Archive
DDS allows strictly controlled family visitation even as it relaxes COVID-19 testing requirements on providers
As Governor Baker continues to reopen the state’s economy due to declining rates of infection in the general population from the coronavirus, the Department of Developmental Services (DDS) announced it is allowing strictly controlled visitation by family members and guardians of loved ones in its residential system.
Yet at the same time, DDS appears to be reducing its levels of testing of individuals for COVID-19 in its group homes.
We strongly support the resumption of family visits. But we are concerned about the apparent lack of consistency by DDS in relaxing testing of residents and staff as the homes are being opened to visitors after a lockdown since March.
The numbers of positive tests for DDS residents are continuing to climb, and the number of deaths in the system, while still relatively low, have been rising as well.
At this critical juncture, DDS appears to be making life difficult for families and easy for providers. The new visitation rules appear not only to have onerous provisions, they contain multiple threats that visits will be terminated and family members banned from any further visits if the providers determine they are in violation of any of the provisions.
Under the new visitation rules, which go into effect tomorrow (June 10), the duration and nature of family visits will be sharply limited, and providers will have discretion to set the terms for the visits and to ban families for perceived violations.
But if DDS is so concerned about family members violating its restrictive visitation policies, the Department does not appear to be concerned that:
- An undetermined number of providers have decided that there will be no COVID-19 testing in their group homes
- Testing of staff continues to be voluntary
- The pace of mobile testing of the group home system appears to be slowing almost to a standstill
- Retesting of individuals appears to be sporadic at best or nonexistent at worst.
Last week, I emailed Christopher Klaskin, the DDS ombudsman, asking whether DDS remains committed to testing the entire group home system, or whether the Department believes that universal testing of residents and staff is not necessary or no longer necessary.
Klaskin did not respond to the question. He did say that DDS is currently “educating providers on the importance of testing and how that data ultimately will inform how we proceed in the phased reopening of our facilities.”
The declining rate of DDS COVID-19 testing may reflect a drop in the rate of testing of the population of the state as a whole. The Boston Globe reported yesterday that even as the administration is opening up businesses throughout the state, COVID-19 testing has dropped to the lowest rate in months.
Testing that has been done by DDS shows that the number of persons in the residential system is continuing to rise (see graph below), and the rate of DDS residents testing positive remains higher than general population. The death rate in the DDS system is still low, but deaths are still rising.
Given the factors noted above about the testing rate and requirements, the positive infection rates in DDS group homes may be higher than the DDS data show.
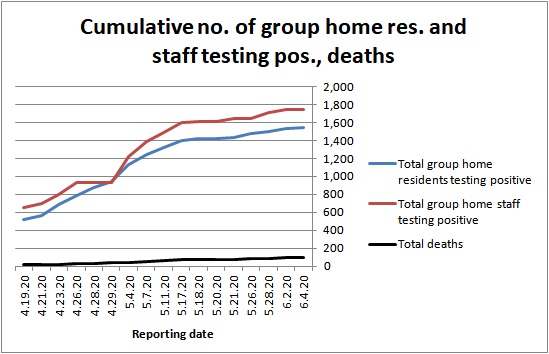
Source: DDS
Testing rate appears to be slowing
Fallon Ambulance Service, which started mobile testing of the DDS residential system on April 10, has tested only 72% of residents and staff in group homes. More than 2,000 residents have yet to be tested.
As the chart below shows, the daily testing rate by Fallon is actually down to less than 200 tests a day. The overall average daily rate since Fallon started on April 10 is 438. But that average is driven by a large spike of tests on April 29, when Fallon actually did more than 2,200 tests.
While Fallon is apparently capable of doing more than 2,000 tests per day, they haven’t done anywhere near that amount per day since the end of April.
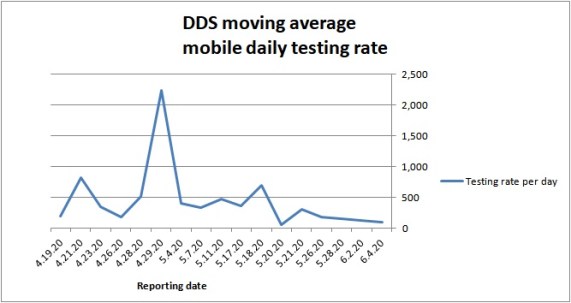
Source: DDS
We filed a Public Records Request with the state last month for Fallon’s contract and related procurement documents. The Executive Office of Health and Human Services has asked for an extension until June 12 to provide those documents.
