent of the 372 individuals moved out of developmental centers in the state since 2008 were placed in state-operated group homes. Another 45 percent of those residents were transferred, at the request of their families, to remaining developmental centers. Just 13 percent of those individuals went to provider-run group homes.
Yet, since 2008, 157 new provider-operated group homes have been built in the state, according to information provided by DDS. In that time, only 38 new state-operated group homes have been built, and three have been closed or converted to provider-operated homes. DDS has projected that it will build an additional six state-operated group homes, but will close or convert five state-operated facilities to provider residences.
Additional funding is needed for the state-operated group home system to preserve it as a choice for people waiting for residential care in the DDS system.
State-operated developmental centers
As a result of class-action lawsuits dating back to the 1970’s, the State of Massachusetts dramatically improved care in its state-run developmental centers, bringing them to a world-class level of care with dedicated, highly-trained staff. But starting in 2003, the Romney administration and subsequently the Patrick administration began efforts to close the state’s then six remaining developmental centers.
Starting in 2008, the Patrick administration stepped up the closure efforts and shut the Monson, Glavin, Templeton, and Fernald Developmental Centers, in many cases over the strong objections of families and advocates of the residents there. And despite the demonstrated desire of families and guardians for the intensive and high-quality care that the developmental centers provide to the most profoundly developmentally disabled, the developmental center line item has been cut repeatedly since 2008. The current-year DDS budget cut the developmental center line item by more than 13 percent in the current fiscal year alone, as noted.
We hope the Baker administration will consider restoring balance to DDS budget accounts by increasing funding to the developmental center and state-operated group home line items. State-operated care continues to be better monitored than provider operated care; and training as well as pay and benefits provided to staff in state-run facilities continue to be higher than in provider-run residences.
Ultimately, only government is in a position to respond directly to the public interest and to the wishes of families and guardians of the most vulnerable people among us. Federal law recognizes that fact by designating families as the “primary decision makers” in the care of individuals with developmental disabilities [(42 U.S.C. §2001(c)(3)].
Thank you for your consideration.
Sincerely,
Colleen M. Lutkevich Thomas J. Frain, Esq. Edward Orzechowski
Executive Director President President, Advocacy Network
Administration proposing last-minute regs changes that will reduce DDS oversight of providers
As it winds down to its last few weeks, the Patrick administration is set to make changes to two state regulations that we are concerned will reduce state oversight of corporate providers of services to the developmentally disabled and further reduce family involvement and choice in care and services.
We are particularly concerned about a proposed change by the Department of Developmental Services that appears to give DDS providers at least partial say in whether their licenses to operate residential and other programs are renewed. Proposed new language in the regulation (115 CMR 8.00, Certification, Licensing and Support) codifies a process that allows providers to assess their own compliance with state licensing and certification standards. This, to us, seems to sanction a conflict of interest.
Meanwhile, proposed changes to a second regulation (115 CMR 7.00: Standards for All Services and Supports) appear to reduce staffing requirements for group homes and remove the words “rights and dignity” from a discussion about providing residential supports and services to DDS clients. More about those additional changes below.
The rewrite of the licensure regulation adds a new section that refers to both a “self-assessment” done by the provider of its own supports and services and a “targeted review” of the provider by the Department as part of the licensure renewal process. Licenses to operate are normally granted to DDS corporate providers every two years following a survey or inspection of their residences and programs. The following sentence in this new section seems to describe a key aspect of this process:
Ratings from the targeted review and self-assessment [done by both the Department and the provider] will be combined to determine…the licensure levels for the provider. (my emphasis)
Based on this language, it appears as though the provider is expected to be involved in making the decision whether the provider will be granted a full renewal of its license or a conditional license or whether it will receive some other licensure requirement. This seems to defeat the purpose of the licensure process, which should be to provide an outside assessment of the provider’s ability to provide adequate supports and services, and to make licensure decisions that are independent of influence from the entity being licensed.
In particular, the provider will be given the authority to review licensure and certification “indicators” that it was found in surveys not to have met.
DDS licenses and certifies hundreds of nonprofit, state-funded group home and day program providers throughout the state each year. A review by COFAR in 2012 of 30 randomly selected online licensure and certification reports raised a number of questions about the effectiveness of the provider licensure and certification system in general. The review also found that DDS made substantial changes to its licensure and certification procedures based on input from the providers themselves.
