Archive
The federal government’s cruel pursuit of deinstitutionalization
When is the federal government — particularly the Department of Justice — going to recognize or admit that deinstitutionalization of the developmentally disabled hasn’t worked as planned?
The DOJ seems to have closed its eyes to the realities on the ground in continuing to file lawsuits around the country to close state-run care facilities. This has caused “human harm, including death and financial and emotional hardship,” according to information compiled by the VOR, a national advocacy organization for the developmentally disabled and a COFAR affiliate.
While the DOJ has not filed such a suit against the State of Massachusetts, that may be because the state has closed, or is in the process of closing, four out of six developmental centers that were in operation as of 2008. But with two developmental centers remaining as well as other programs that the DOJ considers to be institutional, such as sheltered workshops, Massachusetts could well become a target for a lawsuit at any time.
The VOR filed testimony last month, urging a congressional subcommittee to adopt legislative language that would require the DOJ to do two very commonsense things before filing more lawsuits to close state-run facilities:
- First consult with the residents or their legal guardians “to determine residents’ needs and choices with regard to residential services and supports,” and,
- Second, do not “impose community-based treatment on patients who do not desire it.” This second requirement is consistent with the 1999 U.S. Supreme Court decision in Olmstead v. L.C.
The DOJ’s continued pursuit of class-action litigation to close developmental centers and other facilities has led to the irony that those lawsuits are generally opposed by the families of the residents on whose behalf the suits are ostensibly filed. As U.S. District Court Judge J. Leon Holmes wrote in 2011 in dismissing a lawsuit brought by the DOJ against the State of Arkansas to close the Conway Human Development Center center there:
…the United States is in the odd position of asserting that certain persons’ rights have been and are being violated while those persons – through their parents and guardians – disagree. (U.S. v. Arkansas, June 8, 2011, dismissal order).
Judge Holmes’ decision noted that evidence in the case showed that the parents and guardians of residents of the Conway Center “are overwhelmingly satisfied with the services there and believe that the Center is the least restrictive, most integrated placement appropriate for their children and wards.” Moreover, the judge’s decision stated that the weight of the evidence in the case failed to support the DOJ’s contention that care at the Conway Center was substandard.
The VOR notes that the DOJ’s Civil Rights Division has filed more than 45 legal enforcement actions in 25 states since 2009 to limit or shut down state care. On a website listing all the litigation it has filed, the DOJ includes the heading “Olmstead: Community Integration for Everyone.”
It’s not true, though, that Olmstead requires community-based care for everyone. The Supreme Court decision established a right to community-based housing and care only when:
1. The state’s treatment professionals have determined that community placement is appropriate,
2. Transfer is not opposed by the affected individual, and
3. The placement can be reasonably accommodated, taking into account the resources available to the state and the needs of others with mental disabilities.
Despite those clear conditions, the DOJ has plowed ahead with its community-integration lawsuits under the explicit assumption that all institutional care should be ended and everyone should be sent into community-based care, whether they want to go or not.
This viewpoint by the DOJ is a misinterpretation of the Olmstead decision, and it has had tragic consequences, according to the VOR. The organization pointed out in its testimony that higher mortality rates have been documented in Virginia, Nebraska, Tennessee, and Georgia in the wake of the DOJ’s deinstitutionalization settlements.
Those problems have occurred because so many of the privatized group homes to which the people formerly in the state facilities have been transferred are poorly monitored and are afflicted by high turnover and poor training of staff. Yet, that reality does not appear to have been recognized by the DOJ.
In Virginia, a state sued by the DOJ to close its state-run developmental centers, the risk of mortality for those individuals who left those centers was double that of those who stayed.
In Tennessee, DOJ lawsuits resulted in the closure of one developmental center in 2010 and the downsizing of two others. In that state, deaths among people released from institutions nearly doubled between 2009 and 2013. In addition, according to The Tennessean, a 2013 State Comptroller’s audit reported a lack of access to adequate medical and dental care, incarcerations, and hundreds of reports of abuse, and neglect and exploitation among the transferred developmental center residents.
In Nebraska, a 2014 monitoring team report found that of 47 persons considered to be “medically fragile,” who were transferred from a developmental center in 2009 as a result of a DOJ settlement, 20 (or 43 percent of them) subsequently died.
In Georgia, a 2010 a DOJ settlement agreement required the closure of all state-operated developmental centers and the transfer of 1,000 persons with developmental disabilities as well as 9,000 persons with mental illness from facility-based care. In March, The Augusta Chronicle reported that of 499 individuals with profound developmental disabilities, who had been transferred from the state developmental centers under the DOJ settlement, 62 (or 12%) died unexpectedly.
The Augusta Chronicle article discussed the case of Christen Shermaine Hope Gordon, a 12-year-old girl who died in community-care after being transferred from the Central State Hospital in Milledgeville, GA. The article recounted a litany of poor decisions and poor care that appear to have led to Christen’s death.
In a letter to the DOJ in January of this year, Margaret Huss, president of Intellectual Disabilities Advocates of Nebraska, urged the DOJ to ask critical questions about the mortality figures and other data regarding the transfer to community-based care prior to filing further lawsuits to close state facilities. “An increased risk of death should not be the unintended consequences of the worthy goal of community integration,” Huss’s letter stated. As of May 1, the DOJ had not responded to her letter.
That an increased risk of abuse, neglect, and death exists in community-based care has long been recognized, but few policy makers or people elected to office have been willing to stem the tide of deinstitutionalization. In March 2013, U.S. Senator Chris Murphy of Connecticut did call for an investigation of abuse and neglect in privatized group homes around the country, in response to a series by The Hartford Courant detailing those problems in that state.
In a letter to the Office of the Inspector General in the U.S. Department of Health and Human Services, Murphy termed the level of abuse and neglect in group homes “alarming.” Murphy asked the IG “to focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.”
