Archive
Our proposed budget amendments assert a right to placement in an ICF in line with the landmark federal Boulet case
As the Massachusetts House of Representatives gets ready to debate the Fiscal Year 2027 state budget next week, we are advocating for three budget amendments to help ensure the preservation of the Wrentham and Hogan Intermediate Care Facilities.
At our request, Representative Marcus Vaughn, whose district houses the Wrentham Center, has filed Amendment 695 to the budget legislation. This amendment states that people with intellectual and developmental disabilities (I/DD), who have been found to be eligible for ICF-level care, have a right to an ICF residential setting.
A second amendment filed by Rep. Vaughn (Amendment 699) requires DDS to report on its efforts to inform families of all residential choices available for care, including ICF care. And a third amendment (Amendment 703) states that residents of ICFs cannot be involuntarily discharged from those facilities.
Among the House members who have told us they support the proposed amendments and will co-sponsor them are Reps. Lisa Field, a member of the Mass. Nurses Association; Lindsay Sabadosa, and Joseph McKenna. We are urging our members to call or email their House member and ask them to cosponsor or sign onto Amendments 695, 699, and 703. You can find your legislator here.
DDS failing to recognize the right to ICF care
The Department of Developmental Services (DDS), which operates the Wrentham and Hogan Centers, has routinely denied requests for placements in those facilities, implying that clients of the Department do not have a right to such placements.
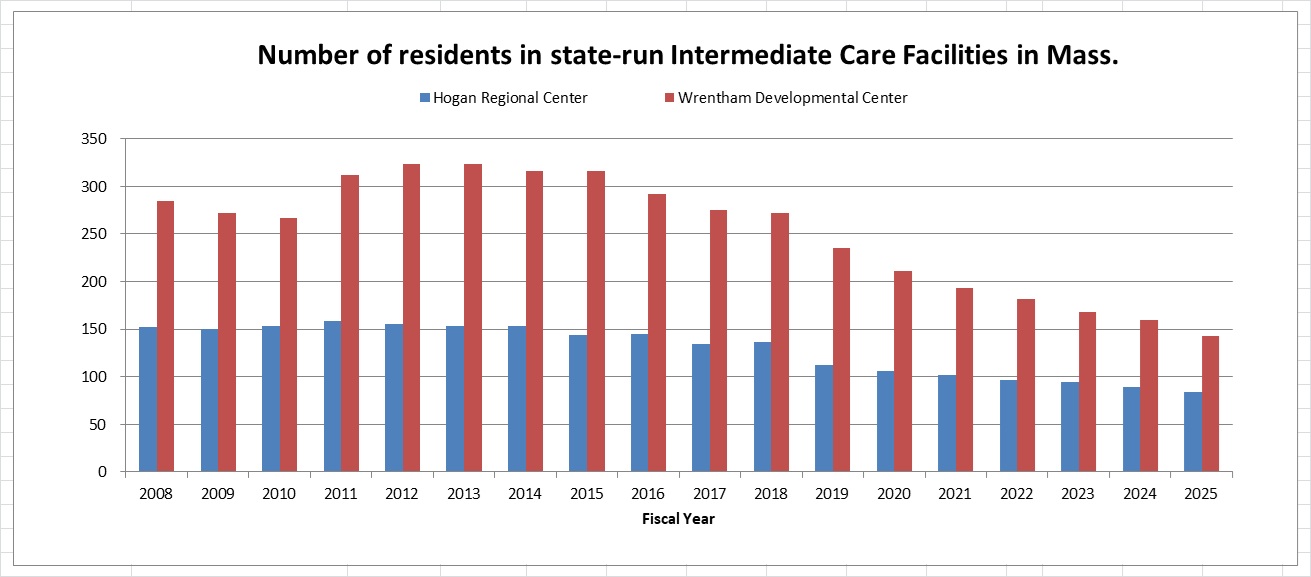
At the same time, DDS has not provided clear or acceptable criteria for admission to Wrentham or Hogan. As a result, the census in both facilities has continued to drop, and we believe the centers are on a path to closure due to attrition. (See the graph below.)
In at least two cases in recent years in which family members have filed administrative appeals to gain admission to Wrentham, a DDS hearing officer accepted the Department’s argument that the federal Medicaid law “does not entitle (the individual) admission to an Intermediate Care Facility…”
DDS’s only stated criterion for admission to Wrentham in those appeals was: “DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
Wrentham and Hogan are the only two congregate-care ICFs remaining in Massachusetts. They are state-run, federally regulated, and Medicaid-certified. They provide specialized services for people with profound disabilities, including 24/7 medical care and structured educational, vocational, and recreational programming.
The loss of these centers would mean the loss of critical care for individuals with the most profound disabilities. Given that thousands of people are reportedly waiting for residential placements in the DDS system, individuals are already facing increased hospitalizations and emergency room visits, and many families are forced to take on care beyond their capacity. The loss of Wrentham and Hogan would only worsen this situation.
Boulet case confirms a right to ICF care under federal law
In our view, eligible DDS clients do have a right to choose care in an ICF. That right is established in the federal Medicaid law and regulations, and is affirmed in the landmark Boulet v. Cellucci federal court decision (107 F. Supp. 2d 61 (D. Mass. 2000).
The Boulet decision, which was written by U.S. District Court Judge Douglas Woodlock, required DDS to provide residential services promptly to thousands of clients who had been waiting for placements, in some cases for years.
Woodlock’s decision states that there is a right to ICF care, provided with “reasonable promptness,” for those clients who are found to be eligible for that level of care and request it. The decision cites and closely tracks the federal Medicaid statute and regulatory language that we have been citing for some time.
- The Boulet decision states that if a state includes ICF services in its state plan, which Massachusetts does, the Medicaid law requires “that this type of ‘medical assistance’ be provided ‘with reasonable promptness.'” The decision then cites the Medicaid statute (42 U.S.C., § 1396a(a) (8)), and adds, “Therefore, to the extent that the plaintiffs have requested ICF/MR (now ICF/IDD) services, the state must provide those services reasonably promptly.”
- The decision also discusses the Home and Community Based Services (HCBS) waiver, and states that under the waiver, an ICF-eligible individual or his legal representative “will be: 1. informed of any feasible alternatives under the waiver; and 2. Given the choice of either institutional or home and community-based services.” The decision further cites the Medicaid regulation, 42 C.F.R. § 441.302(d), as explicitly requiring the choice of either institutional or HCBS care.
Woodlock’s decision also cites a 1998 11th Circuit U.S. Court of Appeals decision (Doe v. Chiles,136 F.3d 709 (1998) at 721) that held that states cannot justify long delays for covered services, including those provided by ICFs/IDD.
We think our proposed budget amendment is therefore consistent with the holdings of both federal law and with Boulet, both of which recognize that eligible clients must be informed of all feasible residential alternatives and given a choice among service settings, including ICF care.
We believe that asserting a right in state law to ICF care for eligible individuals will make it clear that DDS cannot deny admissions for Wrentham or Hogan without establishing clear criteria for admissions that include factors such as the degree of a person’s cognitive impairment.
That should ensure that the doors to those facilities are reopened to eligible clients who seek placements there, and thereby ensure the preservation of those critically important centers.
The Wrentham and Hogan Centers should be on the preservation list along with the Pappas Rehab Hospital
We are supporting the efforts of a number of unions and other advocates for the disabled to save the Pappas Rehabilitation Hospital from closure.
We are also pushing, at the same time, to add the state’s two remaining Intermediate Care Facilities for persons with intellectual and developmental disabilities (ICF/IDDs) — the Wrentham Developmental Center and the Hogan Regional Center — to the list of endangered facilities that must be preserved in Massachusetts.
There appear to be a number of parallels between the Healey administration’s reported policy of restricting admissions to the Pappas Hospital, and its policy of denying most requests for placement at Wrentham and Hogan.
The administration has placed “overly restrictive admissions criteria” at Pappas, according to nurses there. It is a policy that is likely to lead to Pappas’s closure.
As we have long reported, the administration is similarly allowing the Wrentham and Hogan Centers to die by attrition by denying admissions to all but a handful of applicants in recent years.
The 60-bed Pappas Rehabilitation Hospital in Canton offers medical, rehabilitative, educational and recreational services for persons with developmental disabilities up to the age of 22. In January 2025, Governor Maura Healey did announce that she planned to close the facility in order to save money and move the hospital’s programs to the state-run Western Massachusetts Hospital in Westfield.
COFAR joined state employee unions in opposing the governor’s closure of Pappas. That opposition prodded the administration to reverse its public stance. Healey is now saying she has no plans to close the facility, but the nurses there contend the governor’s statements don’t match the administration’s actual policy.
Last month, staffers at Pappas cast a vote of no confidence in Public Health Commissioner Robbie Goldstein in light of the Public Health Department’s alleged efforts to restrict admissions there, the Boston Herald reported.