Other proposed licensing changes
In addition to the introduction of the self-assessment process, the rewritten licensure regulation adds a requirement that the Department give providers at least 30 days notice of planned licensure visits or surveys of their residences. Currently, there is an advance notification requirement, but there is no timetable for that notice in the regulation. Under the new language, the provider has a month to get ready. Once again, this allowance appears to defeat the purpose of the licensure survey process, which is to assess the ongoing care and conditions in facilities.
If a provider knows a month ahead of time exactly when a two-year licensing survey of its facilities will take place, the provider will have an incentive to bring its facilities into compliance with licensing standards at that particular time, but not necessarily at any other time.
In the same section, the rewrite removes current language stating that notification of the survey must also be given to guardians, family members, individuals, and service coordinators. It seems doubly inappropriate to us that the providers will receive a month’s advance notice of planned survey visits, but guardians and families will apparently no longer be told about those visits. We cannot think of any legitimate justification for eliminating that notification to families and guardians other than a desire to keep them in the dark about the Department’s licensure and provider monitoring efforts.
In addition t0 those changes:
- The rewrite of the licensure regulation removes a statement that the survey team may review the provider’s system for conducting Criminal Offender Record Information (CORI) checks on all persons whose paid responsibilities may bring them into direct contact with individuals served. We do not understand the rationale for removing this common-sense requirement.
- The rewrite removes language stating that in cases in which a provider fails to correct conditions that place residents’ lives in jeopardy, those services will not be licensed or certified until such time as corrective action has been taken. We do not understand the rationale for removing this common-sense requirement either.
- The rewrite also increases the length of term of a “conditional license” granted when there is only “partial achievement” of licensing standards or “critical indicators” from one year to two years. Thus, even if a provider is only able to partially meet licensing standards, the provider will still receive the same two-year term for its license as providers that are able to meet all the standards.
Changes to the Services and Supports regulation
As noted above, DDS is proposing a number of changes to the services and supports regulation, which we are concerned will reduce both group home staffing requirements and rights of DDS clients. Those proposed changes include the following:
- In defining and discussing both Residential and Individualized Home Supports, the rewritten language in this regulation removes the words “rights and dignity” in discussing client outcomes. In one instance, that wording is replaced by language stating that providers “shall operate in a manner that supports positive outcomes for individuals in all of the services and supports offered…”
- In defining Family Supports, the rewrite eliminates the phrase that these supports should “enable the family to stay together.” We cannot think of any legitimate justification for removing that phrase.
- In discussing Staffing Standards, the rewrite removes a reference to providers having sufficient staff with enough training to ensure “quality of life outcomes delineated in the provider’s mission statement…”
- The rewrite of this same section removes a requirement that there be at least two staff persons on duty in homes where three or four individuals live and in which three or more individuals require assistance to evacuate within 2½ minutes. In addition, the rewrite removes a requirement that at least one “overnight awake” staff person be on duty at night in homes in which at least one individual requires assistance to evacuate within 2 1/2 minutes.
- The rewrite adds a section to the regulation that appears to advocate the opportunity of “integrated” or mainstream work opportunities for all persons with developmental disabilities, apparently no matter how low-functioning they are. For instance, the new language states the following: “Integrated, individual employment is the preferred service option and outcome for adults of working age…All individuals are to be encouraged and supported in seeking and securing employment or becoming engaged on a pathway to employment.” (my emphasis)
We believe the Department needs to recognize that there are differences in the levels of ability and achievement potential in different people. The new language in this section reflects an ideological blindness to those differences and does a disservice to all persons with developmental disabilities.
DDS has scheduled hearings on the regulatory changes on Wednesday (December 17) at 10 a.m. at the DDS Central Office at 500 Harrison Avenue in Boston, and on Thursday (the 18th) at 10 a.m. in the Northborough Free Library, 34 Main Street, Northborough. Written comments may be submitted by mail to the Office of the General Counsel, DDS Central Office, or by fax to (617) 624-7573 until 5:00 p.m. on Thursday.
We thought there was a state budget deficit
Given that the Patrick administration is projecting a $329 million state budget deficit in the current fiscal year and is seeking to cut millions of dollars in local aid and other accounts, why are they also proposing more than $42 million in additional funding in the current year for corporate providers that contract with the Department of Developmental Services?
While the administration has made more than $200 million in emergency “9C” cuts and has proposed additional cuts, it has filed a supplemental budget appropriation to add $42.5 million to the DDS Adult Long-term Residential (corporate provider) line item. The supplemental funding for the providers, by the way, is listed in the same bill filed by the administration that proposes mid-year cuts in local aid and other accounts.
It’s not as though DDS itself is being spared the funding cuts. As part of the 9C reductions, two DDS line items are being cut: the Community Day and Work line item by $3 million, and Respite Family Supports by $2.5 million.
