Archive
Bipartisan support grows for our budget amendments to save Wrentham and Hogan Centers
As the state House of Representatives begins debate today on the Fiscal Year 2027 state budget, we are gaining bipartisan support for our proposed amendments asserting a right of persons with intellectual and developmental disabilities (I/DD) to placements at the Wrentham and Hogan Intermediate Care Facilities (ICFs).
This is a right that not only aligns with federal law, but is consistent with the state’s policy of encouraging “self-direction” among clients in planning and choosing their services.
When it comes to Wrentham and Hogan, not only does the Department of Developmental Services (DDS) not inform disabled individuals and their families of the existence of those facilities, but the Department implies they don’t have a right to placements there.
Wrentham and Hogan are the last two remaining ICFs for persons with I/DD in Massachusetts, and we are concerned that the centers are heading toward closure.
As of today, 12 legislators have indicated their support for Amendment 695, which states that people with I/DD, who have been found to be eligible for ICF-level care, have a right to placement in an ICF residential setting.
A second amendment, which has also gathered the same cosponsors (Amendment 699), requires DDS to report on its efforts to inform families of all residential choices available for care, including ICF care. And a third amendment (Amendment 703) states that residents of ICFs cannot be involuntarily discharged from those facilities.
The cosponsors so far consist of six Democrats and six Republicans, including Republican Representative Marcus Vaughn, the principal sponsor of each of the amendments. Vaughn represents a district that includes the Wrentham Developmental Center.
Among the cosponsors are:
Representative Bradley Jones, a Republican from North Reading, and the House minority leader
Representative Lisa Field, a Democrat from Taunton, who is also a member of the Mass. Nurses Association. The MNA is supporting the effort to keep Wrentham and Hogan open
Representative Sally Kerans, a Democrat from Danvers, in which the Hogan Regional Center is located
Representative John Marsi, a Republican from Worcester
Representative Lindsay Sabasdosa, a Democrat from Northampton
Representative David Viera, a Republican from Bourne
Representative Michael Soter, a Republican from Bellingham
Representative Natalie Higgins, a Democrat from Leominster
Representative Amy Mah Sangiolo, a Democrat from Newton
Representative James Hawkins, a Democrat from Attleboro
Representative Norman Orrall, a Republican from Lakeville
We would urge all 160 House members to support these amendments because the language in them stakes out a commonsense position in favor of individual choice. We have always advocated for a full continuum of care for the most vulnerable citizens among us.
As advocates of the Wrentham and Hogan Centers have long pointed out, one size does not fit all. Community-based group homes can be the best choice for many, if not most, people with I/DD. But for a segment of that population, the community system is either not desired or it cannot meet their complex needs.
There can be no clearer example of that than the case of Kristen Robinson, who has been denied admission to Wrentham even though she is legally blind, quadriplegic, and has profound ID and complex medical issues. No community-based residence or nursing home could or would provide residential care for her.
Kristen was finally admitted to Hogan, after a months-long battle by her family, where she is now thriving.
But Kristen is the exception. Potentially, thousands of persons are waiting in Massachusetts for residential placements, and neither Wrentham nor Hogan is being offered as an option to them.
Questionable claim of cost savings
A series of administrations has long argued that closing congregate care facilities and placing residents in group homes saves money. But this argument is short-sighted and misleading.
As a recent report by our partner organization, the Saving Wrentham and Hogan Alliance, has shown, comparisons of the cost per resident of group home and ICF residents are comparisons of apples to oranges. ICF costs are reflected in the ICF line item in the state budget each year. Those include staffing costs, clinical care, food, housing, and facility costs.
In contrast, the costs of serving people in group homes show up in several state and federal budgets, including MassHealth, Housing and Urban Development (HUD) subsidies and in SNAP benefits, in addition to the DDS community residential line item.
The Saving Wrentham and Hogan Alliance report makes the overall point that the community-based group home system incurs an estimated $1.3 billion in taxpayer costs each year that are not included in the overall $3.3 billion DDS budget.