Denials of admissions at both Pappas and the ICFs
The administration maintains the allegations of restricted admissions at Pappas are “inaccurate and (an) unhelpful escalation.” But the Herald reported that a mother’s request for admission to Pappas of a 12-year-old boy with severe disabilities had been denied. The boy is nonverbal, blind, and has other medical complications.
The Department of Developmental Services (DDS) has similarly routinely denied requests by family members to gain admission of their loved ones to Wrentham and Hogan. One of those cases involved Kristen Robinson, who is profoundly intellectually disabled, legally blind and quadriplegic, and has a seizure disorder and severe dysphagia, a medical condition that causes an inability to swallow.
DDS initially denied multiple requests by Kristen’s sisters, Kim Meehan and Karen Brady, to get Kristen admitted to the Wrentham Center. It was only through exhaustive efforts that included contacting the media, that Kim and Karen were able to get Kristen into Hogan, where she is now thriving. DDS has continued to deny Kim’s and Karen’s requests to place Kristen at Wrentham, which is much closer to where they live.
It also appears that the legal and internal appeals divisions at DDS have a bias against families and guardians seeking admission of their loved ones to Wrentham and Hogan. In at least two cases, a DDS hearing officer denied appeals by families to transfer intellectually disabled persons from corporate, provider-run group homes to Wrentham.
In both cases, the same DDS hearing officer denied the appeals in rulings that used much of the same language, and discounted concerns raised by the families about a lack of adequate care and meaningful activities in “community-based” group homes and day programs.
In both cases, the hearing officer stated that the individuals did not have a right under federal law to placement in an ICF. Also, in each appeal, DDS stated that it was restricting admissions to ICFs to cases “where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
COFAR is, as a result, urging state lawmakers to adopt language in the state budget, asserting the right to ICF care for all persons who have been found to be eligible for that level of care.
Rhetoric not matching policy
In the case of Pappas, the administration is insisting that there are no admissions restrictions. The Herald quoted a spokesperson for the governor last month as saying:
Pappas continues to operate as usual, with new patients being admitted and patients being appropriately discharged when they finish their treatment. In fact, the Commissioner has been actively notifying providers of space available for new patients to be admitted at Pappas, and will continue to do so.
At a recent call-in show on Boston Public Radio, Governor Healey made a similarly reassuring statement to a COFAR advocate who asked whether the governor planned to keep the Wrentham and Hogan Centers open. Healey responded, saying, “Rest assured, there are no plans to close any facilities in Massachusetts.”
But the advocate wasn’t given the opportunity on the call-in show to ask any follow-up questions, such as why DDS routinely denies admission to the Wrentham and Hogan centers, and why there has been a steadily declining number of residents, or census, in facilities as a result.
The census at Wrentham dropped from 323 in Fiscal 2012, to 143 in Fiscal 2025 – a 56% drop. The census at Hogan dropped from 155 in Fiscal 2012, to 84 in Fiscal 2025 – a 46% drop.
We are urging all of the advocates for the preservation of Pappas to join us as well in fighting to preserve Wrentham and Hogan. Email or call your House member and urge them to support the upcoming budget amendment establishing a right to care in Wrentham and Hogan. You can find your legislator here.
Saving Pappas and saving Wrentham and Hogan are all a part of the same battle. It is a battle to stop the runaway privatization of state-run care and the race to the bottom in standards that will result from the closure of those state-run facilities.
New book gives a fair-minded account of Walter Fernald, yet unfairly attacks the Fernald Developmental Center
There is a strange dichotomy in a new book by writer and anti-congregate care activist Alex Green about the professional life of Walter E. Fernald, the first superintendent of what was later to become the Fernald Developmental Center.
On the one hand, “A Perfect Turmoil: Walter E. Fernald and the Struggle to Care for America’s Disabled,” offers a largely positive and sympathetic account of Walter Fernald, who took the reins in 1887 of what was then called the Massachusetts School for the Feeble Minded.
Green portrays Fernald as a complex figure—capable of compassion, self-reflection, and change—as he engaged with the flawed scientific ideas of his time.
In contrast, the book paints the Waltham-based Fernald Center itself in a uniformly negative and what we consider to be unfair light, branding it at the outset of the book as “a nightmare” and “a place of shame.” That stark characterization is not supported by a similarly balanced examination of the history of the facility, which functioned until its closure in 2014.
There is no question that institutions like Fernald experienced serious problems, particularly in the early and mid-20th century. But the book gives virtually no attention to the landmark federal litigation in Massachusetts — Ricci v. Okin — which brought about significant improvements, starting in the 1970s, in the care and conditions at Fernald and other developmental centers in the state.
That omission is not a minor one. The Fernald Center remains a potent symbol in the ongoing debate over the future of care for people with intellectual and developmental disabilities (I/DD), including the role of the two remaining congregate care facilities in Massachusetts — the Wrentham Developmental Center and the Hogan Regional Center. By focusing almost exclusively on the Fernald Center’s darkest chapters, the book reinforces a one-sided narrative that continues to shape policy discussions today.
Green has long promoted uniformly negative views about Fernald, the institution. For a number of years, he organized protests and petitions related to the Fernald site, and wrote a commentary in November 2020 that advocated for deinstitutionalization. He was also instrumental in the creation of a state commission in Massachusetts, which made several uniformly negative statements about institutional care in its final report.
Green’s advocacy on these issues is also relevant in light of the book’s selection last month as the winner of the National Book Critics Circle Award in the biography category.
Book lauds Walter Fernald, but disparages the Fernald Center
Here is Green’s description of Walter Fernald, the man, in the introduction to his book:
When (Walter) Fernald died (in 1924)…(h)e was remembered for his compassion and kindness; for having seen a group of people who were otherwise unseen, as individual human beings deserving of our attention, love, and fellowship.
Green also states, later in the book, that:
No figure in American history did more to develop a link between the expert professions that continue to work with the cognitively and developmentally disabled today… Because of his influence on the world around him, (Walter) Fernald’s story is of immense historical significance, but its greatest importance lies in his capacity for self-reflection, self-criticism, and change.
Green does criticize Walter Fernald for his view that intellectual disabilities are inherited, and for being “a master propagandist (and) a moralist prude.” But that criticism pales in comparison to the assessments he makes about Fernald, the institution.
Here is the opening paragraph of the introduction to Green’s book:
The Walter E. Fernald State School is the most important historic site of its kind in the United States. The nation’s foremost institution for intellectually and developmentally disabled people, the school had a life span that stretched across an expanse of time from before the Civil War into the early twenty-first century. But for those who know its name, it does not stir thoughts of dates, places, or events. It is a threat, a nightmare, a deep-seated fear. It is a feeling. A place of shame. Its name is a provocation. It should be.
Here is the first sentence of the second paragraph of the introduction:
Sprawling across 196 acres near Boston, the Fernald School is synonymous with the scandal of human experimentation in the 1950s, of gut-wrenching exposes of abuse and neglect, of the futility of institutionalization and society’s widespread failure to confront that fact.
When it comes to Walter Fernald, Green can clearly be quite complimentary. But when it comes to the facility that Walter Fernald ran, he is relentlessly negative. The question is why. Why not treat Fernald, the institution, with the same open-mindedness and fairness that he treats Walter Fernald?
Fernald, the facility, lasted 90 years after Walter Fernald’s death. It was closed over the objections of the families of its 14 then remaining residents, who filed administrative and court appeals to keep it open. The appeals were ultimately unsuccessful.
Why leave out the positive aspects of Fernald’s history after the 1980s, long after Walter Fernald’s death?
The late U.S. District Court Judge Joseph Tauro noted in his 1993 disengagement order from the Ricci V. Okin case that both the major capital and staffing improvements to the facilities and a program of community placements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
Green doesn’t mention that. In fact, he dispenses with Tauro and the Ricci case with one sentence, simply saying that:
In Massachusetts, a series of suits on behalf of inmates, first launched by University of Massachusetts Professor Ben Ricci at the Belchertown State School, were consolidated by Judge Joseph Tauro in federal court, and when Michael Dukakis became governor in 1975, he committed to settling the combined suit by pumping significant sums of money into institutional reform.
Green does not acknowledge Tauro’s conclusion that the reform resulted in a world-class system of both institutional and community-based care. To do so would contradict the narrative that the Fernald Center was never anything other than a nightmare and a place of shame.
Governor asked about Wrentham and Hogan
At a March 27 appearance on Boston Public Radio’s Ask the Governor segment, co-host Jim Braude lauded Green’s book as Governor Maura Healey stood by. Later in the show, Healey took a question from Elaine Strug, a COFAR member and a member of our partner organization, The Saving Wrentham and Hogan Alliance.