But the DDS providers are getting multiple funding increases. As of July 1, the administration and Legislature had agreed to raise the provider line item by $159 million from the previous fiscal year, pushing it over the $1 billion mark. The reason for that nearly 20 percent increase in funding in one year was to fully fund higher payment rates to the providers that were agreed to in legislation enacted in 2008 and known as “Chapter 257.”
But even that $159 million increase this year wasn’t apparently enough. The $42.5 million supplemental appropriation now being sought by the administration is supposedly to make up for a continuing shortfall in fully implementing the Chapter 257 rate increases for the providers.
But why make up that Chapter 257 shortfall now while we’re facing a state budget deficit? Chapter 257 has apparently not been fully funded since it was enacted in 2008, so why is it so important to commit $42 million to it now?
Meanwhile, in light of the planned $42 million increase to the providers, the decision to cut at least one of the two DDS programs –Respite Family Supports by $2.5 million — is especially puzzling. Respite care involves short-term, out-of-home supports for individuals with developmental disabilities who live at home. It allows parents and other primary caregivers to handle personal matters, emergencies, or simply take a break. In fact, DDS listed its commitment to supporting families who care at home for developmentally disabled individuals as the third of its top five strategic goals for fiscal 2012 through 2014.
The DDS strategic plan goes on to promise that:
The Family Support account will provide the resources needed to provide vital respite care, in-home skills development, social programs and support groups for parents and siblings.
The administration and Legislature had, in fact, approved a $2.5 million — or roughly 5 percent — increase in the Respite Family Supports account as of the start of the fiscal year on July 1. So taking that increase away now amounts to an effective cut in inflation-adjusted terms in this “vital” program. The fact that the money is being rescinded in the middle of the year effectively doubles the impact of that cut to $5 million on an annualized basis.
The DDS Community Day line item had been increased by $11.8 million from the previous fiscal year, apparently in part to help fund the transfers of people from sheltered workshops to day programs. In addition, the Legislature had approved two reserve funds totaling $3 million to help fund that same transfer from sheltered workshops to day and employment programs.
The mid-year cut in the Community Day account of that same $3 million amount may make some sense given that language was approved in the current-year budget preventing the planned closures of sheltered workshops. If the workshops are going to stay open past this coming June, DDS won’t need the funding they were originally projecting to transfer people to day programs.
But while the Community Day account cut might make some sense, the cut to the Respite Family account seems to make much less sense. And when considered in light of the extra millions going to the providers, the Respite Family cut seems downright cruel.
In fact, we might take this occasion to ask what happened to the additional $80 to $110 million in Medicaid funding from the federal government that was going to be used to “increase community services and decrease institutional settings in Massachusetts?” As the Massachusetts Association of Developmental Disabilities Providers stated, “the activities of DDS comprise a significant part of the base for this (additional Medicaid) award…”
If we have received up to $110 million in additional Medicaid funding this year, why not use that to help solve the budget deficit, and at least prevent cuts to critical programs such as Respite Family care? Moreover, we hope the House and Senate Ways and Means Committees will see fit to put the administration’s proposed $42 million increase in state funding to the DDS providers on hold, at least while we’re dealing with the current budget shortfall.
DDS should not be investigating itself for abuse and neglect in the Perry case, or in any other cases
As Fox 25 news reported earlier this month, the Department of Developmental Services has determined there was not sufficient evidence to charge staff at the Templeton Developmental Center with mistreatment, stemming from the death last year of Dennis Perry, an intellectually disabled man.
Perry, who was 64, died in September 2013 after having been allegedly shoved into the side of a boiler at the developmental center’s dairy barn by Anthony Remillard, a resident of the center, who had a history of violent behavior.
The DDS investigation report and related correspondence, dated in August of this year, termed the behavior of certain staff prior to the alleged assault “inappropriate” and “unprofessional,” and recommended retraining of Templeton personnel. But the report concluded that there wasn’t evidence that the staff could have prevented Remillard’s alleged “spontaneous and unpredictable assault” on Perry.
We are not in a position to second-guess the conclusions of the DDS report. But this case once again raises the question whether it is appropriate for DDS, in effect, to investigate itself in abuse and neglect cases.
Due to legal loopholes, which I’ll discuss below, DDS itself investigates all cases of abuse and neglect of persons over 60 with developmental disabilities who live in long-term care facilities operated or contracted by the Department. As a result, the Department’s investigation of Perry case and its handling of it raise numerous questions.