But more than two years after Murphy’s request, it is not clear that the HHS Inspector General ever did undertake such an investigation. The IG’s office has so far not released a report and did not respond to an email query from us on April 30, seeking information on whether an investigation has been undertaken and what its status might be.
Senator Murphy’s office also did not respond to repeated inquiries from us last week as to whether Murphy ever received a response from the IG to his call for an investigation or whether he ever followed up with the IG after his original request in 2013.
Unfortunately, lawmakers in the U.S. Senate, in particular, have also not been supportive of VOR’s proposed legislative language to require the DOJ to consult with families before filing further lawsuits against state care. While language was inserted in a House appropriations bill for the DOJ last year at VOR’s request that protections for institutional care be considered by the DOJ as appropriate for those who desire it, that language was later watered down.
We can only hope that folks begin to wake up in Washington and elsewhere to overwhelming evidence that deinstitutionalization accompanied by privatization is not working, and that someone finally steps forward to slow both of those trends.
The HW&M budget has great news for sheltered workshops, not so good news for state care in general
The great news is the House Ways and Means Committee re-inserted protective language last week in the proposed Fiscal Year 2016 state budget that would protect vital sheltered workshops from closure.
Representative Brian Dempsey, chair of the committee, who was instrumental last year in keeping the workshops open, has renewed his commitment to those facilities in this year’s budget go-round with the administration.
The bad news is that the House Ways and Means budget continues to squeeze state-run programs for the developmentally disabled and maintains the administration’s disproportionate increase in proposed funding for the corporate, provider-run group home system. But let’s look at the good news first.
Last spring, after a lobbying campaign by advocates of the workshops, Dempsey placed language in the House Ways and Means version of the current-year budget, stating that DDS “shall not reduce the availability or decrease funding for sheltered workshops serving persons with disabilities who voluntarily seek or wish to retain such employment services.” The protective language survived a House-Senate conference committee in June, largely due to Dempsey’s support.
While that protective language in the budget appeared to offer the workshops an indefinite reprieve, the proposed fiscal 2016 budget submitted by Governor Charlie Baker in March removed the language. As a result, the workshop supporters went to work once again in the past month, calling Dempsey’s office and urging their local legislators to reinstate his language.
Dempsey did reinstate the language; and in a conference call last week concerning the House Ways and Means budget plan, DDS Commissioner Elin Howe indicated that the administration did not intend to file any amendments to remove the language from the budget legislation. It also appears that organizations representing corporate DDS providers, such as the Association of Developmental Disabilities Providers, have not filed amendments to close the workshops.
It is now up to the Senate and specifically to Senator Karen Spilka, the chair of the Senate Ways and Means Committee, to follow Rep. Dempsey’s lead and insert the same protective language in the Senate budget.
The workshops first came under attack from the administration of then Governor Deval Patrick, which targeted them for closure as of this coming June, arguing that they were “segregating” disabled persons from their peers in the mainstream workforce. But families of the workshop participants fought back. They maintain that the facilities are fully integrated into the surrounding communities and provide the participants with meaningful activities and valuable skills.
Sheltered workshops provide developmentally disabled persons with a range of assembly jobs and other types of work, usually for a small wage.
Meanwhile, the bad news we were talking about largely concerns funding for DDS group homes, remaining developmental centers, and service coordinators. The House Ways and Means budget proposal would cut the developmental center line item even deeper than Governor Baker has proposed and would reduce the service coordinator line item below the amount proposed by the governor. It would also fund the state-operated group homes at a level below what DDS considers a “maintenance level.”
While the state has closed three of six existing developmental centers since 2008 and is in the process of closing a fourth, funding appropriated to run the remaining three centers may have dropped too fast to maintain existing services in those facilities. As we recently noted, years of cuts in the developmental-center line item have lately resulted in the closing of several cottages at the Wrentham Developmental Center, requiring residents to be moved from long-time residential locations.
The Wrentham Center has become a major destination for persons transferred from the developmental centers that have been closed in recent years.
While Governor Baker’s fiscal 2016 budget would cut the developmental center line item by about $375,000 from projected spending, the House Ways and Means budget would cut it by $1 million beyond that.
DDS-operated group homes would get the same amount in fiscal 2016 under the House Ways and Means budget as under the governor’s version of the budget, which amounts to a $2 million reduction from what DDS considers a “maintenance budget.”
Also, the House Ways and Means budget would fund the DDS line item that pays service coordinators at a level $538,000 less than what Baker has proposed. In March, DDS Commissioner Howe had said Baker’s budget would fund the service coordinator line item at $1.8 million below what DDS had requested. So the House Ways and Means budget further reduces that proposed funding for the service coordinators next year by more than half a million dollars.
The service coordinators, whom Howe has referred to as “the heart and soul” of DDS, are responsible for ensuring that clients throughout the system are receiving services to which they are entitled. The service coordinators have seen their caseloads rise dramatically in recent years.
In last week’s conference call, Howe noted the shortfalls in funding under the House Ways and Means budget for the developmental centers, DDS-operated group homes, and service coordinators. But in what may be a sign of the priority that this administration places on these services, Howe said the Department did not plan to seek amendments to the House budget to increase that funding.
At the same time, the House Ways and Means budget preserves a major funding increase to the corporate providers in the coming fiscal year. The Ways and Means plan provides for the same $35 million increase from the current year for the DDS corporate residential line item that Baker has proposed. As of July, this line item will have been increased by more than 28 percent since the filing of a lawsuit by the corporate providers in June 2014 against the then Patrick administration.
While we understand that direct-care workers in corporate, provider-operated group homes are woefully underpaid, it’s not clear how much of the additional funding being sent to the providers is, or will be, going to those workers. As we have noted, the hundreds of executives working for those provider agencies in Massachusetts have been making out quite well.