We have expressed concerns for some time about the slow pace of Fallon’s testing, and have gotten no response from Health and Human Services Secretary Marylou Sudders as to why no additional companies have been hired to supplement Fallon’s work.
DDS says it isn’t requiring testing of all group homes
Also concerning to us is that DDS has acknowledged for the first time that not all provider residences are being tested for residents and staff who might be infected with the virus. This appears to violate DDS guidance and previous statements made by the Department.
I asked DDS ombudsman Christopher Klaskin last week about the matter after we heard from a parent of a resident of a provider-run group home who said she was informed that no one in the home had been tested because no one was symptomatic, and that the provider did not intend to implement mobile testing in its residences.
DDS guidance, which was sent in April to all providers states that the intent of the Department’s mobile testing program is to “have all individuals and staff tested,” and that those that are symptomatic would be “prioritized.” (my emphasis). That is also the message that DDS Commissioner Jane Ryder gave us when we talked with her in a conference call in April.
On Friday, Klaskin confirmed that “some locations have not requested testing” if staff or residents have not been symptomatic. Klaskin said that in those cases, DDS has told the providers that all residents and staff need to be continuously monitored and that they must request mobile testing or another means of testing “as soon as an individual shows symptoms or has been exposed to the virus.”
DDS’s written guidance, however, doesn’t state that testing will be done only if providers request it, or that asymptomatic residents can be monitored rather than tested. The guidance specifically states the Department’s intent is to test all individuals and staff.
It appears providers can avoid testing altogether by stipulating to DDS that no one in their residences is symptomatic. Thus far, 52% of provider-operated homes have reported positive cases to DDS, according to departmental data; so the remaining 48% could conceivably decline testing. We have asked DDS for the number of homes that have declined all testing.
Retesting may be being done only in ICFs and state-operated group homes
The issue of retesting of residents in the DDS system is critically important in ensuring that the true rate of infection over time is known and controlled. However, the amount of retesting that is being done in the system is unknown, and the nature of any retesting that is being done appears to be sporadic at best.
In April, when we first asked about the issue, Klaskin implied that DDS was not doing any retesting. In an email on April 20, in response to a question about the issue, Klaskin wrote, “DDS and Fallon are currently focused on testing all facilities before mobile retesting can be made available.”
Early this month, however, we began to receive reports that Fallon was actually returning to some state-operated group homes to retest residents there who had previously been tested. When I asked Klaskin about that and specifically asked where the retesting was being done, Klaskin said only that Fallon “has increased their capacity to now retest locations meeting CDC criteria for retesting.”
Klaskin didn’t respond to my questions where the retesting was being done or why some residents were being retested while others were still waiting to be tested for the first time.
Family members singled out for visitation restrictions
In light of the decision to loosen a virtually complete ban on visitation, DDS issued new guidelines on June 6. But those guidelines appear to be harder on families than the COVID-related requirements DDS is imposing on the providers themselves.
Under the new rules, families will not be allowed inside the residences for any reason. Residents are limited to two visitors at a time, and providers have discretion to limit the number of visits, times per week, and length of visits.
At the same time, the guidance says visits will be limited to a maximum of once a week and 30 minutes. Failure to adhere may result in a “termination of the visit” and a “temporary ban” on visits. DDS or providers can change the policy with “little notice,” and providers can also prohibit visits if they determine for any reason that the visits are not safe.
We have seen many cases in which providers have banned family members and even guardians from visiting loved ones on the basis of flimsy pretexts.
Yet despite the virtual ban since March on visits, and the severity of the restrictions even now, one parent said her daughter has been taken out by staff during the lockdown to commercial establishments and fast food restaurants.
There appears to be little consistency in DDS’s response to the ongoing coronavirus crisis. Even as the Department is opening up the residential system to visitors, it is slowing down the COVID-19 testing rate and allowing providers to avoid testing altogether if they stipulate that no one is symptomatic.
DDS officials will not even commit publicly to the clear statement in their guidance that all residents and staff in the system should be tested.
And despite the relaxed attitude DDS has adopted toward testing for the spread of the virus in the group home system, in particular, it is maintaining harsh restrictions on family visitation and giving providers the discretion to ban family members from residences for any perceived violations.
We think DDS needs to rethink both of those stances. The Department should recommit itself to universal testing in its system; and it should not give providers complete discretion to ban families from visits for perceived violations of overly onerous restrictions.
DDS residents have tested positive for COVID-19 at higher rate than general population
Residents with intellectual and other developmental disabilities in group homes have tested positive for COVID-19 at a significantly higher rate than the general population in Massachusetts since the end of April, according to an analysis by COFAR.
