DDS mortality reports show a rise in deaths in the community system since 2008
If you do some intensive searching, you may just find a series of what seem to be fairly well-hidden reports on the Department of Developmental Services website that present data on deaths in the DDS system between the years 2001 and 2013.
We did find those reports, and reviewed them going back to 2008, the year the then Patrick administration implemented its “Community First” initiative. Within DDS, the initiative involved a major push to close large state-run developmental centers and to move the residents of those facilities to community-based group homes.
It appears to be difficult from the data in the reports to draw any firm conclusions about the total numbers of deaths in the DDS system, which have fluctuated substantially in years between 2008 and 2013. There was a low of 406 deaths in 2010 and a high of 438 deaths in 2012.
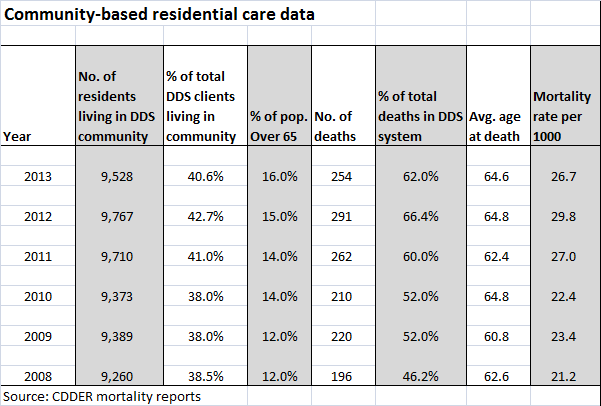
What did appear to stand out in the data was the significantly higher number of deaths in the community residential system in 2013 than in 2008. There were 196 deaths in the community residential category in 2008, and that number rose to 254 deaths in that category in 2013. That was an increase of 58 deaths per year, or about 30 percent.
The number of deaths in the community system rose in three of the five years between 2008 and 2013. There was a slight drop in the number of deaths in the community system in 2010, and a somewhat larger drop in 2013, the latest year for which the mortality reports are available. Nevertheless, the increase in the number of annual deaths between 2008 and 2013 is statistically significant.
We looked at the mortality report data for two other residential categories within the DDS system — people living at home and people in the remaining developmental centers. We did not review report data for two other categories of residential care — nursing homes, which had a relatively small number of DDS clients living in them during the 2008-2013 period, or for settings listed as “non-DDS facilities.”
In contrast to the community residential system, the numbers of deaths in the developmental centers and living-at-home categories decreased fairly steadily between 2008 and 2013.
The percentages of all deaths in the DDS system rose in the community residential category from 46.2 percent in 2008 to 62 percent in 2013, while the percentages of all deaths dropped in that time in the developmental centers and among people living at home. During that time, the percentage of DDS clients living in the community system increased only slightly — by 2.1 percent.
The data raises some questions. Did the closures of the Fernald, Monson, and Glavin developmental centers, starting in 2008, contribute to the increase in the overall death rate in the community system? Were there people living in those centers who died as a result of having been moved into the community system?
The mortality reports, which were done by the Center for Developmental Disabilities Evaluation and Research (CDDER) within UMass Medical School, do not offer any speculation or answers to that question.
CDDER’s 2010-2011 mortality report does offer some speculation about a statistically significant increase in deaths in the community system between those two years. The report states that the increase may have been due to people with “high medical needs” having been moved into the community at that time from nursing homes. But we found no discussion in any of the reports about the potential impact of moving people into the community from the developmental centers.
The CDDER reports also do not appear to differentiate between corporate-provider-run and commonwealth-operated group homes. The community residential category examined in the reports appears to lump both of those types of residential care together. This allows no comparisons to be made between the state-run and privatized group home systems with regard to the mortality rate.
The CDDER reports do provide the average ages of people in each residential setting. But the reports do not compare average levels of intellectual disability or medical conditions in each category. (Some of the reports did compare the medical causes of death in some of the residential settings, but the data didn’t indicate the percentages of residents in each setting with specific medical conditions such as cancer and heart disease.)
There is a lot of important research contained in the CDDER reports, but the omissions are concerning, though perhaps not surprising. CDDER is under contract to DDS to produce the reports, and they are not going to produce or analyze any data that DDS doesn’t want them to produce or analyze.
For years, we have been critical of the ongoing privatization of DDS services. We have raised concerns about the Patrick and now Baker administrations’ policies of under-funding state-operated care, closing existing state-operated group homes, and preventing people from choosing state-operated care as a residential option.
We have also expressed concern that care in the privatized system is not as well overseen as it should be; that staff in provider-run group homes is often underpaid and inadequately trained, and that provider executives are continuing to make huge salaries nonetheless.
We have also been critical of the closures of the developmental centers, which took place in many cases over the objections of the families of the residents in them.
One would think the DDS-sponsored mortality reports would examine the impact of both the developmental center closures and privatization of services on client deaths among other variables. That is, unless DDS would rather not get into those matters. Based on the reports, it would seem that DDS does not want CDDER looking into the impact of increasing privatization, at least on client deaths.
As a result, we can only glean some hints from the CDDER data about those issues.
According to the reports, the community residential system appears to have grown by about 2.9 percent during 2008-2013 period, which makes sense since people were being moved there from nursing homes and from developmental centers.
The data show that the number of residents of the developmental centers dropped from 925 in 2008 to 550 in 2013 — a 44 percent decrease. Given that the number of residents in the centers was dropping so rapidly, the number of deaths among that population was bound to drop as well. There were 49 deaths in the centers in 2008, and 24 deaths in 2013 — a 55 percent decrease.
Among people living at home, the number of deaths also dropped between 2008 and 2013. There were 69 deaths among people living at home in 2013 — a drop of 18.8 percent from the 85 deaths listed in 2008. The total number of people living at home dropped only by 4.3 percent during that period.
Nursing homes and developmental centers had the highest mortality rates per 1,000 clients among the residential settings, according to the 2012-2013 CDDER report. The report explained that the high mortality numbers in those two settings were due to the relatively advanced age of the residents and their relatively serious health conditions.
As noted, however, the mortality reports don’t appear to have compared medical data among residents living in the various settings. The data do show that an average of more than 30 percent of the residents of the developmental centers were over the age of 65 between 2008 and 2013, compared with about 14 percent of residents in the community and 5 percent of DDS clients living at home.
As of 2013, 550 or 2.3 percent of all DDS adult clients were still living the developmental centers. That year, there were 9,528 clients living in the community system, or 40.6 percent of all DDS clients; and there were 11,822 clients living at home, or 50.4 percent of all DDS clients.
In sum, there doesn’t seem to be too much that is surprising in the data, other than the apparent increase in deaths in the community system between 2008 and 2013.
We think it’s possible that those transfers from the developmental centers may have contributed to that increase in deaths in the community system. But given that CDDER does not appear to have collected data concerning deaths of former developmental center residents, we may never know the real impact on mortality of the closures of the centers.
And unless CDDER begins differentiating between provider-run and state-operated group homes, we may never know the impact of increasing privatization on mortality rates in residential care.

I would be curious about the impact of increased community exposure on not just the number of deaths, but, also, on the number of crimes against the disabled who were moved into the community. I expect that in NJ, where the developmentally disabled receiving services from the Division of Developmental Disabilities, are no longer allowed to live in settings where there are more than 25% disabled, and where there are on-site services, the added exposure to those who would take advantage of their vulnerability would increase incidents of victimization.
LikeLike