The Baker administration is apparently fine with that state of affairs. Terming the House Ways and Means plan “a very reasonable budget,” Howe pointed out that it would add $17 million to the DDS bottom line compared to the governor’s budget. Under the House Ways and Means budget, the Community Day and Work line item would be almost $10 million higher than what the governor proposed.
The House Ways and Means budget also would provide $12.4 million under a new DDS line item to implement the expansion of DDS eligibility to people with autism, Prader-Willi, and Smith-Magenis Syndrome.
While that expansion of eligibility funding is certainly needed, the Senate has a lot of other work in store for it as well. We hope that in addition to protecting the sheltered workshops, the Senate begins to address the imbalance in the budget between corporate and state-run DDS care.
Human service providers’ lawsuit boosts their state funding despite deficit
While programs and services are being cut throughout state government as a result of projected budget shortfalls, corporate human services providers have gotten hundreds of millions of dollars in additional state funding due, at least in part, to a lawsuit they filed against the state.
The irony is that the U.S. Supreme Court has just ruled in a separate case that providers cannot sue to raise Medicaid service rates. So, it’s not clear to us that the Massachusetts providers were on solid legal ground in filing their lawsuit.
In June 2014, the providers sued the then Patrick administration, arguing that the administration was not boosting state funding to them fast enough to satisfy a timetable set in a 2008 law known as Chapter 257. Chapter 257 established formulas and timetables for increasing provider funding rates.
As a result of the lawsuit, both the Patrick administration and the incoming Baker administration approved major funding increases to the provider-run group-home line item in the Department of Developmental Services budget, even as it was becoming clear the state was facing major budget shortfalls in the current and coming fiscal years.
In a press release issued on March 4, the day he submitted his Fiscal Year 2016 budget to the Legislature, Governor Baker stated that his administration had allocated $30 million “to resolve litigation and adjust Chapter 257 rates for human service providers.”
The $30 million referred to in the governor’s press release may have understated the impact of the lawsuit. Baker’s proposed funding for the provider group-home line item in the DDS budget for fiscal 2016 is more than $230 million higher than the amount appropriated for that line item in fiscal 2014 when the provider lawsuit was filed. That is a 28 percent increase.
In contrast, the line item for the state developmental centers would be cut in that same period by almost 9 percent, and state-operated group homes would get an increase of about 13 percent in that time period.
In what sounds like a similar lawsuit to the the litigation in Massachusetts, service providers in Idaho had argued in federal court that Idaho had failed to raise Medicaid payments to them as outlined in a federally approved formula. But the U.S. Supreme Court ruled on March 31 that private providers cannot sue for higher Medicaid reimbursement rates.
In the suit filed by the Massachusetts providers, state Superior Court Judge Mitchell Kaplan ruled in January that the state had violated Chapter 257 by not setting higher rates for providers. In response to the suit, the then Patrick administration had initially argued that Chapter 257 could be fulfilled only if the state itself had adequate revenues to do so.
But Judge Kaplan ruled that the state had to comply with the higher rates required under Chapter 257 regardless of whether the funding was available or not. That would mean that in order to fulfill the requirements of Chapter 257, funding would have to be cut in other areas, which is what has happened.
Like the Idaho providers, the Massachusetts providers had argued that the inadequacy of the state funding was causing them to fail to keep up with rising costs and was resulting in lower paid staff and high staff turnover as well as poorer quality services. We have maintained, though, that the funding has been adequate to support high salaries for executives running the provider corporations. Close to $100 million a year is spent on those executive salaries in Massachusetts.
As we’ve noted before, the major funding increases in the provider line item in the past year have increased an already existing imbalance in funding between that line item and accounts for state-run services.
One example of that imbalance is the state-run developmental center line item, which will be some $10.6 million less under Baker’s fiscal 2016 budget than it was in fiscal 2014. This has led to the necessity of closing several cottages at the Wrentham Developmental Center in the past several months, requiring residents to be moved from long-time residential locations.
An April 2 memo sent to Wrentham Center staff referred to an “immense challenge” in meeting budget constraints facing the Center in the current fiscal year, and a “yet another difficult budget forecast for Fiscal Year 2016.”
At the time the Massachusetts providers filed their suit, a spokesman for the providers explained that they had rejected an offer from the then Patrick administration to meet them more than part-way by providing 90 percent of the full funding increase specified under Chapter 257 as of January 2015.
“…in the end, it wasn’t enough,” the spokesman for the providers said. “At this point, we’ve been as patient as we can be and the law is the law and we want the Commonwealth to abide by the law. Every day that full implementation is delayed, the imbalance and the unfairness grows.”
The providers and the Baker administration, however, do not seem to be as concerned about the continuing and growing imbalance in funding between provider and state-run services.
Following the money on three new DDS-related laws
More than five months ago, three important pieces of legislation affecting people with developmental disabilities were ceremonially signed into law with a lot of fanfare by then Governor Patrick; but there has been little information since about the status of these new laws.
We are attempting to find out via Public Records law requests to the Department of Developmental Services what is being done to implement these laws, how much it all will cost, and where the money is going. The Department does not seem eager to part with that information voluntarily.
1. National Background Check law: This new law authorizes national criminal background checks for persons hired to work in an unsupervised capacity with persons with developmental disabilities. It will ultimately require that both current and prospective caregivers in the DDS system submit their fingerprints to a federal database maintained by the FBI.
We previously reported that the requirements under this law have been delayed by up to four years.
On March 2, we sent in information request to DDS, asking what steps the Department had taken to implement the law and whether the Department has finally applied for grant funds available since 2010 from the federal Centers for Medicare and Medicaid Services under the Affordable Care Act to design a national background check program.