The DDS line item for corporate group home providers has doubled from a decade ago to more than $2 billion in the current fiscal year. During that same period, the line item for the Wrentham and Hogan facilities has declined by about 14% to roughly $130 million.
So where is the savings in closing ICFs and placing people in the group home system?
Right to an ICF
The assertion in Amendment 695 that ICF-eligible individuals in Massachusetts have a right to placement in an ICF aligns with the establishment of that right in the federal Medicaid Law and regulations.
The landmark Boulet v. Cellucci federal court decision (107 F. Supp. 2d 61 (D. Mass. 2000) cites the Medicaid statute (42 U.S.C., § 1396a(a) (8)), and explicitly states, “…to the extent that the plaintiffs have requested ICF/MR (now ICF/IDD) services, the state must provide those services reasonably promptly.”
The Boulet decision, which was written by U.S. District Court Judge Douglas Woodlock, required DDS to provide residential services promptly to thousands of clients who had been waiting for placements, in some cases for years. Unfortunately, the decision hasn’t led to a resolution of the problem. Not only are people still waiting months or years for placements, but DDS is badly underutilizing its state-run residential resources, which could help mitigate the problem.
DDS’s policy of personal choice
The right to choose an ICF also aligns with DDS’s stated policy that individuals and their guardians should be able to “self-direct” their care. The DDS’s Self-Directed Services website page contains the following statement:
DDS helps an individual to have more control in their life and to make decisions about services based on their vision, path, preferences, beliefs and abilities. The individual decides who helps them and how they want that help to be provided, based on what they want in life and their personal goals.
Placement in an ICF should be a part of that choice.
Connection to fight to preserve Pappas
Finally, we believe there are a number of parallels between the Healey administration’s reported policy of restricting admissions to the Pappas Rehabilitation Hospital and its policy of denying most requests for placement at Wrentham and Hogan.
In sum, our budget amendments are intended to preserve choice and to ensure respect for the wishes and preferences of DDS clients and their families. We hope all 160 House members would agree that the right to a choice of residential options along the entire spectrum of care should be respected and upheld.
Please continue to call or email your House member and ask them to cosponsor or sign onto Amendments 695, 699, and 703. You can find your legislator here. Thanks!
Our proposed budget amendments assert a right to placement in an ICF in line with the landmark federal Boulet case
As the Massachusetts House of Representatives gets ready to debate the Fiscal Year 2027 state budget next week, we are advocating for three budget amendments to help ensure the preservation of the Wrentham and Hogan Intermediate Care Facilities.
At our request, Representative Marcus Vaughn, whose district houses the Wrentham Center, has filed Amendment 695 to the budget legislation. This amendment states that people with intellectual and developmental disabilities (I/DD), who have been found to be eligible for ICF-level care, have a right to an ICF residential setting.
A second amendment filed by Rep. Vaughn (Amendment 699) requires DDS to report on its efforts to inform families of all residential choices available for care, including ICF care. And a third amendment (Amendment 703) states that residents of ICFs cannot be involuntarily discharged from those facilities.
Among the House members who have told us they support the proposed amendments and will co-sponsor them are Reps. Lisa Field, a member of the Mass. Nurses Association; Lindsay Sabadosa, and Joseph McKenna. We are urging our members to call or email their House member and ask them to cosponsor or sign onto Amendments 695, 699, and 703. You can find your legislator here.
DDS failing to recognize the right to ICF care
The Department of Developmental Services (DDS), which operates the Wrentham and Hogan Centers, has routinely denied requests for placements in those facilities, implying that clients of the Department do not have a right to such placements.