The numbers appear to demonstrate the importance of maintaining safe conditions in the homes and testing all staff, particularly if the administration begins to loosen lockdown restrictions in coming weeks.
COFAR analyzed cumulative testing data provided by both the Department of Developmental Services (DDS) and the Department of Public Health (DPH). DDS tracks testing data for residents and staff in its residential facilities, and DPH tracks and publishes testing data for the general population on a daily basis.
COFAR found that on a cumulative basis, the COVID-19 positive rate of DDS residents was 18.4% between April 23 and May 26, while the positive rate in the general population was 12.5% during that same period. That’s a 47% higher positive rate for DDS residents.
While the high rate of COVID-19 infection in nursing homes is widely known, it hasn’t been reported in the media in Massachusetts that residents of DDS group homes have apparently also contracted the virus at a higher rate than the general population.
The number of deaths in DDS group homes has been lower on a percentage basis than in nursing homes, but that death toll is continuing to rise. As of May 28, there have been 87 deaths in the DDS system, up from 78 deaths ten days earlier.
It is not clear why the death toll has been relatively low in the DDS system. But it should not come as a surprise that the conditions that have caused the quick spread of the virus through nursing homes are similar to those that exist in DDS-funded group homes.
Group homes are small, household sized facilities in which DDS residents have been locked down since March. As such, a virus can spread quickly in a group home especially if it is introduced by an outside source — namely staff who are, in many cases, not being tested.
COFAR tracked cumulative DDS and DPH testing data within a period from April 23 through May 26. DPH publishes testing data on a daily basis and breaks it down among several demographic categories.
The general population data that COFAR analyzed is contained in this linked DPH report, which is referred to as the DPH “COVID-19 Dashboard,” and is updated and published daily by that agency.
But the DPH report does not break out data for persons with intellectual and developmental disabilities. COFAR has obtained testing data on persons in the DDS system after directly contacting DDS on a daily basis.
We compared DDS and DPH testing data after April 23 because that was the first date for which we received data from DDS showing the total number of residents tested in the system. The state engaged Fallon Ambulance Service on April 10 to begin testing residents and staff in group homes and at the Wrentham and Hogan developmental centers.
Starting April 10, DDS began reporting results on positive tests on a cumulative basis. DPH has, in contrast, reported test results and test numbers on a daily basis; so we added the DPH daily testing numbers together since April 23 in order to make the numbers from both agencies comparable.
In the period between April 23 and May 26, Fallon Ambulance Service tested a total of 4,500 residents in both DDS group homes and the two developmental centers. During that time, 826 DDS residents tested positive, according to the DDS data. That appears to be a cumulative positive test rate of 18.4%.
During that same period, the DPH website document linked above shows that 320,243 members of the general population were tested in Massachusetts, and that of that number, 39,928 had tested positive — a cumulative positive test rate of 12.5%.
(Note: DDS ombudsman Christopher Klaskin maintained that the numbers provided by DDS of residents testing positive include the results of tests done by sources in addition to Fallon, whereas the total numbers of tests done reflect only those tests done by Fallon since April 10. As a result, he maintained, the numbers provided by DDS of persons testing positive cannot be compared to the numbers provided of tests done.
Klaskin said DDS doesn’t track either the number of positive results from tests done by sources other than Fallon or the number of tests done by those other sources.
As a result of Klaskin’s assertions, we limited our comparison to tests done after April 23, the date for which we first got a breakdown from DDS on the total number of residents tested. We do not think it is likely that more than a negligible number of tests have been done in the DDS group home system outside of Fallon’s mobile testing process.)
Governor, planning to restore visitation, cites declining positive test rate
According to the State House News Service, Gov. Charlie Baker said last week that COVID-19 public health data indicates “that we are trending in the right direction.” As a result, the head of the state’s COVID-19 Command Center said plans are in the works to allow people to once again visit their loved ones in long-term care settings.
Residential facilities in the DDS system have been locked down, with few visitors permitted to enter them since March. DDS group home licensure inspections have been discontinued as well.
In that light, we are urging that the administration take measures to better ensure the safety of the residents in DDS facilities. We think DDS can start in that direction by making testing of staff mandatory.
Disability Law Center echoes our concerns on staff testing and safety
A May 21 letter from the Disability Law Center in Massachusetts, a partially federally funded nonprofit organization, echoes many of the concerns COFAR has raised with regard to testing and safety conditions in the DDS system.
The DLC letter to Dan Tsai, assistant secretary for MassHealth, calls for mandatory testing of staff in the DDS system, better training of staff in using Personal Protective Equipment in group homes, and better reporting of data by DPH.