To date, despite a follow-up email on March 30, we have received no response from the Department to our questions. As a result, we submitted a Public Records request to the Department on March 31, asking for all reports, memoranda, and other records that concern those issues. Legally, state agencies do not have to respond to information requests, but they do have to respond within 10 days to requests for public records.
More than a year and a half ago, a DDS administrator said the Department had not applied for an ACA grant, which can be as high as $3 million per state, because the legislation authorizing national background checks in Massachusetts had not yet been passed.
2. The ‘Real Lives’ law: This law introduces what is called “person-centered planning” in providing care and services to persons with developmental disabilities.
On March 3, we submitted a Public Records request to DDS, seeking records pertaining to all payments made by the Department in Fiscal Years 2014 and 2015 to a company called Public Partnerships, LLC. According to a DDS website PowerPoint document, Public Partnerships has begun contracting with DDS to provide “individualized fiscal intermediary” or financial management services to participants in the Real Lives program.
While the Real Lives law is touted as providing individuals with more choice and “self determination” in the services they receive from DDS, we are concerned the law will transfer decision-making authority from guardians and family members of disabled individuals to private financial management companies.
Thus far, it is unclear exactly what services Public Partnerships has or will provide under the law and how much it has or will be paid to do so. The DDS PowerPoint states that the financial management services “may include” fiscal accounting, tax withholding, criminal background checks, and other services. The PowerPoint provides no specifics, however.
As of early March, it did not appear that DDS had yet developed policies or regulations regarding the Real Lives law, and more specifically concerning the nature of the financial management services that will be used under the law. The most recent policy statement from DDS concerning “self-determination” is dated January 2010.
Public Partnerships is not new to contracting with DDS. The firm received $14 million in funding from DDS in Fiscal Year 2014, according to an online state site that tracks spending on human services contractors. It was not clear what services Public Partnerships provided to DDS in fiscal 2014.
The state’s Open Checkbook website listed a total of $10.9 million in DDS payments to Public Partnerships so far in the current fiscal year. The website, however, also does not specify the services provided for that funding.
Public Partnerships bills itself on its website as “a full-service financial management services firm dedicated solely to providing fiscal/employer agent, third party administrator, and related support services to public agencies.” The site adds that the firm helps state, county, and local public agencies “implement a participant-directed service model.”
Audited financial statements for the company and a Colorado affiliate, available on the state contractor site, disclose that Public Partnerships and its Colorado affiliate received more than $1 billion in total revenues in fiscal 2014. Public Partnerships is a subsidiary of Public Consulting Group, a Boston-based consulting firm, which has received $3.3 million so far in the current fiscal year from several agencies in the Executive Office of Health and Human Services.
3. The DDS eligibility law: In September 2014, we first asked DDS for information on the funding available to carry out this new law, which requires that the Department expand services to include persons with autism and conditions known as Prader-Willi and Smith-Magenis Syndrome. We received no response to that request for information.
Then on March 2 of this year, we sent an email to the DDS commissioner, asking whether the Department has developed a cost estimate for expanding services under the new law and what that estimate might be. Having received no response to that question, we have asked in a Public Records request for reports, memoranda, and other documents that concern the potential cost of the new law.
You may wonder why we have even bothered to send information queries to DDS, given that they don’t seem to respond to them. The answer is they have, at times, responded to those queries. In the past year or so, it seems, they’ve stopped responding. It’s hard to say why. Maybe they they’ve adopted a new policy of circling the wagons and cutting off information.
Guardian rights bill would help families caught in the DDS-probate system
As we have chronicled a number of times, family members can get shut out of the process when their loved ones with developmental disabilities enter the state’s system of residential care.
This is particularly the case when family members lose their legal status as guardians of disabled persons. That, as we have seen, can happen for reasons that are not always fair or just.
That’s why we strongly support a bill (H. 1459) now before the state Legislature that would require probate court judges to give more consideration than they now do to the appointment of family members as guardians of incapacitated persons.
The bill, which has been filed for years by Representative David Linsky, has never made it out of committee. We understand, though, that the Massachusetts Developmental Disabilities Council, which advises the state on issues of concern to the developmentally disabled, has put this bill on their priority list for passage this year.
The bill states that the spouse, parent or parents or their designees of an incapacitated individual should be presumed to be suitable guardians unless competent evidence is introduced to the contrary.
Obtaining guardianship when a developmentally disabled person reaches the age of 18 is essential in participating in the care of that person. Guardians have legal rights to participate in individual support planning, a key element in the care of developmentally disabled persons, and to make other decisions that affect their wards’ services and well-being. Even the parents of a developmentally disabled person over 18 will find they have virtually no say in that person’s care if someone else is appointed as his or her guardian.
But the appointment by probate court judges of guardians of developmentally disabled persons is often haphazard. In many of those cases, judges appoint either attorneys or corporate human services provider organizations as guardians, and those attorneys or providers may have no connection to the persons who need their representation.
Attorneys, corporate providers, and others who are appointed to guardianships of developmentally disabled persons are generally paid for those services by DDS. According to DDS records, eleven of the 20 highest-paid guardians by the Department in Fiscal Year 2014 were either corporate providers or attorneys.
There seems to be a view among at least some judges and within DDS that corporate providers or attorneys make more suitable guardians than do family members, particularly if those family members are seen as aggressive or contentious in their relationships with DDS. We think this dismissal of families is wrong and has caused a lot of needless suffering among families, not to mention hindering adequate care.
Moreover, the view that the so-called experts and not family members know what is best for disabled persons appears to be at odds with the federal Developmental Disabilities Assistance and Bill of Rights Act, which states that family members of developmentally disabled individuals shall be the “primary decision-makers” in the care of such persons.
It would seem that too few people in DDS or the probate court system in Massachusetts are familiar with the DD Assistance and Bill of Rights Act.