Elaine asked whether Healey planned to keep the Wrentham and Hogan Centers open, noting that her son would benefit from the 24/7 specialized medical and clinical care available in either of those facilities. Elaine pointed out that Hogan and Wrentham, which are now known as Intermediate Care Facilities (ICFs), are federally regulated and Medicaid certified.
Healey responded to Elaine, saying, “Rest assured, there are no plans to close any facilities in Massachusetts.” But Elaine was not able to ask a follow-up question as to why individuals like her son are generally denied admission to the centers, and why the administration appears to be letting the centers die by attrition.
Little actual discussion of the Fernald Center
It is also somewhat strange that while Green’s book condemns the Fernald Center, it devotes relatively few of its 368 pages to actually discussing the Center’s sins and shortcomings.
The book instead dwells at length on Walter Fernald’s complex relationship with the eugenics movement in the U.S. and around the world in the early 20th century. Green also extensively discusses Fernald’s shifting views on the nascent intelligence testing movement during that same period. He notes that while Fernald understood the necessity of such testing, he questioned the methodology that was being developed at the time and whether it was accurate in measuring the capacity of persons with I/DD.
Green further discusses Fernald’s skepticism of the push in the early 20th century, in line with the eugenics movement, to sterilize people with I/DD. He quotes Fernald as saying that intellectual disability, which was then called feeble-mindedness “is infinitely a more complicated problem than the believers in the potency of sterilization would have us believe.”
Green’s discussion of those topics is the strongest and most interesting part of his book. There is actually remarkably little discussion in the book of conditions in the Fernald institution itself, even prior to the 1980s.
Green does acknowledge that by the time Fernald closed in 2014, the community-system itself wasn’t living up to the promise that had been envisioned for it. He states that, “group homes became isolating and isolated mini-institutions in and of themselves.”
Green also recognizes that by 2014, the parents of the remaining residents were resisting Fernald’s closure, noting that, “They had fought for improvements to the institution and were getting them. Why should they send people into a world (community system) of cruelty and abuse?”
But then Green dismisses the parents’ concerns:
They were unwittingly in the same position as Walter Fernald in the 1890s, making the argument that had failed him because it deprived disabled people of their fundamental rights as a result of something they were not responsible for – the cruelty of the nondisabled.
Green’s is the standard argument in favor of community-based care: Even if the community system is an isolating system consisting of isolated mini-institutions, disabled people have a right to be subjected to those conditions. Even their families need to understand that this is what is best for them.
And Green flatly states that “the institutions were capable of only so much reform. Rampant abuse was impossible to stamp out,” although he acknowledges abuse is “as likely to occur inside or outside of an institution.” So, why does he condemn only institutional care at the outset of the book?
A book that gets institutional care right
The best history of institutional care I’ve read is Ingrid Grenon’s book, “From One Century to the Next: A history of Wrentham State School and the Institutional Model in Massachusetts.”
As I noted in my review of Grenon’s book, her account of the Wrentham Center makes a powerful case that institutions, in themselves, are neither good nor bad. It is how they are run that counts, just as is the case in any care setting. Grenon recounts that the 1920s was a period when the then Wrentham State School, under the direction of its first superintendent, George Wallace, had a caring staff and administration, and offered a multitude of services and activities for the residents.
As Grenon points out, the Wrentham Center, like Fernald and other similar institutions that sprang up in this state and around the country, entered a long decline, starting in the 1930s as they became more and more overcrowded and understaffed. The state schools in Massachusetts were finally brought back to excellence as a result of the Ricci v. Okin class action litigation.
Unlike Green, Grenon, in our view, draws the correct lesson from history of the role of institutional care in Massachusetts and elsewhere around the country.
State Commission vilifies institutions for people with developmental disabilities and demands an apology from the governor
A state commission established in 2023 to study the history of institutions for the developmentally disabled and mentally ill in Massachusetts has issued a final report which, as expected, almost completely vilifies those facilities.
The report by the Massachusetts Special Commission on State Institutions, which is dated May 25, paints an overwhelmingly negative and untrue picture of the history of the institutions, often couched in extreme terms. The report only briefly mentions the dramatic improvements in those centers for the developmentally disabled that occurred starting in the 1970s.
We repeatedly predicted that the Commission would examine only the history of the institutions prior to the 1980s when those facilities were notorious for abuse, neglect and poor conditions.
Our concern has been, and now remains, that opponents of the Wrentham and Hogan Intermediate Care Facilities (ICFs), the state’s two remaining congregate care centers for people with developmental disabilities, will use the report as justification for pushing for the closure of the facilities.
Notably, the report demands a formal apology from the governor, who, it claims, “must acknowledge the enormity of the legacy and harm of mass institutionalization that reverberates today.”
But what about the improvements that were made in institutional care starting in the 1970s in Massachusetts under the landmark Ricci v. Okin class action lawsuit? The late U.S. District Court Judge Joseph L. Tauro, who oversaw the consent decree in that case, said in 1993 that the care in the institutions was by then “second to none anywhere in the world.”
Isn’t that improvement also part of the legacy of institutionalization in Massachusetts? Should Governor Healey apologize for that?
What about the high federal standards that Wrentham and Hogan meet today? And what about the families that are fighting to keep Wrentham and Hogan open as the state pursues a policy of letting Wrentham and Hogan die by attrition?
Also, what about the legacy of deinstitutionalization, which the report does not criticize, but which has also caused much harm?
While the report has tried to make a positive contribution in calling for making public the historical records of the care of residents of institutions in Massachusetts, the report appears to assume that those records contain only damning accounts of that care. That is, of course, not true; but, the report implies that the purpose of providing public access to the records is to reveal “atrocities” committed in the institutions. As the report states:
By hiding a story of mass human rights abuses, the Commonwealth is preventing society from engaging in a full reckoning with the atrocities that have been inflicted on disabled people throughout our history.
Sensational claims concerning closed facilities
The report also makes a number of sensational claims that lack evidence of what it alleges are shocking activities that have taken place on the campuses of closed facilities. Among those allegations, for which the report doesn’t provide any details, are that some unidentified campuses have been used for pornographic photo shoots and “white supremacist celebrations.”
As the report puts it:
At their most offensive, (former institutional) sites have been used for pornographic photo shoots, white supremacist celebrations, community festivals, and amusement parks that would never be tolerated at similar sites of significant human rights abuses in Massachusetts or America.
I have not been able to find any references on line to pornographic photo shoots on the campuses of closed institutions. As noted, the Commission report provided no examples of it.
Brandeis University’s student newspaper, The Justice, reported that graffiti featuring markings of Neo-Nazi groups has been discovered on the walls of one of the buildings on the campus of the former Fernald Developmental Center. But the Waltham Police Department stated that “there are no known organized hate groups operating in the area.”
So, while vandalism at the former Fernald Center has been an ongoing issue, there is no information I could find that refers to white supremacist celebrations being held there. The Commission also provided no examples of amusement parks on the campuses of former institutions.
The amusement park reference might be to the development by the City of Waltham of a portion of the Fernald campus as a memorial park and “universally accessible” playground, with an electric train, a mini golf course, and a spray park “that would make it the largest disability-accessible park in New England.” The park received two awards from the Massachusetts Recreation and Parks Association in February for its design and commercial partnership.
In addition, the Commission report includes what appears to be a false claim that there is a threat of a “revival of large-scale institutionalizations” in Massachusetts. It provides no evidence for the claim.
While the report doesn’t appear to specifically recommend the closure Wrentham or Hogan, it claims institutionalization “stubbornly remains.” The statement appears to be an indirect call for the closure of facilities such as Wrentham and Hogan. If the report is referring only to institutions for the mentally ill as stubbornly remaining, it doesn’t specify that distinction.
The report’s full statement on this issue is:
Precisely because the public is largely unaware of the countless tragedies inflicted by these institutions—tragedies told in this hidden history—people with disabilities today face very-real threats by the non-disabled including the revival of large-scale institutionalizations where the practice has been abolished, and its expansion where it stubbornly remains.
Rights abuses were not ‘overlooked’
In its coverage of the Commission’s report, GBH News, a Boston-based National Public Radio affiliate and one of the more fervent critics of the former Fernald Center, quoted Alex Green, vice-chair of the Commission and one of the chief proponents of the Commission’s creation. According to GBH News, Green stated:
I think that there’s a massive ongoing act of erasure happening about one of the most significant and overlooked human rights tragedies in the history of this state and the country. It [the report] really gives us a devastatingly personal sense of how the state turned the idea of care into a much darker thing that harmed a lot of people.”
But the Ricci class action case and Judge Tauro’s involvement clearly show that those human rights abuses were not overlooked. They were addressed and corrected.
Moreover, even with regard to the early history of institutional care in Massachusetts, the Commission’s report appears to be uniformly negative when, in reality, not everything was necessarily bad about those early years.