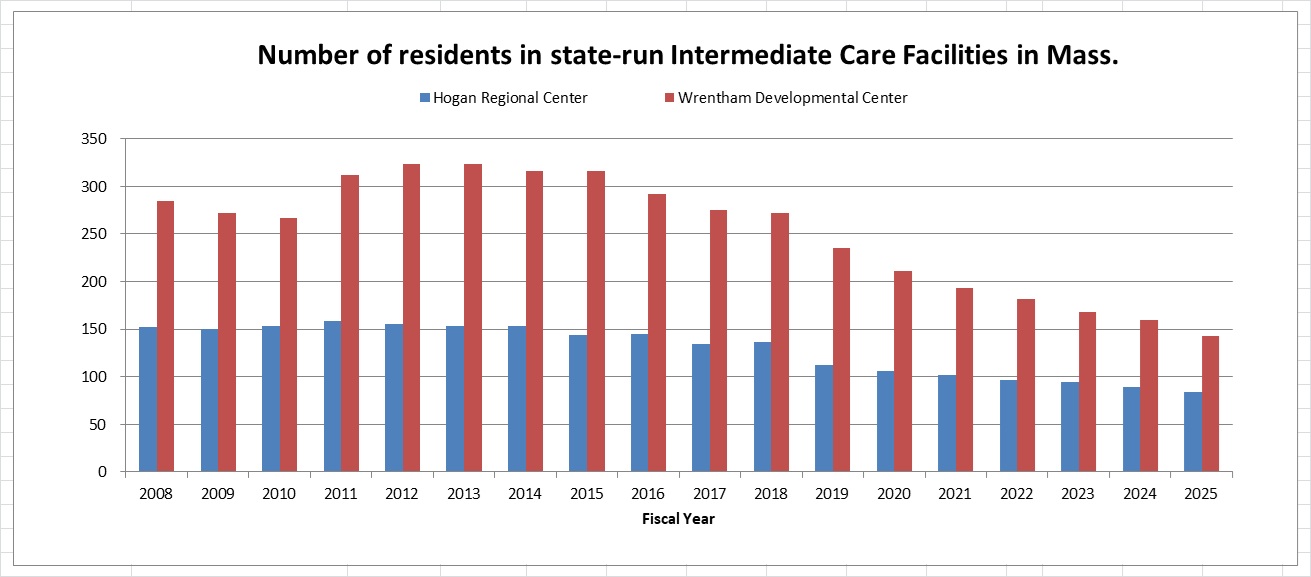
At the same time, DDS has not provided clear or acceptable criteria for admission to Wrentham or Hogan. As a result, the census in both facilities has continued to drop, and we believe the centers are on a path to closure due to attrition. (See the graph below.)
In at least two cases in recent years in which family members have filed administrative appeals to gain admission to Wrentham, a DDS hearing officer accepted the Department’s argument that the federal Medicaid law “does not entitle (the individual) admission to an Intermediate Care Facility…”
DDS’s only stated criterion for admission to Wrentham in those appeals was: “DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
Wrentham and Hogan are the only two congregate-care ICFs remaining in Massachusetts. They are state-run, federally regulated, and Medicaid-certified. They provide specialized services for people with profound disabilities, including 24/7 medical care and structured educational, vocational, and recreational programming.
The loss of these centers would mean the loss of critical care for individuals with the most profound disabilities. Given that thousands of people are reportedly waiting for residential placements in the DDS system, individuals are already facing increased hospitalizations and emergency room visits, and many families are forced to take on care beyond their capacity. The loss of Wrentham and Hogan would only worsen this situation.
Boulet case confirms a right to ICF care under federal law
In our view, eligible DDS clients do have a right to choose care in an ICF. That right is established in the federal Medicaid law and regulations, and is affirmed in the landmark Boulet v. Cellucci federal court decision (107 F. Supp. 2d 61 (D. Mass. 2000).
The Boulet decision, which was written by U.S. District Court Judge Douglas Woodlock, required DDS to provide residential services promptly to thousands of clients who had been waiting for placements, in some cases for years.
Woodlock’s decision states that there is a right to ICF care, provided with “reasonable promptness,” for those clients who are found to be eligible for that level of care and request it. The decision cites and closely tracks the federal Medicaid statute and regulatory language that we have been citing for some time.