In 2012, DDS petitioned a probate judge to remove Patricia Feeley as her son’s guardian because Feeley would not agree to a Department plan to place her son in a residential care setting without 24-hour nursing. DDS agreed to dismiss its petition a year later, but only after the Department had proposed to appoint a Woburn-based attorney, who had never met Feeley’s son, as his guardian.
In 2010, Norfolk County Probate Court Judge George Phelan dismissed the entire Duzan family as unsuitable to continue as guardians for Sara Duzan, a young woman with a developmental disability who had been repeatedly abused with unnecessary restraints in a series of provider-operated residential care settings.
In his order, Phelan discounted the family’s claims that Sara was being abused, and contended the family itself had “demonstrated through a variety of encounters their vacillation, indecisiveness, and inability to work with others.” In the place of Sara’s family, Phelan appointed the executive director of the Arc of Greater Fall River, a DDS corporate provider, as her guardian.
Phelan’s order set the stage for the eventual cutoff of all contact between the family and Sara for months, and forced them into an expensive and still ongoing legal battle over her custody. But vacillation, indecisiveness, and even the inability to work with others, even if that were the case, do not seem to us to be sufficient reasons to deny an entire family the right to guardianship of a loved one.
In a third case, Stan McDonald voluntarily relinquished his guardianship nearly 30 years ago of his intellectually disabled son, Andy, as part of a custody battle with his former wife. What followed were years, with few exceptions, of poor decision-making regarding Andy’s care by a number of court-appointed guardians.
The idea for H. 1459 came from Stan McDonald, who has still been unable to regain his guardianship of Andy, and has had to watch helplessly as Andy’s emotional needs have been ignored or neglected. Andy McDonald’s current court-appointed guardian has had as many as 100 wards at one time. The provider executive director appointed as guardian of Sara Duzan had 24 other wards at the time, according to court records.
The current probate law does state that in appointing guardians, the court should consider, in order of priority, a spouse, then a parent, and then “anyone else the court deems appropriate.” But a judge is not obligated to give more weight to a parent than to anyone else he or she deems appropriate.
In fact, the current probate law goes on to state that: “The court, acting in the best interest of the incapacitated person, may pass over a person having priority and appoint a person having a lower priority or no priority.” That provision gives probate judges carte blanche to bypass the express wishes of parents and other family members. H. 1459 would remove that provision.
There are a number of additional reasons to support of H. 1459:
- It would lower caseloads for attorneys who are not able to advocate effectively for the often large numbers of incapacitated persons for whom they are responsible. It would also reduce the cost to taxpayers in paying these attorneys.
- H. 1459 would also reduce the use of scarce court resources expended on families disputing the appointments of non-family members to be guardians of their loved ones.
By itself, H. 1459 is just one of a number of measures that are needed to reform the dysfunctional DDS/probate court system of care for people with developmental disabilities. Other measures are needed as well. For instance, there should be a mediation process available in guardianship disputes so that families are not forced to impoverish themselves in court litigation when they do lose their guardianship rights.
In the absence of a mediation process, the state should be required to appoint an attorney to represent an individual who gets involved in a dispute with the state over guardianship and can’t afford an attorney on their own.
Also, in light of the Developmental Disabilities Assistance and Bill of Rights Act, family members and other caring individuals should have standing to advocate for an individual even if they are not the person’s guardian. And limits are needed on the number of persons that individual attorneys, corporate guardians, and others should be allowed to represent as guardians.
Baker administration continues Gov. Patrick’s misguided effort to close sheltered workshops
As the Legislature takes up Governor Baker’s budget for the coming fiscal year, it looks as though the battle over sheltered workshops for the developmentally disabled in Massachusetts is set to begin once again.
Supporters of these vital programs won a reprieve last year when the Legislature inserted protective language for the workshops in the current-year budget. The language prohibits the Department of Developmental Services from closing or cutting off funding for sheltered workshops as long as there are people who seek them or wish to remain in them.
The budget language temporarily thwarted the efforts of then Governor Patrick to close all remaining sheltered workshops in the state as of this coming June. But the protective language has been removed from Governor Baker’s proposed budget for fiscal 2016.
It appears that despite the fact that we have a new governor, it is the same DDS with the same administrators running it; and they will never back away from their ideological opposition to any program that serves more than a handful of disabled individuals in one location.
Sheltered workshops provide settings in which developmentally disabled people can do assembly jobs and other types of work. In the view of the now Baker administration, such settings of care “segregate” developmentally disabled people from their non-disabled peers, and supposedly prevent them from reaching their potential in the mainstream workforce.
Many families and guardians of workshop participants, however, want these programs to continue and depend on them to provide valuable skills and meaningful activities to the participants.
Last spring, after a lobbying campaign by advocates of the workshops, language was inserted into the current-year budget, stating that DDS “shall not reduce the availability or decrease funding for sheltered workshops serving persons with disabilities who voluntarily seek or wish to retain such employment services.” The protective language survived a House-Senate conference committee in June, largely due to the support of House Ways and Means Chair Brian Dempsey.
But Governor Baker’s budget has not only removed that language protecting the workshops, the budget proposes a $4 million increase in a separate DDS account to move people from sheltered workshops into DDS day programs, many of which do not provide work-related activities.
We support the continued operation of sheltered workshops for reasons given in an email sent to Dempsey last May by Richard Urban, who is a guardian of his brother Tom. In December 2013, DDS closed Tom’s sheltered workshop where he had been employed for most of his adult life. Richard noted that Tom’s “work ethic and paycheck (from his sheltered workshop program) were two constants that allowed him a place on a playing field of equality with his peers, family and friends.”
Since his “forced exit from his workshop,” Richard said, Tom “has grown distant, is very confused, and expresses continued sadness over his job loss. His identity, and work community, have been lost, through no fault of his own but by virtue of a policy shift for which I am at a complete loss to understand.”