As Ingrid Grenon noted in her book, “From One Century to the Next: A history of Wrentham State School and the Institutional Model in Massachusetts,” the 1920s was a period when the then Wrentham State School, under the direction of its first superintendent, George Wallace, had a caring staff and administration, and offered a multitude of services and activities for the residents.
Grenon’s book points out that Wrentham, like other similar institutions that sprang up in this state and around the country, entered a long decline, starting in the 1930s as it became more and more overcrowded and understaffed. The state schools in Massachusetts were finally brought back to excellence as a result of the Ricci v. Okin class action litigation.
But the Special Commission has this to say about those early years of institutional care in Massachusetts:
…Massachusetts developed, sustained, and exported many of the first legal, medical, educational, charitable, and social systems for placing people with intellectual, developmental, and mental health disabilities in institutions: practices widely understood for more than 75 years to be a violation of fundamental human rights. (my emphasis)
In sum, we would again emphasize that the report appears to have made some positive contributions with regard to the need for public access to records and for the identification of unmarked graves on the sites of the former institutions in Massachusetts.
But it is unfortunate that the report repeatedly leaps from those issues to unwarranted condemnations of the role and history of institutional care in the state. It’s clear from the report that the Commission did not closely examine the full history.
As we’ve previously noted, Green and other proponents of the Commission made statements prior to serving on the Commission that were almost uniformly negative about care at the former Fernald Center, in particular.
That negative agenda appears to have muddied the positive contribution that the report has tried to make with regard to the role of institutional care in Massachusetts.
An overlooked but vitally important book on the history of institutional care in Massachusetts
Among the books that anyone interested in the continuum of care for persons with intellectual and developmental disabilities (I/DD) should not miss is Ingrid Grenon’s meticulously researched “From One Century to the Next: A history of Wrentham State School and the Institutional Model in Massachusetts.”
I hope the controversial Special Commission on State Institutions, which is due to release a report on the history of institutional care in Massachusetts next June, has a copy of this book. While the book can be purchased online, it is also available in libraries.
I have to confess to having missed this book, which was published in 2015, until Grenon contacted me a few weeks ago. Having now read it, I realize it makes a powerful case that institutions, in themselves, are neither good nor bad. It is how they are run that counts, just as is the case in any care setting.

As this book documents, the high point of the care and services at Wrentham — prior to the advent of the modern Intermediate Care Facility (ICF) model in the 1980s — was during the 1920s.
The 1920s, exactly a century ago, was a period when the then Wrentham State School, under the direction of its first superintendent, George Wallace, had a caring staff and administration, and offered a multitude of services and activities for the residents. Wallace displayed a genuine interest in helping them lead meaningful and productive lives.
But, as the book shows, Wrentham, like other similar institutions that sprang up in this state and around the country, entered a long decline, starting in the 1930s as it became more and more overcrowded and understaffed. By 1960, Wrentham, which was intended to house no more than 1,500 residents, had a residential population of 2,400. Today, less than 160 residents remain there.
Wrentham and other state schools in Massachusetts were finally brought back to excellence as a result of the Ricci v. Okin class action litigation in the 1970s and the intervention of the late U.S. District Court Judge Joseph L. Tauro.
A refutation of the ideology behind deinstitutionalization
Based on that historical arc, I think the book offers a compelling refutation of the longstanding and dominant ideology used to support deinstitutionalization. That ideology is based on the premise that all institutional care is bad and outdated, and that that characteristic never changes and can never change.
The book, however, shows, on a year-by-year basis, how one institution – Wrentham — progressed from very good to very bad, and back again. Wrentham did change, and it changed dramatically. It is clear that if an institution is well run and has sufficient resources, it can be a positive and even necessary option for residential care.
Grenon’s book also shows how the ongoing debate over institutional versus community-based care was central to the thinking even of Walter Fernald and Wallace way back in the late 19th and early 20th centuries.
What was later to become the Fernald Developmental Center was established in 1848 as the first institution in the United States for persons with intellectual and developmental disabilities. It was later named for Walter Fernald, who became its first superintendent. The then Wrentham State School was officially opened in 1910.
Grenon’s book demonstrates that it’s not a simple proposition that the Fernald and Wrentham schools were meant to be segregated facilities, intended to keep people with intellectual disabilities out of the view of the general public. Even for Walter Fernald and George Wallace, there were two ways of looking at their facilities.
The centers could be seen from the perspective of the now discredited science of eugenics, as places to separate people with I//DD from the general population. Or they could be seen, as Wallace viewed them and Fernald later came to view them, as places where people with I/DD could be helped to lead meaningful and fulfilling lives. Unfortunately, the prevailing view today is that that former perspective regarding institutions is the only valid one.
Bellotti and Dukakis changed the game
Grenon documents Wrentham’s history virtually year by year from the early 1900s until 1993 when Judge Tauro officially disengaged from the Ricci litigation. It includes many photos from throughout that period.
In addition to consulting numerous primary sources, Grenon interviewed many key figures in the history of Wrentham and of institutional care in Massachusetts. Among those were former Governor Michael Dukakis and his then Attorney General Francis Bellotti.
Bellotti, who died yesterday (December 17) at the age of 101, took the unusual and courageous step in response to the Ricci lawsuit of refusing to defend the conditions at Wrentham, Fernald, Belchertown and the other state schools in the 1970s.
As Grenon explains, Bellotti’s refusal as attorney general to defend the administration – a position that Dukakis fully supported – meant the state would cooperate with the plaintiffs in the case. Those plaintiffs included Ben Ricci, who had brought the original lawsuit on behalf of his son, who was a resident of the then Belchertown State School.
Founding of COFAR
Grenon also interviewed John Sullivan, one of the founders of COFAR, whose daughter, Colleen Lutkevich, continues to work with this organization.
Sullivan, who died in 2017, told Grenon in 2012 that he had helped start COFAR in 1984 as a counter to the Massachusetts Arc and to Rhode Island Senator John Chaffee, both of whom were pushing to close all of the state schools and transfer all of the residents to privately run, community-based group homes.
Sullivan and other like-minded advocates, including Ricci, Charles Hart, Richard Krant, and Louise Johnson, believed that the improvements brought about by the Ricci litigation had transformed Wrentham and the other state schools into the best possible settings for their loved ones by the mid-1980s.
Personal experiences
But Grenon’s book is based on more than historical research and even interviews. She also recounts her own experiences at Wrentham, having worked there for 34 years in a variety of capacities, starting in 1981. Her personal descriptions draw the reader into the day-to-day life and drama of the institution during her time, and add to the context and richness of the center’s history.
Grenon started working at Wrentham after graduating from college with a degree in psychology. Her first job was as a direct care worker, a position referred to at the time as a “Mental Retardation Assistant.” She spent most of the next four years with the “heavy hitters” — women in the D Building who were given that appellation because they had behavioral problems.
In 1982, Grenon was promoted to ward supervisor, and then became building manager, and later back-up shift supervisor and crisis responder.
In 1985, because of her separate degree in equestrian science, she became director of a new therapeutic horseback riding program at Wrentham. And from 1992 until 2014, she served as a coordinator in public relations at Wrentham and as a community liaison.
In 2016, Grenon discussed her book and emerging therapies and models of care for people with I/DD in a series of interviews, including this one.
Opposition from DDS
But as Grenon explained to me, the Department of Developmental Services (DDS) was not happy with her book. She said that when top DDS administrators learned she was writing it, they wanted her to emphasize only “the most egregious” aspects of Wrentham’s history.
The reason for DDS’s position is clear. Since the 1990s, a succession of administrations in Massachusetts has been intent on shutting down state-run residential care and privatizing the services. But Grenon told the Department officials she wanted to tell the whole history of Wrentham, both good and bad.
The result, she said, was that she was repeatedly threatened by DDS with termination in the last few years of her employment, and was later even banned from visiting the campus.
Grenon said that at a meeting with the DDS administrators in 2013, “They all wanted to know why I wanted to present the facility in a positive light, and I told them something like, ‘up until now, everything that has ever been written about facilities has been very negative. I’ve found some surprising evidence to the contrary and I want to present it. I don’t just want to regurgitate egregious conditions, I want to present facts.’”
Grenon said, though, that the reply from one of the administrators at the meeting was, “’We would really rather that you present the egregious conditions. . .’” She said she was also told “not to make the facility look good.”
As we’ve argued before, it is vitally important to study the history of the care of persons with I/DD in Massachusetts and elsewhere, if only to avoid repeating the mistakes of the past. It is just as important to recount the entire history, and, as Grenon said, to present the facts.
It is only in recounting the full and complete history of any person, event, trend or institution that valid conclusions can be drawn as to the meaning of the past and how to plan for the future. That is what Grenon sought to do in writing her book; and, in our view, she fully succeeded.
Is RFK Jr. open to reversing the longtime federal policy of phasing out state-run and ICF care?