By way of disclosure, Thomas Frain, president of COFAR’s Board, is representing Perry’s family in legal action against the state in the incident. I haven’t consulted Attorney Frain in writing this post, other than to ask him for a copy of the DDS investigation report.
Among the questions raised by the Perry case that don’t appear to have been considered in the DDS report are: Was it appropriate for Remillard to have been admitted to the Templeton Center in the first place, and was the overall level of supervision at the Templeton Center adequate? The DDS report didn’t even appear to consider whether the level of supervision of Remillard himself was adequate. The report merely examined the actions of staff caring for Remillard in the moments prior to, and during, the alleged assault.
For instance, the DDS report noted that a Templeton staff member had “sat” on Remillard because he wouldn’t get up from a nap just before the alleged assault of Perry occurred, and told him he would not be given a sandwich if he didn’t cooperate. There was a reference to a staff person “flicking” some water at Remillard as well.
The DDS report, which was based on statements taken from staff, stated that Remillard laughed in response to the staff person’s actions, got up and went to a bathroom to change his shoes. Then, on his way with a staff member to the an exit door in the dairy barn, Remillard suddenly spun around and shoved Perry, who had been standing nearby, toward the boiler, causing him to hit his head and fall to the floor. The staff stated that Remillard’s action was so unexpected and sudden that there was nothing they could do to prevent it.
That may all be perfectly true, but in focusing entirely on the actions of staff immediately prior to the alleged assault, the DDS report missed the potentially more important questions noted above. The report did note that Remillard had a history of criminal assaults and threats, including threatening with a dangerous weapon and threatening to blow up a school, and had a pending arson charge against him when he was admitted to Templeton. While at Templeton, he was verbally abusive toward staff and had assaulted staff members, according to the report. So, why not examine some questions that go beyond just what the staff at the time of the alleged assault did or didn’t do?
As we have pointed out many times, Templeton is one of several state-run facilities that have been either closed or significantly downsized in recent years, and the declining level of staffing and supervision in these facilities has been a source of concern. It’s not surprising that DDS, which is heavily invested in closing and downsizing these facilities, would not want to examine any potential negative impacts of that downsizing.
For reasons like that, we have long argued in favor of providing more funding and resources to the Disabled Persons Protection Commission (DPPC), an independent agency, to investigate abuse and neglect complaints. The DPPC, however, has been given such a limited budget and resources by the administration and Legislature that it is forced to refer most of the complaints it receives to DDS for investigation. The DPPC is further prevented by statute from investigating allegations of abuse or neglect of individuals over the age of 60.
Because Perry was over 60, the DPPC referred the investigation of his assault to both DDS and the Executive Office of Elder Affairs, according to a DPPC official whom I emailed about the case. The EOEA itself is prohibited by statute, however, from investigating abuse cases involving elderly persons in long-term care facilities such as developmental centers and group homes.
The result is that DDS has become, by default, the only agency with authority to investigate cases such as that of Perry in which an elderly person with an intellectual disability is allegedly abused in a long-term care facility.
The DPPC tried to rectify that situation as long ago as 1992. A May 1994 directive from the then secretary of elder affairs expressed support for a bill filed that year by the DPPC that would have allowed the DPPC to investigate reports of abuse of elderly persons living in facilities operated or contracted by DDS. The directive noted that similar legislation had failed to pass in the previous two years. The 1994 bill wasn’t enacted.
A DPPC official said this week that the agency filed a bill again in 2000 that would have given it the authority to investigate abuse of elders in DDS facilities. That bill failed as well, and the agency hasn’t tried again since. It seems fairly clear that the DPPC realized it was going to get nowhere with legislation that would give it more investigatory authority at the expense of DDS.
For years, the DPPC has asked for more resources to enable it to hire more investigative personnel. In our view, it has been DDS itself that has lobbied the Legislature against the DPPC’s common-sense recommendations to increase its investigative authority and resources, and has fought to keep the DPPC’s budget as low as possible. It appears to be a political turf issue as far as DDS is concerned.
In the meantime, it appeared earlier this year that the Legislature’s Children, Families, and Persons with Disabilities Committee might step in and take an independent look at the Perry case and the issues surrounding it. Last January, we received a notice from the office of Representative Kay Khan, House chair of the committee, that the committee was planning an oversight hearing on the Perry case. But despite a subsequent inquiry that we made to the committee, we never received any additional information about such a hearing.
On Monday, I emailed both Khan and her staff, and Senator Michael Barrett, committee Senate chair, and his staff, asking whether an oversight hearing on the Perry case is still planned and, if not, why it had been cancelled. To date, I’ve received no response to those queries.