We’re at a loss to understand it as well.
Two lawmakers support an independent evaluation of Andy McDonald
More than a year ago, we asked for an independent clinical evaluation of a now 47-year-old intellectually disabled man, who has not been permitted to visit his parents in their Sherborn home for the past 19 years because he has been deemed to be a danger to the community.
Finally, two state legislators are asking for the same independent evaluation of Andy McDonald. In a letter sent to the Department of Developmental Services on February 25, both Senator Richard Ross and Representative David Linsky further asked that the evaluation take into account the views of Andy’s father, Stan, and his step-mother, Ellen, who have been fighting for years for supervised visits home for him.
Not only is Andy prohibited from visiting the home he grew up in; Stan and Ellen are not even permitted to discuss the topic with him. Under the rules imposed by his DDS-funded group home, Andy, who has frequently expressed a longing to see his home again, is forbidden from mentioning his desire to do so. It seems like a violation of free speech; but then again, when you are under the control of both the DDS and probate court system, your right to self-determination becomes very limited.
That loss of self-determination may be appropriate in some cases; but the McDonald case shows how dysfunctional the system can get. The case is replete with questions about the validity of previous clinical evaluations of Andy and about a 2006 probate court ruling, which concluded that Andy was sexually dangerous and should never be allowed to return home.
In the 2006 ruling in which he denied Stan’s bid for guardianship of Andy, Middlesex County Probate Court Judge Edward Rockett stated that Andy had been arrested in 1990 for sexual assaults of three young girls who lived across the street in Sherborn. That was not true, however.
Andy was arrested in May 1990 for threatening an unidentified person during a telephone call, according to the district court record. The nature of the threats was not disclosed. In July of that year, he was arrested for disturbing the peace in downtown Sherborn and with assault for punching his stepmother, according to a police report. Both Stan and Ellen say the punch was accidental and occurred while Ellen was driving Andy to the police station after he was accused of disturbing the peace. “He was flailing his arms, not threatening me,” Ellen said in an email this week, “and his fist landed on me. It didn’t hurt me. It made a red mark that faded shortly after.”
There is no indication in the police reports that Andy ever sexually assaulted anyone.
In his ruling, Rockett also cited a statement by the clinical director of Andy’s group home that Andy had told him he had had sexual fantasies about children. But Rockett acknowledged in his ruling that there was testimony in the court case that Andy “will always say what he thinks other people want to hear. This causes his statements to be very inconsistent.”
As we noted in a previous post about this case, Andy was committed to McLean Hospital in Belmont immediately after the July 1990 threatening and disturbing-the-peace incidents. In the years following, he was subjected to a series of inappropriate residential placements and treatment, in many cases because a series of court-appointed guardians, state agencies, and providers made the wrong decisions regarding his care.
Most of the decisions about placement and treatment of Andy were made without the consent of Stan, who had agreed to the appointment of a guardian for Andy in 1986 as part of the settlement of a longstanding custody battle over him with his former wife. Andy has had a series of court-appointed guardians since, and Stan has never been able to regain that guardianship. His attempts in probate court to do so have been opposed by DDS.
Andy has not exhibited any significant behavioral problems in a decade and has been taken on community outings to many places other than his home without any behavioral incidents, according to Stan and to notations in Andy’s clinical care plan. But that record of good behavior does not appear to have changed the position of either the probate court, DDS, or Andy’s current court-appointed guardian that he must never be allowed to go back to his hometown.
That ban on visits to Andy’s boyhood home combined with his group home’s policy that he must not even discuss his desire to visit his parents there amounts to psychological abuse, Stan maintains. Moreover, the situation raises concerns in Stan’s and Ellen’s minds about Andy’s future and what will happen when they are no longer able to travel from Sherborn to visit him in his group home in Northborough. Stan is 79 years old.
In 2000, Ronald Ebert, a psychologist, recommended that the staff of Andy’s group home try a “trial visit” to the Sherborn Inn to hear Stan, an acclaimed jazz musician, play in his band if it could be demonstrated that the persons Andy was accused in 1990 of threatening no longer lived in town. In fact, Stan says, those persons had moved away as of that time. “If such visits can be managed successfully, there is no reason why they could not be built into his visit schedule…,” Ebert wrote. But Ebert’s recommendation was never heeded.
As is the case with he parents of Sara Duzan, who were denied all contact with their daughter for several months, Stan and Ellen McDonald have found themselves trapped in a Twilight-Zone-like situation imposed on them by the state’s dysfunctional human services and probate court system. It’s long past time to bring in someone with a truly independent view to take a new look at this case.
Budget reductions falling heavily on state-run services for the disabled
During a conference call on Wednesday with advocates for the developmentally disabled, Department of Developmental Services Commissioner Elin Howe didn’t have much good news about the potential impact of Governor Baker’s proposed Fiscal Year 2016 budget.
The budget is bad news for DDS accounts, particularly state-operated services.
“These are huge and difficult reductions,” Howe said.
Baker is dealing, of course, with a projected budget shortfall in the coming fiscal year, and it looks as though people with intellectual and developmental disabilities are among those who will pay a price for that shortfall. Howe said DDS is assuming departmental layoffs will not be necessary if the Legislature accepts Baker’s early retirement proposal for state workers. If that doesn’t happen, measures such as layoffs may be needed, she said.
Just about every DDS account is being funded lower than what DDS had asked for. Howe said the governor’s budget required a total of $27 million in reductions from DDS funding requests, but DDS has been able to reduce the hit by $8 million by using some federal revenues as an offset to the total reductions.
As usual, state-operated services may be taking the brunt of the reductions. Howe noted that Baker was proposing a $2.6 million reduction from the DDS request in the state-operated group homes line item. Under Baker’s budget, the line item would be increased by $5.1 million, from current-year spending (from $209.6 million to $214.7 million). But that amount is below what DDS considers necessary to maintain current services.