Late last month, we sent a message to Robert F. Kennedy Jr. via his Make America Healthy Again (MAHA) website, asking whether he would support the preservation of state-run, congregate and group home care for persons with intellectual and developmental disabilities (I/DD).
RFK, who has been nominated by President-elect Donald Trump to head the U.S. Department of Health and Human Services (HHS), has spoken out about what he refers to as the capture of governmental agencies and regulators by the pharmaceutical, agricultural and other industries. He has cited the undue influence of corporate interests in healthcare, in particular.
While there are many people who are skeptical of Kennedy, primarily due to his controversial statements about COVID and other vaccines, our main concerns center around the future of residential care for people with I/DD. Would Kennedy’s efforts to rein in corporate interests in healthcare include reining in corporate providers that contract with states to run group homes for people with I/DD?
In our message to Kennedy, we asked whether he would be “committed to changing the direction in which HHS and the U.S. Department of Justice (DoJ) have long been headed in furthering the runaway privatization of human services and the closures of state-run services for people with I/DD, including Intermediate Care Facilities (ICFs).”
We understand that there are many people competing for Kennedy’s attention right now, and that it might be some time before we hear back. We hope we do hear back.
Privatization proponents acknowledge problems, but oppose the use of institutional resources
As we noted in our message to Kennedy, the privatized system of care in Massachusetts and elsewhere in the nation for people with I/DD is broken.
In Massachusetts, the state Department of Developmental Services (DDS) is funding the privatized group home system at close to $1.7 billion in the current fiscal year — an increase of more than 60% from a decade previously. Yet, thousands of people are waiting for residential placements in group homes that are rife with abuse and neglect and underpay their direct-care staff. The executives who run those corporate providers make exorbitant salaries.
Massachusetts has just two remaining state-run ICFs, which serve as a critical backstop for residential care, and meet strict federal standards for staffing and treatment. They are the Wrentham Developmental Center and the Hogan Regional Center. Yet a succession of administrations has let these facilities die slowly by attrition, and has steadily increased funding to corporate group-home providers.
Also being phased out in this state is a smaller network of state-run group homes, which provide care from well-trained staff. Families and guardians seeking residential placements for their loved ones with I/DD are not informed of these state-run options, and, when they do seek those placements, are routinely denied.
Federal government has pushed for ICF closures
As we noted to Kennedy, this same anti-congregate care trend has long been encouraged at the federal level. The federal Centers for Medicaid and Medicare Services (CMS) and the Civil Rights Division of the DoJ have pursued a relentless policy for years of deinstitutionalization and privatization of services. This policy has been promoted under the guise of civil rights, with the misleading argument that congregate care segregates people with I/DD.
Not only has the DoJ filed unnecessary and unwanted lawsuits around the country to close ICFs, but the federal government has encouraged the closures of important and highly successful programs such as sheltered workshops for people with I/DD. This has been done under the mistaken ideology that all people, no matter how severe their disabilities, can compete and succeed in the community-based system.
However, the U.S. Supreme Court in Olmstead v. L.C. recognized that institutional care is valid and appropriate for those who desire it and who can’t cope in the community.
Yet the single-minded focus of the federal government and other proponents of privatization on eliminating institutional care has caused the proponents to ignore the serious problems with community-based care.
Biden administration increased funding for community-based care, but not state-run ICFs
Over the past four years, the Biden administration increased Medicaid funding to states for home and community-based services. But as COFAR and a key state employee union, AFSCME Council 93, noted in a joint letter to Massachusetts Senator Elizabeth Warren in 2021, the Biden administration was not similarly proposing any additional funding for state-run ICFs.
Many advocates for the disabled are worried today that the incoming Trump administration will reverse the Medicaid gains that the home and community-based system has received under the Biden administration. They are particularly concerned that under the leadership of Kennedy and Mehmet Oz, who has been nominated to head the CMS, Medicaid funding to the states will be replaced by block grants, and individual recipients will be subject to work work requirements.
While we understand these concerns, we would also note that pumping more Medicaid dollars into a flawed, privatized system won’t solve the problems that continue to plague that system.
As we stated in our message to Kennedy, we believe that the states need to reopen the doors of their state-run ICFs and group homes before it is too late. If we lose these critical residential options, we foresee a race to the bottom in the quality of care for thousands of our most vulnerable residents.
However, the Healey administration in Massachusetts, like several before it, takes its cue from the federal government, and is pushing us ever closer to the demise of state-run and ICF-level care.
A compelling new book chronicles a girl’s life at the Belchertown State School
Edward Orzechowski has done it again. He has written a second gripping, as-told-to account of life within the notorious and now long-closed Belchertown State School in western Massachusetts.
The launch of his new book, “Becoming Darlene,” is scheduled for November 23 at 1 p.m. at the Florence Civic Center in Florence, MA.
“Becoming Darlene” is about the life of Darlene Rameau, a former Belchertown resident, as related in a series of interviews with Orzechowski. It follows a similar pattern to that of Donald Vitkus, whose experience before, during, and after Belchertown, was the subject of Orzechowski’s first book, “You’ll like it Here.”

In each case, Orzechowski, a former COFAR Board member, has written the life story of a person who spent most of their childhood at the Belchertown school. When Donald was first sent there in the 1950s, and Darlene in the 1960s, that institution, like a number of others in Massachusetts, was a literal warehouse of abuse and neglect.
It is important to understand that the type of institution that Orzechowski describes in both of his books no longer exists today. Starting in the mid-1970s, while Darlene was still at Belchertown but Donald had long since left it, major upgrades in care and conditions began to be implemented at that and other similar institutions in Massachusetts. These changes were the result of a class action lawsuit first brought by Benjamin Ricci, the father of a former Belchertown resident.
The upgrades were overseen by U.S. District Court Judge Joseph L. Tauro. By the time Tauro disengaged from his oversight of the case in 1993, he wrote that the improvements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
As Orzechowski notes, Darlene became aware while she was still at Belchertown of the impact of Tauro’s involvement. Suddenly, and seemingly in one day, new, kinder staff appeared. Restrictions and beatings ended, Darlene says. But those changes still took many years to be fully implemented.
In 1996, Belchertown was closed for good. Today, only two large congregate care facilities remain in Massachusetts — the Wrentham Developmental Center and the Hogan Regional Center. Both centers must meet strict federal standards for care and staffing that were made possible by the federal litigation in Massachusetts and in other states starting in the 1970s.
At Belchertown, Darlene was a keen observer of nonstop human suffering, of wards filled with naked, neglected children, and reeking of urine and feces and infested with insects.
As was the case with Donald Vitkus’s story, much of the story about Darlene is about her attempts to cope in the “real world,” after having been discharged from Belchertown. For both Donald and Darlene, the transition was filled with trials and setbacks. Belchertown continued to affect both of their lives in sometimes tragic ways.
“Becoming Darlene” is a true story, but it reads like a novel. It is a page turner. It is at turns disturbing and heart breaking. But as with Orzechowski’s first book, one finishes this second book with a feeling of gratitude for Darlene and for the triumph of her spirit.
Does the state commission on the history of institutional care have a private agenda?
A year into the operation of a state commission on the history of the former Fernald Developmental Center and other state institutions, the commission members apparently have yet to discuss that history.
As a result of that and other evidence, we are concerned that the commission’s real purpose may be something else entirely.
In fact, the evidence shows the commission may be poised to recommend the closure of the last two existing state-run congregate care facilities for persons with intellectual and developmental disabilities in Massachusetts — the Wrentham Developmental Center and Hogan Regional Center.
Our concern is based on online minutes and recorded Zoom meetings of the Special Commission on State Institutions since those meetings began in June 2023. It is also based on prejudicial statements made prior to the establishment of the commission by individuals later appointed to the commission and by organizations given appointing power to the commission.
The commission’s enabling statute states that the commission will “study and report on the history of state institutions for people with intellectual or developmental disabilities or mental health conditions in the commonwealth including, but not limited to, the Walter E. Fernald state school and the Metropolitan State hospital.”
However, a provision in the statute also states, in part, that that the commission’s work “may include recommendations for… deinstitutionalization…(and regarding) the independent living movement.”
Why would a commission established to study and report on the history of state institutions also be authorized to recommend deinstitutionalization — in other words, the closure of currently existing institutions?
The minutes and Zoom recordings of the commission’s meetings thus far indicate that the major subject that appears to have been off the table for discussion has been the history of the state institutions. There simply don’t appear to have been any discussions reflected in the minutes about that history, pro or con. Instead, the discussions have been about numerous peripheral issues.
Might that lack of discussion about institutional history mean the commission has already reached its conclusions?
The commission is required to submit a report to the Legislature with its findings and recommendations by June 1, 2025.