The DLC letter adds that there is still no “firm rule” which prevents direct support staff from working for multiple employers in different DDS group home settings. The letter also notes that the waiting period for previously COVID-positive staff to return to work is seven days, whereas the public health standard is 14 days.
Also, according to the letter, there are no “clearly enforced protocols” against DDS-funded staff working with COVID-positive and COVID-negative residents within the same shift. COVID-positive and COVID-negative residents “are being confined together in close quarters within group homes, often with COVID-egative residents getting little or no fresh air,” the letter stated.
The DLC letter stated that there is a lack of “strong protocols” for testing, screening, and separating transportation providers, such as van drivers, who may be COVID-positive.
The letter added that to the extent that there may be legal barriers to imposing additional safety requirements on providers, such as mandatory testing, those barriers may be overcome through DPH’s emergency powers or DDS’s ability to adopt emergency regulations, as many other jurisdictions have done.
Secretary Sudders still has not responded to us
Meanwhile, the pace of testing remains slow in the DDS system. Health and Human Services Secretary Marylou Sudders has not responded to our question, emailed to her on May 20, why only one company, Fallon Ambulance Service, is being used to do the testing.
Moreover, we received reports this past weekend that while thousands of residents are still waiting for their first COVID-19 test, residents in some group homes were being retested on a regular basis.
We have asked DDS for an explanation of the testing sequence in the group home system.
In sum, the DDS group home system remains a potential tinderbox that still could erupt if additional safety precautions are not taken. The higher-than-average COVID-positive rate of residents in the system over the past month is evidence of that potential.
It is unfortunate that at this critical juncture in the COVID-19 crisis, in which the administration is considering loosening many of the restrictions that have kept the crisis under control, top administration officials appear to lack accountability.
It is unconscionable that Health and Human Services Secretary Sudders does not feel it necessary even to respond to basic questions about the testing process for residents and staff in the DDS system.
The administration needs to do a better job of ensuring the safety of clients of the DDS system and of demonstrating to families and the public in general that it is in control of the situation.
Administration mum so far on why DDS COVID-19 testing process has been so slow
Although we have been getting data and responses from the Department of Developmental Services (DDS) to questions about COVID-19 testing results in group homes, no one in the administration is saying why the testing has been going slower than projected, and no one seems concerned about speeding it up.
According to the latest data we have from DDS, which was as of Thursday (May 21), the Department’s mobile testing provider, Fallon Ambulance Service, had tested 16,200 residents and staff, most of them in group homes throughout the system.
While that may sound like a lot, Fallon, a Quincy-based company, began testing on April 10, and has been averaging under 400 tests per day since then. DDS Commissioner Jane Ryder stated early on that Fallon had the capacity to perform up to 1,000 tests per day.
At this point, six weeks into the testing program, Fallon has tested about 65% of what we had estimated to be a total of 25,000 residents and staff in the DDS system. As we understand it, there has been no retesting of any of those persons living or working in the group homes, although we have heard that some people have been periodically retested in the Wentham and Hogan developmental centers.
Our estimate of the total number of staff in the DDS system might be low. WCVB Channel 5 news reported last night that there are a total of 34,000 staff working in the DDS system. If that is the case, Fallon has tested only 35% of the total number of residents and staff in the system.
The number of residents tested, in fact, stayed the same between Monday (May 18) and Wednesday. As of Monday, 5,600 residents and 10,200 staff had been tested throughout the DDS system.
As of Wednesday (May 20), DDS data showed the number of residents tested had remained at that same 5,600 level, while 100 additional staff had been tested. It would appear from those numbers that between Monday and Wednesday of this week, Fallon was averaging only 50 tests a day, and the company tested only staff during that time.
Despite the slow pace, the actual results of the testing continue to be important and concerning. More than 3,300 of the total staff and residents tested — or nearly 21% — have been found to have COVID-19. And the DDS data shows that more than 50% of the provider-run group homes in the state have now reported cases of the virus in their residences.
That data only underscores the importance of conducting the testing on a more timely basis.
We first raised a concern about the apparently slow pace of the testing process about a month ago. We also expressed a concern at that time — the first of many times since — that the testing process was voluntary for staff in the group homes. Apparently little or nothing has been by the administration to address either of those concerns.
Neither DDS or EHS commenting so far on the slow pace of testing
When we got the data from DDS that as of Monday, only 15,800 persons in the DDS system had been tested, I emailed DDS Ombudsman Christopher Klaskin to ask if Fallon was still the only company doing the testing. We heard reports that at least one other ambulance company was interested in supplementing the testing done by Fallon.