Exactly what the state-run group home line item reduction means is unclear. Howe said DDS is not projecting “reductions in services to people,” but rather there will be “changes in staffing.” Among other things, DDS has been working to reduce the use of overtime in state-operated group homes, she said.
In January, we sent a letter to Kristen Lepore, Baker’s new secretary of administration and finance, asking that the new administration consider making the funding of state-operated care for the developmentally disabled a priority. For too long, as we noted, state government has been divesting itself of its responsibility to provide care for the most vulnerable of its citizens, and has failed to adequately monitor and control the handover of human services to state-funded corporate providers.
Baker’s first budget does not appear to address that situation.
In addition to the shortfall in funding for state-operated care, Howe said the state-run developmental centers line item would be funded under the governor’s budget at $2 million less than what DDS was requesting. This account would be cut from the level of spending in the current fiscal year as well, under Baker’s budget.
In addition, DDS service coordinators, Howe said, were being funded at a level $1.8 million below what DDS had requested. The DDS administrative line item, which funds the service coordinators, would be increased under Baker’s budget, but not by enough to maintain current services.
Corporate provider-run care does not come through unscathed in the governor’s budget, but the overall imbalance in funding between state and provider-operated care will remain.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. In fiscal 2014, then Governor Patrick and the Legislature increased the provider line item by more than $140 million –or more than 16 percent—in FY 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
The provider residential account subsequently received a supplemental budget increase in the current fiscal year of $44.7 million, even as both Baker and his predecessor, Patrick, were cutting spending across the board to deal with a projected current-year budget deficit.
Baker has proposed another $33.6 million increase in the provider residential line item for fiscal 2016, but DDS and the providers apparently wanted $4 million more than that.
Among the other DDS line items:
- Baker has proposed an increase in funding for the day program line item that is $9.7 million lower than what DDS wanted. The line item would be increased by $2.8 million under Baker’s budget proposal.
- Respite and Family Supports would be funded at a level $5 million below DDS’s request. Under Baker’s budget, the line item would be increased by $7.4 million, but this line item has been continually underfunded in recent years. It was cut in the current year by $2.5 million in light of the projected budget deficit.
- The transportation line item would receive a $3.5 million increase under Baker’s budget, but that increase was $3 million below what DDS wanted.
- The Autism and Turning 22 accounts would be level-funded, which amounts to a cut when adjusted for inflation.
- A long-time revenue account of $150,000 from sales from the dairy barn at the Templeton Developmental Center would be eliminated. The money has been used for program needs at the Center.
The fiscal 2016 budget is now before the Legislature, specifically the House Ways and Means Committee. We understand that this is a fiscally difficult time for all state programs. When it comes to the DDS budget, though, this may be a good time to rethink some longtime funding priorities. We hope key legislators will do just that in coming months.
Public Health Department needs to release report on death of developmentally disabled man
The Department of Public Health has completed an investigation of the case of a developmentally disabled man who died en route to Lowell General Hospital in February 2012 after having been turned away from the hospital twice without any significant treatment.
We may never know, however, what the result of the investigation is. The Department, citing the deceased man’s privacy rights, won’t release the report.
We are appealing this denial to the state’s Public Records Division, arguing that the potential public interest in knowing what happened in this case outweighs the privacy rights of a deceased individual. Our view is that the real potential wrong to this person was done when he was denied treatment by the hospital. The public, we think, deserves to know what happened here and so do persons with developmental disabilities and their families and guardians.
This case suggests possible inadequate training of health care personnel in the treatment of developmentally disabled persons, which is an issue of concern to advocates for the disabled and to many policymakers.
The National Council on Disability, with which we have had our disagreements, maintains that:
The absence of professional training…for health care practitioners is one of the most significant barriers preventing people with disabilities from receiving appropriate and effective health care.
The man was a former resident of the Fernald Developmental Center. He had been living in a group home in Chelmsford and was attending a day program in Lowell on the morning of February 6, 2012, when the staff at the day program made the first call to 911 to take him to the hospital. He had reportedly been having difficulty breathing and was sweating profusely. The hospital released the man shortly after his arrival, however, and sent him back to his group home, according to sources.
By about 8 a.m. the following morning, the man was slumped over in his wheelchair and sweating heavily, a source said. A group home staff member called 911 shortly afterward.
A Disabled Persons Protection Commission (DPPC) complaint form stated that the man was observed at the hospital on the morning of February 7 to be sweating profusely, but his vital signs were good when he arrived. According to the complaint form, the man was sent home with a prescription (the name of which was redacted). According to sources, this was the second time he had been sent away by the hospital.
The DPPC complaint form stated that shortly after arriving back at the group home, the man began to vomit and then lost consciousness, and that the staff began mouth-to-mouth CPR until paramedics arrived. The group home received a call from the hospital later that afternoon that the man had died.
Because the man’s death appeared to have been connected with his treatment or lack of treatment by the hospital, the DPPC referred the case to the Department of Public Health for investigation.
Did the apparent failure of Lowell General Hospital to properly diagnose this man’s illness and provide him with adequate treatment result from a lack of training in disability issues? Did the Public Health Department consider that question in their investigation of this case? Unless the Department releases its report, we will never know the answers to those questions.
While the Public Health Department’s position is that a state law [(M.G.L. c. 66A, s. 2(k)] prohibits them from releasing medical information about an individual, even if that person is deceased, we are not in agreement with their interpretation.
First, there do not appear to be consistent policies among state agencies in releasing investigative reports on deaths of developmentally disabled persons. The Disabled Persons Protection Commission (DPPC) has released a number of these reports to us after redacting what they considered to be identifying information.