We have repeatedly expressed concern that the commission would examine only the history of the institutions prior to the 1980s when those facilities were notorious for abuse, neglect and poor conditions. We have contended the commission would likely ignore the history of the state institutions after significant improvements to them were made and overseen by a U.S. District Court judge in the 1980s.
We reviewed the minutes and Zoom recordings of the commission’s meetings, which have been posted on line. The meetings were held on June 1, September 6, and October 20, 2023, and on January 18 and March 21 of this year.
Among the additional evidence for our concerns are that:
- No clear direction thus far appears to have been publicly provided by the commission to its consultant, the Center for Developmental Disability Evaluation and Research (CDDER), regarding the scope of the commission’s inquiry. CDDER, which is part of the UMass Medical School, will apparently be charged with writing the commission’s report.
- There has thus far been no participation on the commission, as required, by a family member of a current resident of the Wrentham Center. That appears to be the only position on the commission that has gone unfilled to date.
A family member, who did initially agree to serve on the commission, said he was told by an administration official that he couldn’t continue to serve because he lives out of state. However, nothing in the commission’s enabling statute requires family members to live in Massachusetts in order to serve on the commission.
During the legislative process to create the commission, we argued for the inclusion on the commission of family members of current residents of both Wrentham and Hogan in order to help ensure that the commission will at least focus to some extent on the high level of care currently provided in those facilities.
According to the minutes, it was only in March of this year, nine months after the start of the commission meetings, that a family member of a current Hogan resident was apparently appointed.
- Four members of the 17-member commission include Healey administration officials or designees, and an additional seven members are appointees of the governor.
The administration has been blocking admissions to the Wrentham and Hogan Centers – a policy that is leading to a steady decline in the number of residents in those facilities. We are concerned that by the time the commission is scheduled to issue its report, the cost per resident at Wrentham and Hogan will have risen to a point at which the administration will begin making a case for the closure of the centers.
Wrentham and Hogan, the state’s two remaining Intermediate Care Facilities (ICFs), provide intensive residential services and are a critical backstop for care for some of the most severely intellectually disabled residents in the commonwealth.
We are concerned that the eventual closure of Wrentham and Hogan is being planned by the Healey administration. The administration and state Legislature, in contrast, have continued to increase the budgetary line item for community-based group homes to over $1.7 billion in the current fiscal year.
Commission members have made previous prejudicial statements
Proponents of the commission made statements prior to serving on the panel that were almost uniformly negative about care at the former Fernald Center, in particular. Those criticisms of Fernald were exclusively focused on the institution’s history prior to the 1980s, and never acknowledged improvements made at Fernald and other similar ICFs after that period.
For instance, several organizations, which were authorized under the commission’s enabling statute to appoint members to the commission, signed a petition and letter to Waltham Mayor Jeannette McCarthy in December 2021 opposing a Christmas light show on the Fernald grounds because Fernald had allegedly exclusively been a site of abuse and neglect. That petition, and one prior to it the previous year, stated that:
The use of this (Fernald) site (for a Christmas light show) is both disturbing and inappropriate, given its history of human rights abuses and experimentation on children. Hosting the Greater Boston Celebration of Lights here ignores the fact that the people who lived at the Fernald School were denied holidays with their families and loved ones for generations.
It appears the minds of the signers of that letter and petition had already been made up about Fernald before the commission was created. Neither the petition or letter noted the positive transformation of Fernald starting in the 1980s, nor the opposition of many families to Fernald’s closure in 2014.
Among the signers of the 2021 petition and letter to McCarthy were four organizations that were later given authorization under the enabling statute to appoint members to the commission – the Arc of Massachusetts, Mass. Advocates Standing Strong, Mass. Families Organizing for Change, and the Boston Center for Independent Living.
A member of a fifth organization, Kiva Centers, which also signed the petition and letter to McCarthy, is also serving on the commission, according to the minutes. Kiva Centers is not specified in the enabling statute as being authorized to appoint a member to the commission.
Alex Green, one of the principal backers of the commission’s enabling statute, started the petitions against Fernald and made numerous negative statements about Fernald, including writing a commentary in November 2020 that advocated deinstitutionalization. Green was appointed to the commission by the Arc of Massachusetts.
In his commentary, Green stated:
I have no doubt that a full reckoning with disability history would have led us to create a society better than this one, where the deaths of disabled Americans — who are often still forced to live in institutional settings — are as many as the anonymous ditches bulldozed for bodies (of persons who died during the COVID pandemic) on Hart Island in New York. (Link in the original.)
Enabling statute is vague about historical scope, but specifies deinstitutionalization and ‘the independent living movement’
The commission’s unclear focus appears to be at least partly due to the vagueness of the commission’s enabling statute, which was enacted as an amendment to the state’s Fiscal Year 2023 budget. A more carefully drafted bill, (H. 4961) which would have given COFAR an appointment to the commission, died in a legislative committee in July 2022.
As noted, the enabling statute states that the commission will “study and report on the history of state institutions for people with intellectual or developmental disabilities or mental health conditions in the commonwealth including, but not limited to, the Walter E. Fernald state school and the Metropolitan State hospital.”
The statute does specify that the commission will review records of former residents of the institutions, assess records of burial locations of those residents, and try to find unmarked graves of residents. But none of those requirements describes the nature of the history the commission will study or the purpose of such a study.
A final requirement in the statute states that the commission will:
…design a framework for public recognition of the commonwealth’s guardianship of residents with disabilities throughout history, which may include, but shall not be limited to, recommendations for memorialization and public education on the history and current state of the independent living movement, deinstitutionalization and the inclusion of people with disabilities. (my emphasis)
It’s not clear what, if anything, that provision in the statute has to do with the history of the state institutions. However, the provision does appear to allow the commission to recommend deinstitutionalization, which we think could mean closures of the Wrentham and Hogan Centers.
The provision also states that the commission may issue recommendations regarding the “independent living movement.” The independent living movement is not defined, but it appears to stand in opposition to congregate care in ICFs. As such, it appears to refer to “community-based” group homes or other community-based living arrangements such as staffed apartments or staffing in private homes.
While so-called community-based care works well for many high-functioning individuals, we have maintained that ICFs remain a critically important option for persons who cannot function in the community system.
Rejected bill contained independence clause and gave COFAR appointment
The previous bill, H. 4961, which had been reported favorably by the Mental Health and Substance Abuse Committee in July 2022, was also vague about how the commission would research and report on the history of the institutions. But it had a number of provisions that would have been helpful to the commission’s charge, but which were removed in the final, budget amendment version.
The rejected bill had stated that the commission would be “independent of supervision or control by any executive agency and shall provide objective perspectives on the matters before it.” That language was taken out of the final budget version.
Also, the rejected bill stated that the commission would “assess the quality of life” of residents currently living in state institutions, including Wrentham and Hogan, and would collect testimonials from current and former residents of state institutions, including Wrentham and Hogan, as part of a human rights report. That provision was also taken out of the final budget version.
Finally, the final version of the enabling statute removed a provision in H. 4961, which would have given COFAR the authority to appoint one person to the commission. The final version of the statute, however, kept that appointing authority for the Arc and the other anti-ICF organizations mentioned earlier.
Focus on issues irrelevant to the history of the institutions
As noted, the commission’s minutes don’t appear to contain any discussion about the actual history of the institutions. Instead, the commission’s discussions appear to have focused on such things as:
- The discovery, a decade after Fernald’s closure, of records of residents that were left behind in a state of disarray on the floors of abandoned buildings on the Fernald campus.
While this is a serious issue that needs to be investigated, it has nothing to do with the history of Fernald or the other institutions while they were in operation. The fact that the Fernald records breach has been the focus of discussion in at least two commission meetings may be an indication of the vagueness of the commission’s scope of inquiry as set out in the enabling statute.
- The hiring of CDDER as the commission’s consultant.
The first commission meeting, held on June 1, 2023, contained a preliminary discussion of a plan to hire a consultant to the commission for “staffing support,” and to use $145,000 in funding allocated to the commission for that purpose.
The commission’s second meeting on September 6 included a discussion of a recommendation that the commission hire CDDER as the consultant. It still wasn’t clear what the consultant was being hired to do.
In the third commission meeting on October 20, the commission voted to hire CDDER, with discussion that CDDER would likely be writing the commission’s report to the Legislature. It doesn’t appear that the commission considered any other consultants for the job.
- The creation of commission working groups for tasks including sending a letter of inquiry to Governor Healey about the records of residents of the state facilities and how to protect and access them; the status of burial locations of former residents; and “developing a framework for recognition” of former residents, including developing memorials.
No working group was established to develop the scope of the commission’s primary charge to study of the history of the institutions.
Family member of Wrentham resident told he could not serve
A family member of a Wrentham Center resident was actually recruited by the director of the Wrentham Center in December 2022 to serve on the commission.