- The Boulet decision states that if a state includes ICF services in its state plan, which Massachusetts does, the Medicaid law requires “that this type of ‘medical assistance’ be provided ‘with reasonable promptness.'” The decision then cites the Medicaid statute (42 U.S.C., § 1396a(a) (8)), and adds, “Therefore, to the extent that the plaintiffs have requested ICF/MR (now ICF/IDD) services, the state must provide those services reasonably promptly.”
- The decision also discusses the Home and Community Based Services (HCBS) waiver, and states that under the waiver, an ICF-eligible individual or his legal representative “will be: 1. informed of any feasible alternatives under the waiver; and 2. Given the choice of either institutional or home and community-based services.” The decision further cites the Medicaid regulation, 42 C.F.R. § 441.302(d), as explicitly requiring the choice of either institutional or HCBS care.
Woodlock’s decision also cites a 1998 11th Circuit U.S. Court of Appeals decision (Doe v. Chiles,136 F.3d 709 (1998) at 721) that held that states cannot justify long delays for covered services, including those provided by ICFs/IDD.
We think our proposed budget amendment is therefore consistent with the holdings of both federal law and with Boulet, both of which recognize that eligible clients must be informed of all feasible residential alternatives and given a choice among service settings, including ICF care.
We believe that asserting a right in state law to ICF care for eligible individuals will make it clear that DDS cannot deny admissions for Wrentham or Hogan without establishing clear criteria for admissions that include factors such as the degree of a person’s cognitive impairment.
That should ensure that the doors to those facilities are reopened to eligible clients who seek placements there, and thereby ensure the preservation of those critically important centers.
The Wrentham and Hogan Centers should be on the preservation list along with the Pappas Rehab Hospital
We are supporting the efforts of a number of unions and other advocates for the disabled to save the Pappas Rehabilitation Hospital from closure.
We are also pushing, at the same time, to add the state’s two remaining Intermediate Care Facilities for persons with intellectual and developmental disabilities (ICF/IDDs) — the Wrentham Developmental Center and the Hogan Regional Center — to the list of endangered facilities that must be preserved in Massachusetts.
There appear to be a number of parallels between the Healey administration’s reported policy of restricting admissions to the Pappas Hospital, and its policy of denying most requests for placement at Wrentham and Hogan.
The administration has placed “overly restrictive admissions criteria” at Pappas, according to nurses there. It is a policy that is likely to lead to Pappas’s closure.
As we have long reported, the administration is similarly allowing the Wrentham and Hogan Centers to die by attrition by denying admissions to all but a handful of applicants in recent years.
The 60-bed Pappas Rehabilitation Hospital in Canton offers medical, rehabilitative, educational and recreational services for persons with developmental disabilities up to the age of 22. In January 2025, Governor Maura Healey did announce that she planned to close the facility in order to save money and move the hospital’s programs to the state-run Western Massachusetts Hospital in Westfield.
COFAR joined state employee unions in opposing the governor’s closure of Pappas. That opposition prodded the administration to reverse its public stance. Healey is now saying she has no plans to close the facility, but the nurses there contend the governor’s statements don’t match the administration’s actual policy.
Last month, staffers at Pappas cast a vote of no confidence in Public Health Commissioner Robbie Goldstein in light of the Public Health Department’s alleged efforts to restrict admissions there, the Boston Herald reported.
Denials of admissions at both Pappas and the ICFs
The administration maintains the allegations of restricted admissions at Pappas are “inaccurate and (an) unhelpful escalation.” But the Herald reported that a mother’s request for admission to Pappas of a 12-year-old boy with severe disabilities had been denied. The boy is nonverbal, blind, and has other medical complications.
The Department of Developmental Services (DDS) has similarly routinely denied requests by family members to gain admission of their loved ones to Wrentham and Hogan. One of those cases involved Kristen Robinson, who is profoundly intellectually disabled, legally blind and quadriplegic, and has a seizure disorder and severe dysphagia, a medical condition that causes an inability to swallow.