Secondly, while we have blogged about this case, we have never used the name of the individual involved or tried to publicly identify him. A Department of Public Health attorney wrote to us, though, that even if we did not use the individual’s name in a blog post about the investigative report, “it is possible for someone to utilize the information that is available (age and date of death) and potentially come up with the patient’s name.” While that is possible, we do not understand why anyone would do that in this case. It seems farfetched.
Third, even if it were true that someone might reveal the identity of the individual involved, there appears to be case law that limits privacy rights of deceased individuals. A Hofstra Law Review article notes that “while postmortem medical confidentiality exists, it is much narrower than the privacy protections guaranteed to the living.” In Massachusetts, case law involving privacy rights after death does not appear to have been settled. (See Ajemian v. Yahoo!, Inc.)
Finally, the privacy statute cited by the Public Health Department [(M.G.L. c. 66A, s. 2(k)] states only that the Department must:
maintain procedures to ensure that no personal data are made available in response to a demand for data made by means of compulsory legal process, unless the data subject has been notified of such demand in reasonable time that he may seek to have the process quashed.
This seems to imply that the person involved has to be living. And, as attorney Steve Sheehy notes in a comment to this post below, at most this statute would require notice to the deceased person’s executor or representative.
Prior to filing our appeal, I asked the Public Health Department attorney whether it might be possible to provide us with a copy of the investigative report with explicit personal data or medical information redacted. As I noted, our interest is whether the Department has investigated or commented on the hospital’s procedures for training staff to treat persons with developmental disabilities.
To the extent that the Department’s report addresses hospital policies and procedures in this case, it would probably not be necessarily for us to know specific medical details about this individual. To date, I have not received an answer from the Department to my query.
Unfortunately, this is not an isolated case of apparent institutional secrecy. When it comes to deciding whether to make public reports of potential mismanagement by human services or health care facilities, the natural instinct of public managers and administrators seems to be to keep it all secret and cite privacy rights as the reason. That has certainly been the practice at the DPPC, but at least, as noted, the DPPC has released redacted reports.
We hope the Public Records Division, which is part of the office of Secretary of the Commonwealth Bill Galvin, will make the right decision and order the Public Health Department to make known the results of its investigation of this troubling Lowell General Hospital case.
Compensation of provider executives in MA reaches $100 million
More than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation, according to our updated survey of the providers’ nonprofit federal tax forms.
By our calculations, state taxpayers are on the hook each year for up to $85 million of that total compensation.
We reviewed the federal tax forms for some 300 state-funded, corporate providers, most of which provide residential and day services to persons with developmental disabilities.
The following is a summary chart of our latest survey results (click on the chart to enlarge):

For the complete survey chart, click here.
We first released our survey about a year ago, when we found that more than 550 executives working for some 250 state-funded corporate providers of services to people with developmental disabilities in Massachusetts received a total of $80.5 million in annual compensation.
COFAR has also previously raised concerns that increasing amounts of money going to provider executives have not translated into higher pay for direct-care workers in Massachusetts.
The latest survey reports on 635 executives who received total annual compensation of $102.4 million and average annual compensation per employee of $161,231. The survey was based on provider tax forms filed in either the 2011 or 2012 tax years. Those tax forms are available online at www.guidestar.org.
The survey sample included 100 CEO’s and presidents, making an average of $210,227 in salaries and benefits; and 107 executive directors receiving an average of $130,835 in compensation. As the chart above shows, the survey also included 67 chief financial officers, 31 chief operating officers, 100 vice presidents, 110 directors, and 120 other officers, all earning, on average, over $100,000 a year.
A state regulation limits state payments to provider executives to $158,101, as of fiscal year 2013. Money earned by executives above the state cap is supposed to come from sources other than state funds.
Based on this regulation, we calculated that provider executives are eligible for up to $85 million a year in state funding to cover those total salary and benefits costs. Our calculation was based on identifying the companies paying executives at or above the state threshold of $158,101, and assuming that amount as the maximum state payment for each of those companies’ executives.
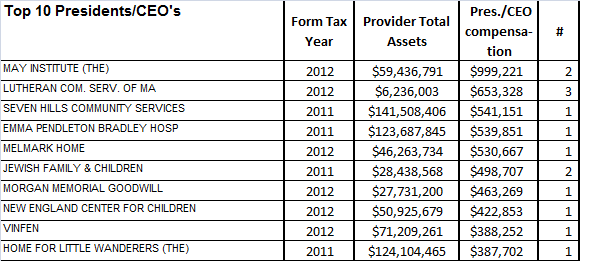
Among the top-paying providers in our latest survey was the May Institute, which paid two employees a total of $999,221 in the 2012 tax year. Both employees were listed as president and CEO of the provider. The May Institute’s federal tax form shows that one of the two employees, Walter Christian, worked for the company until December 2012 and received a total of $725,674 in salary and benefits in that tax year, which started on July 1, 2012. Christian was replaced as president and CEO by Lauren Solotar, who received a total of $273,547 in that same tax year, which ended on June 30, 2013.
Despite the regulation capping compensation payments by the state, the state auditor reported in May 2013 that the state had improperly reimbursed the May Institute, a corporate provider to the Department of Developmental Services, for hundreds of thousands of dollars paid to company executives in excess of that cap. COFAR had previously reported in 2011 that the state may have paid Christian and other executives of the May Institute more than the state’s regulatory limit on individual executive salaries.
The following charts show the top earning presidents/CEO’s and executive directors in our latest survey and the number of those executives holding each title in each company:

Most of the providers surveyed are under contract to the Department of Developmental Services, which manages or provides services to people with intellectual disabilities who are over the age of 22. The providers operate group homes and provide day programs, transportation and other services to tens of thousands of intellectually disabled persons in the DDS system.
As we have noted, the state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in fiscal 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
More financial information about nonprofit corporate providers, including compensation of executives, can be found at www.guidestar.org.