That individual, who lives in Connecticut, said he had scheduling conflicts, but did attend a commission meeting in October 2023. But he said that shortly after that meeting, he was notified by an administration official that he was not eligible to continue to participate on the commission because he lives out of state.
Despite what that family member was apparently told, the commission’s enabling statute does not state that members of the commission must live in the state of Massachusetts. A Guide for Members of Boards and Commissions, published by the Inspector General’s Office, also does not state that living in Massachusetts is a requirement in general of such members.
Commission wasn’t established in good faith
In summary, we don’t believe this commission was established in good faith to study the full history of the state institutions.
The evidence for our conclusion includes the prejudicial statements made by some of the key commission members and organizations involved with the commission, and the language in the enabling statute that specifically says the commission may recommend deinstitutionalization.
Either this is a commission established to study the history of the institutions, or it is a commission established to recommend closure of existing institutions. It can’t and shouldn’t be both, but that is what the enabling statute appears to allow the commission to do.
In fact, the language in the enabling statute authorizing the commission to recommend deinstitutionalization is buried in a dense word salad that appears intended to hide that authorization.
Other evidence includes the enactment of the enabling statute as a budget amendment in an apparent end-run around the more carefully drafted legislation in 2022. As part of that end-run, COFAR’s appointment to the commission was rescinded.
The commission has subsequently failed to appoint a family member who might conceivably have good things to say about the current level of care at the Wrentham Center.
Finally, the evidence includes the lack of discussion in the commission meetings about what the commission is actually going to do. The actual discussions have focused on peripheral issues, including the breach in the storage of confidential records of former Fernald residents a decade or more after Fernald was closed.
All of this evidence may be circumstantial, but there’s an awful lot of it; and we just don’t think it’s all coincidental.
Why we are asking federal and state lawmakers to help save the Wrentham and Hogan Intermediate Care Facilities
We believe individuals with intellectual and developmental disabilities in Massachusetts have a right under federal law to care at the Wrentham and Hogan Intermediate Care Facilities (ICFs).
They also have a right to work opportunities in their day programs and other congregate care settings.
Those rights are under continued assault. (See here and here.)
As a result, we are contacting members of the Massachusetts delegation in Congress and key members of the state Legislature, and are asking them to relay information about those rights to policymakers at the federal and state levels.
It seems to us that most lawmakers and policymakers do not recognize the wide range of functioning and needs among people with intellectual and developmental disabilities, or the importance of giving this population a full continuum of choice. One size does not fit all.
DDS phasing out state-run residential care
The Massachusetts Department of Developmental Services (DDS) is allowing the state’s two remaining ICFs — the Wrentham Developmental Center and the Hogan Regional Center — to slowly die by attrition. We believe the eventual closures of these essential backstops for care of the state’s most profoundly disabled residents will be disastrous.
So far, we have met online with legislative staff of U.S. Senators Elizabeth Warren and Ed Markey, and of Representatives James McGovern, Seth Moulton, and Catherine Clark, and imparted that message. We still have six additional members to meet with in the congressional delegation.
Next week, we will also meet online with staff of state Senator Robyn Kennedy, the new Senate chair of the Legislature’s Children, Families, and Persons with Disabilities Committee. We hope to discuss these issues with Senator Kennedy herself, at some point, and will try to schedule a meeting soon with state Representative Jay Livingstone, House chair of the Committee, and his staff.
We want these legislators to know that DDS has failed to inform families and guardians of individuals in the DDS system of the existence of the Wrentham and Hogan Centers, and, with few exceptions, has denied their requests to place their loved ones in those facilities. The Department is also failing to inform people of the existence of its network of state-operated group homes.
What DDS has done has been to attempt to place virtually all persons waiting for residential services in the much larger network of corporate provider-run group homes that the Department funds.
That policy was explicitly confirmed in a decision earlier this month in which DDS Commissioner Jane Ryder upheld the denial of an appeal by the parents of an intellectually disabled man to place their son at Wrentham.
In that case, the parents presented evidence that their son has received inadequate services in his provider-run group home. He is also facing eviction from the residence, and had been abused by staff employed by his group home and day program provider. But a DDS-appointed hearing officer adopted the Department’s position that “federal law does not entitle the (son) to admission to an Intermediate Care Facility at WDC (the Wrentham Center).”
DDS policy runs counter to federal rules
As Medicaid.gov, the federal government’s official Medicaid website, explains, “States may not limit access to ICF/IID service, or make it subject to waiting lists, as they may for Home and Community Based Services (HCBS)” (my emphasis). The son’s group home in the appeal case is run by a corporate DDS provider that is partly federally funded under the HCBS program.
Unfortunately, in his decision, the hearing officer confirmed that DDS’s policy is the opposite of the federally prescribed policy that states may not limit access to ICFs. The hearing officer stated that he agreed with the testimony of a DDS regional director in the appeal hearing that, “DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
In our view, however, the federal Medicaid law and its regulations confer the right to the choice of ICF care to individuals and their families and guardians.
DDS, like many advocates of deinstitutionalization of care for people with intellectual and developmental disabilities, has also regularly misinterpreted the landmark Olmstead v. L.C. Supreme Court decision, which also implies a right to ICF care for those who desire it.
Federal ICF legislation that we support and oppose
In our meetings, we are urging lawmakers in Congress to oppose pending bills that would expand funding to largely privatized HCBS system, but would not direct similar funding to ICFs.
We oppose:
The Latonya Reeves Freedom Act of 2023
- H.R. 2708 (Steve Cohen, D-TN) https://www.congress.gov/bill/118th-congress/house-bill/2708
- S.1193 (Michael Bennett, D-CO) https://www.congress.gov/bill/118th-congress/senate-bill/1193
As Hugo Dwyer, executive director of the VOR, our national affiliate explained, this legislation was proposed by ADAPT, an organization that has “repeatedly called for the elimination of the ICF model.” Dwyer stated that VOR supports “keeping all services available and allowing individuals and their families to choose what is right for them.”
- H.R.547 (Debbie Dingell, D-MI) https://www.congress.gov/bill/118th-congress/house-bill/547
- S.100 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/100
- H.R.1493 (Debbie Dingell, D-MI) https://www.congress.gov/bill/118th-congress/house-bill/1493
- S.762 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/762
Dwyer noted that these latter bills would increase federal Medicaid funding for direct-care wages, which we and VOR support. But those wage increases would be in HCBS settings only, leaving out the ICFs.
We support:
Recognizing the Role of Direct Support Professionals Act
- H.R.2941 (Brian Fitzpatrick, R-PA) https://www.congress.gov/bill/118th-congress/house-bill/2941
- S. 1332 (Maggie Hassan, D-NH) https://www.congress.gov/bill/118th-congress/senate-bill/1332
Dwyer said these bills would help raise wages and training of direct-care staff in all settings, including ICFs.
Work opportunities legislation
With regard to work opportunities for people with intellectual and developmental disabilities, two pending bills in Congress would encourage such opportunities:
We support:
- H.R.1296 (Glenn Grothman, R-WI) https://www.congress.gov/bill/118th-congress/house-bill/1296
- H.R.553 (Glenn Grothman, R-WI) https://www.congress.gov/bill/118th-congress/house-bill/553
The Restoration of Employment Act would give an individual a choice whether to accept employment at a subminimum wage. (This blog post explains why the subminimum wage is needed by people who are unable to compete in the mainstream workforce.)
The Workplace Choice Act states that a program setting in which an intellectually disabled individual is able to interact with “colleagues, vendors, customers, and superiors…” would be considered a “competitive, integrated employment” setting. This would allow people who can’t compete in the mainstream workforce to be provided with work activities in their day programs.
We oppose:
- H.R. 1263 (Bobby Scott, D-VA) https://www.congress.gov/bill/118th-congress/house-bill/1263
- S.533 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/533
- H.R. 4889 (Bobby Scott, D-VA) https://www.congress.gov/bill/118th-congress/house-bill/4889
- S.2488 (Bernie Sanders, I-VT) https://www.congress.gov/bill/118th-congress/senate-bill/2488
The legislation above would make work opportunities harder to find for people who can’t handle mainstream work environments. Those bills would remove the option of the subminimum wage.
A number of family members have joined us in our online meetings with legislators. If you are interested in attending upcoming meetings, let us know. Your stories are vitally important for lawmakers and policymakers to know.
In ruling criticized as biased, DDS denies family’s request to place son at the Wrentham Center
As had been expected, Department of Developmental Services (DDS) Commissioner Jane Ryder last week upheld the denial of a request by a couple to place their intellectually disabled son at the Wrentham Developmental Center.
Ryder upheld a recommended decision by DDS Hearing Officer William O’Connell, who had previously denied a request by the couple to submit a COFAR blog post in rebuttal to a DDS closing brief in the case.