DDS initially denied multiple requests by Kristen’s sisters, Kim Meehan and Karen Brady, to get Kristen admitted to the Wrentham Center. It was only through exhaustive efforts that included contacting the media, that Kim and Karen were able to get Kristen into Hogan, where she is now thriving. DDS has continued to deny Kim’s and Karen’s requests to place Kristen at Wrentham, which is much closer to where they live.
It also appears that the legal and internal appeals divisions at DDS have a bias against families and guardians seeking admission of their loved ones to Wrentham and Hogan. In at least two cases, a DDS hearing officer denied appeals by families to transfer intellectually disabled persons from corporate, provider-run group homes to Wrentham.
In both cases, the same DDS hearing officer denied the appeals in rulings that used much of the same language, and discounted concerns raised by the families about a lack of adequate care and meaningful activities in “community-based” group homes and day programs.
In both cases, the hearing officer stated that the individuals did not have a right under federal law to placement in an ICF. Also, in each appeal, DDS stated that it was restricting admissions to ICFs to cases “where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
COFAR is, as a result, urging state lawmakers to adopt language in the state budget, asserting the right to ICF care for all persons who have been found to be eligible for that level of care.
Rhetoric not matching policy
In the case of Pappas, the administration is insisting that there are no admissions restrictions. The Herald quoted a spokesperson for the governor last month as saying:
Pappas continues to operate as usual, with new patients being admitted and patients being appropriately discharged when they finish their treatment. In fact, the Commissioner has been actively notifying providers of space available for new patients to be admitted at Pappas, and will continue to do so.
At a recent call-in show on Boston Public Radio, Governor Healey made a similarly reassuring statement to a COFAR advocate who asked whether the governor planned to keep the Wrentham and Hogan Centers open. Healey responded, saying, “Rest assured, there are no plans to close any facilities in Massachusetts.”
But the advocate wasn’t given the opportunity on the call-in show to ask any follow-up questions, such as why DDS routinely denies admission to the Wrentham and Hogan centers, and why there has been a steadily declining number of residents, or census, in facilities as a result.
The census at Wrentham dropped from 323 in Fiscal 2012, to 143 in Fiscal 2025 – a 56% drop. The census at Hogan dropped from 155 in Fiscal 2012, to 84 in Fiscal 2025 – a 46% drop.
We are urging all of the advocates for the preservation of Pappas to join us as well in fighting to preserve Wrentham and Hogan. Email or call your House member and urge them to support the upcoming budget amendment establishing a right to care in Wrentham and Hogan. You can find your legislator here.
Saving Pappas and saving Wrentham and Hogan are all a part of the same battle. It is a battle to stop the runaway privatization of state-run care and the race to the bottom in standards that will result from the closure of those state-run facilities.
New book gives a fair-minded account of Walter Fernald, yet unfairly attacks the Fernald Developmental Center
There is a strange dichotomy in a new book by writer and anti-congregate care activist Alex Green about the professional life of Walter E. Fernald, the first superintendent of what was later to become the Fernald Developmental Center.
On the one hand, “A Perfect Turmoil: Walter E. Fernald and the Struggle to Care for America’s Disabled,” offers a largely positive and sympathetic account of Walter Fernald, who took the reins in 1887 of what was then called the Massachusetts School for the Feeble Minded.
Green portrays Fernald as a complex figure—capable of compassion, self-reflection, and change—as he engaged with the flawed scientific ideas of his time.
In contrast, the book paints the Waltham-based Fernald Center itself in a uniformly negative and what we consider to be unfair light, branding it at the outset of the book as “a nightmare” and “a place of shame.” That stark characterization is not supported by a similarly balanced examination of the history of the facility, which functioned until its closure in 2014.
There is no question that institutions like Fernald experienced serious problems, particularly in the early and mid-20th century. But the book gives virtually no attention to the landmark federal litigation in Massachusetts — Ricci v. Okin — which brought about significant improvements, starting in the 1970s, in the care and conditions at Fernald and other developmental centers in the state.
That omission is not a minor one. The Fernald Center remains a potent symbol in the ongoing debate over the future of care for people with intellectual and developmental disabilities (I/DD), including the role of the two remaining congregate care facilities in Massachusetts — the Wrentham Developmental Center and the Hogan Regional Center. By focusing almost exclusively on the Fernald Center’s darkest chapters, the book reinforces a one-sided narrative that continues to shape policy discussions today.
Green has long promoted uniformly negative views about Fernald, the institution. For a number of years, he organized protests and petitions related to the Fernald site, and wrote a commentary in November 2020 that advocated for deinstitutionalization. He was also instrumental in the creation of a state commission in Massachusetts, which made several uniformly negative statements about institutional care in its final report.
Green’s advocacy on these issues is also relevant in light of the book’s selection last month as the winner of the National Book Critics Circle Award in the biography category.
Book lauds Walter Fernald, but disparages the Fernald Center
Here is Green’s description of Walter Fernald, the man, in the introduction to his book:
When (Walter) Fernald died (in 1924)…(h)e was remembered for his compassion and kindness; for having seen a group of people who were otherwise unseen, as individual human beings deserving of our attention, love, and fellowship.
Green also states, later in the book, that:
No figure in American history did more to develop a link between the expert professions that continue to work with the cognitively and developmentally disabled today… Because of his influence on the world around him, (Walter) Fernald’s story is of immense historical significance, but its greatest importance lies in his capacity for self-reflection, self-criticism, and change.
Green does criticize Walter Fernald for his view that intellectual disabilities are inherited, and for being “a master propagandist (and) a moralist prude.” But that criticism pales in comparison to the assessments he makes about Fernald, the institution.
Here is the opening paragraph of the introduction to Green’s book:
The Walter E. Fernald State School is the most important historic site of its kind in the United States. The nation’s foremost institution for intellectually and developmentally disabled people, the school had a life span that stretched across an expanse of time from before the Civil War into the early twenty-first century. But for those who know its name, it does not stir thoughts of dates, places, or events. It is a threat, a nightmare, a deep-seated fear. It is a feeling. A place of shame. Its name is a provocation. It should be.
Here is the first sentence of the second paragraph of the introduction:
Sprawling across 196 acres near Boston, the Fernald School is synonymous with the scandal of human experimentation in the 1950s, of gut-wrenching exposes of abuse and neglect, of the futility of institutionalization and society’s widespread failure to confront that fact.
When it comes to Walter Fernald, Green can clearly be quite complimentary. But when it comes to the facility that Walter Fernald ran, he is relentlessly negative. The question is why. Why not treat Fernald, the institution, with the same open-mindedness and fairness that he treats Walter Fernald?
Fernald, the facility, lasted 90 years after Walter Fernald’s death. It was closed over the objections of the families of its 14 then remaining residents, who filed administrative and court appeals to keep it open. The appeals were ultimately unsuccessful.
Why leave out the positive aspects of Fernald’s history after the 1980s, long after Walter Fernald’s death?
The late U.S. District Court Judge Joseph Tauro noted in his 1993 disengagement order from the Ricci V. Okin case that both the major capital and staffing improvements to the facilities and a program of community placements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
Green doesn’t mention that. In fact, he dispenses with Tauro and the Ricci case with one sentence, simply saying that:
In Massachusetts, a series of suits on behalf of inmates, first launched by University of Massachusetts Professor Ben Ricci at the Belchertown State School, were consolidated by Judge Joseph Tauro in federal court, and when Michael Dukakis became governor in 1975, he committed to settling the combined suit by pumping significant sums of money into institutional reform.
Green does not acknowledge Tauro’s conclusion that the reform resulted in a world-class system of both institutional and community-based care. To do so would contradict the narrative that the Fernald Center was never anything other than a nightmare and a place of shame.