The COFAR post claims, among other things, that federal law gives individuals a right to care in an Intermediate Care Facility (ICF) such as the Wrentham Center.
The couple, who have asked that their names not be used, have sought the Wrentham placement as part of an appeal of their son’s Individual Support Plan (ISP). They contend the DDS-funded corporate provider that operates their son’s group home and day habilitation program does not provide services their son needs, such as nursing, speech and occupational therapy; and they note that these services are provided at Wrentham.
O’Connell’s 24-page recommended decision denying the couple’s appeal was dated July 20. The couple maintain that the language and reasoning in O’Connell’s decision confirms that he held a bias against them and in favor of DDS.
Son had been abused at day hab program and is facing eviction from group home
The couple also stated in their appeal that their son had been sexually and physically abused in his day hab facility. They further stated that the provider sought last September to evict their son from the group home after he had a toileting accident on the group home’s outside deck.
The eviction is currently on hold based on the couple’s objection to it under DDS regulations.
The couple said they are considering an appeal of O’Connell’s decision in state Superior Court. They said their hope is that a win in court would establish a precedent for other families seeking to place their loved ones with intellectual and developmental disabilities at either Wrentham or the Hogan Regional Center, the two remaining congregate ICFs in Massachusetts.
In ruling against the couple, O’Connell cited the testimony of two DDS regional directors during a hearing on the couple’s appeal in April. O’Connell stated that based on that testimony, he concluded that “the assessments and/or goals used to develop (the son’s) ISP…form a more than adequate basis for service planning for (the son), including his needs and treatments.”
O’Connell also stated in his decision that the son’s current services are “the ‘least restrictive’ to meet (his) current needs.”
O’Connell’s decision, however, largely did not address the couple’s contention that the actual services their son has received in his group home are inadequate.
Also, as COFAR pointed out in the blog post, which O’Connell would not allow to be submitted, “a statement that a community-based setting is necessarily less restrictive than an ICF is an ideological position that ignores the evidence.”
Hearing officer appeared to have a bias against the family
The couple further noted to us that the regional directors whose testimony was cited by O’Connell are bureaucrats who are largely unfamiliar with the day-to-day care of the son. Yet, the couple said, O’Connell clearly placed all of his credence in the directors’ testimony and not in their own testimony.
In his final decision, O’Connell used the term “credible” or “credibly” to describe the testimony of the two DDS regional directors at least 14 times, while repeatedly stating that the couple had “not met the burden of proof” and had not provided “probative evidence” to support their request that their son be placed at Wrentham. He didn’t explain why their evidence wasn’t probative.
The mother also told us that during the April hearing, O’Connell had expressed repeated impatience with her, telling her to “get to the point…” She said he never interrupted the DDS attorney.
O’Connell had also stated in his previous ruling that the COFAR Blog post was “not probative” as a reason for refusing to consider COFAR’s rebuttal to the DDS closing brief. The blog post would have required him to address several points including:
- That the federal Medicaid statute does provide a right and choice to individuals and their families to ICF care.
- That care at Wrentham and Hogan is not necessarily more restrictive than in provider-run group homes.
- That the couple’s son’s care in the community-based system has not been successful for the past 13 years, as the DDS closing brief stated, and O’Connell repeated.
- That DDS’s policy for many years of blocking new admissions to both Wrentham and Hogan is likely to result in the eventual closure of both of these vitally important backstops of care for some of the state’s most vulnerable residents.
In his decision, O’Connell also repeatedly stated that the couple had rejected all providers of community-based residential services that DDS had identified for them. But he did not acknowledge that the couple said they did so because they believe the community-based system has failed their son and will continue to do so.
ISP hearing process inherently unfair
COFAR has additionally questioned the fairness of the ISP appeal process, under which both the hearing officer is appointed by the DDS commissioner, and the commissioner then makes the final decision whether to uphold the hearing officer’s ruling. COFAR has called for such appeals to be decided by the state’s independent Division of Administrative Law Appeals.
Hearing officer discounted the impact of sexual and physical abuse of couple’s son
In his decision, O’Connell played down the impact of two incidents of sexual and physical abuse of the couple’s son, which the couple said were part of the reason they don’t believe the community-based system is safe or adequate for him. Both incidents had occurred in the bathroom of the day hab facility.
In one case in 2017, a staff member at the day hab program slapped the son on the head, punched him in the back, grabbed his genitals, and was verbally abusive to him over the course of several days.
In a second case in 2015, the son arrived from the day hab facility with a belt tightened so tightly that the parents couldn’t get it off. They said the belt was used to keep their son from going to the bathroom and moving his bowels. Their son has Crohn’s disease and needs to use the bathroom frequently.
According to the couple, their son cried and screamed when they tried to get the belt off. They said he had clear marks and indentations on his stomach which they photographed. In both cases, abuse was substantiated by the DDS investigations unit.
But O’Connell stated in his decision that:
I credit the (couple’s) concerns regarding (their son’s) well-being and safety given these terrible events, but find they were at day supports, not a residential placement, and thus do not have particular probative effect to the (couple’s) current appeal of the ISP and POC (Plan of Care).
O’Connell also stated, in line with the DDS closing brief, that the abuse happened five or more years ago.
But O’Connell didn’t mention that the same provider that runs the son’s day hab program also runs his group home. Also, there was no evidence presented by DDS or the hearing officer that abuse and neglect in the DDS provider system has become less prevalent in the past five years or that the abuse is unlikely to occur again.
Also, abuse in the provider system in general is not restricted to day programs, but occurs in residential settings. If the son were to be admitted to Wrentham, he would attend a day program there, where the abuse rate is likely to be lower than in the provider system.
We have found that abuse overall is lower in the ICFs than in provider run group homes.
Did not address specific services allegedly missing from the community
In a brief that they filed with their original appeal, the couple stated that there is no speech, occupational, recreational, or vocational therapy available to their son in his group home. The group home provider doesn’t provide those services, but Wrentham does.
The couple also stated that their son’s group home and day hab provider have not assigned a nurse to him or provided the name of a nurse to call in case a medical issue arises. They also said there is no nursing listed on his ISP or day hab service plan.
Also, the couple stated that no one at the group home “knows about (their son’s) health status at any given time.” For instance, they said, no member of the staff was aware their son was due for a colonoscopy in June.
The couple also maintained that in most doctors’ offices in the community, there are no accommodations for individuals like their son who have trouble waiting for long periods of time to be seen by the doctor.
O’Connell’s decision largely did not address these specific issues. However, O’Connell did respond to the couple’s contention that their son is not receiving the proper nursing care, writing that “DDS has indicated they will work with (the provider) and any subsequent residential agency to support (the son’s) specific nursing needs.”
The couple maintained to us, however, that saying DDS will “work with” the provider is a tacit admission that the service doesn’t currently exist, and is not an assurance that anything concrete will be done. Those nursing services, however, do exist at Wrentham.
O’Connell also stated that one of the DDS regional directors “credibly testified” that the couple had stated during an informal conference prior to the hearing that the son’s doctor is “excellent.” While that may be the case, the fact remains that the medical staff at Wrentham are highly trained to deal with people with intellectual disabilities, while medical staff in the community are not.
Also, O’Connell stated that the son’s difficulties in waiting at doctors’ officers “are common and easily managed by staff.” The parents disputed this, saying that if that behavior were easily managed, the problem would have been solved long ago.
Couple says son did not face discharge due to their actions
In his decision, O’Connell, once again adopting the DDS closing brief position, stated that the couple were notified last September that the son’s provider “was looking to discharge (him) from their residential placement services due to the (couple’s) actions, not due to any issue with (the son) or (the provider’s) ability to serve (the son).”
O’Connell did not say what those actions were that the parents allegedly committed. Moreover, the couple disputed O’Connell’s characterization of the matter. According to the couple’s original appeal brief, the incident that led to the discharge notice started when no staff were available in the residence to let their son inside to use the toilet.
The group home blamed the couple following the son’s accident on the group home deck, claiming they failed to clean up the area and failed to notify the staff about it. The couple dispute that charge, saying they used a sheet in their car to clean up the area and then emailed both provider and DDS officials about it.
The couple said there was one other incident that precipitated the discharge notice having to do with a Facebook post that the mother made that was critical of the staff of the group home. Neither of these incidents, in our view, are sufficient reasons to have issued a notice to evict the son. No details were provided in the hearing officer’s decision about either of those reasons for the discharge notice.
In sum, O’Connell’s decision in this case, in our view, shows exactly why the ISP appeal process is inherently unfair to families and guardians. His decision was entirely supportive of DDS’s position, and was entirely dismissive of the testimony and evidence put forth by the parents.
For the reasons the couple enumerated, we too hope they will win in court should they decide to appeal, and that this case would then set a precedent that might serve to save the Wrentham and Hogan Centers and other state-run residential programs and services from eventual extinction.