Governor asked about Wrentham and Hogan
At a March 27 appearance on Boston Public Radio’s Ask the Governor segment, co-host Jim Braude lauded Green’s book as Governor Maura Healey stood by. Later in the show, Healey took a question from Elaine Strug, a COFAR member and a member of our partner organization, The Saving Wrentham and Hogan Alliance.
Elaine asked whether Healey planned to keep the Wrentham and Hogan Centers open, noting that her son would benefit from the 24/7 specialized medical and clinical care available in either of those facilities. Elaine pointed out that Hogan and Wrentham, which are now known as Intermediate Care Facilities (ICFs), are federally regulated and Medicaid certified.
Healey responded to Elaine, saying, “Rest assured, there are no plans to close any facilities in Massachusetts.” But Elaine was not able to ask a follow-up question as to why individuals like her son are generally denied admission to the centers, and why the administration appears to be letting the centers die by attrition.
Little actual discussion of the Fernald Center
It is also somewhat strange that while Green’s book condemns the Fernald Center, it devotes relatively few of its 368 pages to actually discussing the Center’s sins and shortcomings.
The book instead dwells at length on Walter Fernald’s complex relationship with the eugenics movement in the U.S. and around the world in the early 20th century. Green also extensively discusses Fernald’s shifting views on the nascent intelligence testing movement during that same period. He notes that while Fernald understood the necessity of such testing, he questioned the methodology that was being developed at the time and whether it was accurate in measuring the capacity of persons with I/DD.
Green further discusses Fernald’s skepticism of the push in the early 20th century, in line with the eugenics movement, to sterilize people with I/DD. He quotes Fernald as saying that intellectual disability, which was then called feeble-mindedness “is infinitely a more complicated problem than the believers in the potency of sterilization would have us believe.”
Green’s discussion of those topics is the strongest and most interesting part of his book. There is actually remarkably little discussion in the book of conditions in the Fernald institution itself, even prior to the 1980s.
Green does acknowledge that by the time Fernald closed in 2014, the community-system itself wasn’t living up to the promise that had been envisioned for it. He states that, “group homes became isolating and isolated mini-institutions in and of themselves.”
Green also recognizes that by 2014, the parents of the remaining residents were resisting Fernald’s closure, noting that, “They had fought for improvements to the institution and were getting them. Why should they send people into a world (community system) of cruelty and abuse?”
But then Green dismisses the parents’ concerns:
They were unwittingly in the same position as Walter Fernald in the 1890s, making the argument that had failed him because it deprived disabled people of their fundamental rights as a result of something they were not responsible for – the cruelty of the nondisabled.
Green’s is the standard argument in favor of community-based care: Even if the community system is an isolating system consisting of isolated mini-institutions, disabled people have a right to be subjected to those conditions. Even their families need to understand that this is what is best for them.
And Green flatly states that “the institutions were capable of only so much reform. Rampant abuse was impossible to stamp out,” although he acknowledges abuse is “as likely to occur inside or outside of an institution.” So, why does he condemn only institutional care at the outset of the book?
A book that gets institutional care right
The best history of institutional care I’ve read is Ingrid Grenon’s book, “From One Century to the Next: A history of Wrentham State School and the Institutional Model in Massachusetts.”
As I noted in my review of Grenon’s book, her account of the Wrentham Center makes a powerful case that institutions, in themselves, are neither good nor bad. It is how they are run that counts, just as is the case in any care setting. Grenon recounts that the 1920s was a period when the then Wrentham State School, under the direction of its first superintendent, George Wallace, had a caring staff and administration, and offered a multitude of services and activities for the residents.
As Grenon points out, the Wrentham Center, like Fernald and other similar institutions that sprang up in this state and around the country, entered a long decline, starting in the 1930s as they became more and more overcrowded and understaffed. The state schools in Massachusetts were finally brought back to excellence as a result of the Ricci v. Okin class action litigation.
Unlike Green, Grenon, in our view, draws the correct lesson from history of the role of institutional care in Massachusetts and elsewhere around the country.