Klaskin wrote back to me on Wednesday, stating that Fallon “is the only provider contracted to perform mobile testing for DDS and several other EHS (Executive Office of Health and Human Services) agencies.”
Given that Fallon had by Monday been on the testing job for 39 days and was thus averaging only 405 tests a day since starting, I asked Klaskin whether any other companies had expressed interest in supplementing the testing, and why Fallon was still the only company doing the work. Klaskin declined to respond to those questions, saying Fallon is contracting for the work with MassHealth, which is part of EHS, and that I should direct my questions to them.
So, on Wednesday afternoon, I emailed EHS Secretary Marylou Sudders with essentially the same questions, and asked whether the state was seeking to contract with any additional companies to undertake the testing. Thus far, I haven’t gotten a response either from Sudders or from Jessica Lyons, the communications manager for MassHealth, whom I had also emailed on Wednesday.
Also on Wednesday, I filed a Public Records request with EHS/MassHealth and DDS, asking for the contract with Fallon for testing in the DDS system, and any related procurement documents and memoranda that address the need for the procurement, the scope of the services, the projected costs, timelines, and capacity of the company, and any applications filed by any other companies to undertake or supplement the testing program.
Testing is a critically important part of the process of getting us through the pandemic with as little additional loss of life as possible. The Baker administration has made testing a priority, and Massachusetts has, in fact, acquired a reputation as a leading state with regard to testing its residents overall.
But when it comes to ensuring the speediness and thoroughness of testing of persons with intellectual and other developmental disabilities and their caregivers, the state has once again fallen short. And no one in the administration appears to be willing to acknowledge or discuss it.
DDS may be flouting state and federal guidelines in failing to make testing of group home staff mandatory
While testing of staff for COVID-19 remains voluntary in group homes funded by the Department of Developmental Services (DDS), state guidelines appear to require testing of staff in small facilities in which at least some individuals are symptomatic.
Meanwhile, a state senator, who filed a bill (S.2657) to make testing of staff mandatory in nursing homes, is reportedly supporting mandatory staff testing in the DDS system as well. A legislative aide to Senator Jamie Eldridge said Eldridge supports amending his bill to make testing mandatory for DDS group home staff.
Eldridge’s legislative aide said he notified the Legislature’s Public Health Committee of the senator’s support for that change. Eldridge’s bill is currently in the committee.
While DDS started a mobile program more than a month ago to offer tests to every resident and staff member in its residential system, DDS has stated that the tests are voluntary for staff. In addition, DDS has no current plans to undertake periodic re-testing of either residents or staff.
We have repeatedly raised the concern that staff are potentially the main source of introduction of the virus to group homes, in which residents have been locked down from nearly all visitation since mid-March.
As a result, even as the rate of COVID-19 cases among all residents of the state has started to taper off and Governor Baker has introduced a detailed plan to reopen the state’s economy, the number of COVID-19 cases in the DDS system appears to be continuing to rise rapidly.
As of May 11, the last day for which DDS provided data to us, 1,000 provider-run homes in the DDS system were reporting positive COVID-19 cases. That is nearly 50% of the total number of provider-run homes in the system, and that was up from 900 homes reporting positive cases as of May 7. We are asking DDS for more up-to-date figures.
Despite the voluntary nature of the staff testing in the DDS system, COVID-19 testing guidelines from the Department of Public Health (DPH), dated May 13, state that “all individuals” who have “close contact” with persons showing symptoms “should be tested” for COVID-19.
Under DDS’s own guidelines, group homes appear to be a type of facility in which close contact is unavoidable. Those guidelines define “close contact” as “living in the same household as a person who has tested positive for COVID-19, caring for a person who has tested positive for COVID-19, or being within 6 feet of a person who has tested positive for COVID-19 for about 15 minutes.”
As a result, the DPH guidelines would seem to require that all staff be tested if they are working at least in those group homes in which one or more residents are symptomatic.
Also, guidelines from the federal Centers for Disease Control (CDC) identify “workers in congregate living settings” as a “high priority” for testing if they themselves have symptoms of COVID-19. Other persons in that high-priority class, if they have symptoms, are residents in those facilities and hospitalized patients.
DDS, however, is not requiring group home providers to test staff even if the workers have symptoms. While those staff are precluded from working in the residences while they are ill, they can return to work three days after recovering from their illness without necessarily getting tested.
Guidelines have some apparent contradictions regarding staff testing
Despite the clear-sounding statements in the guidelines regarding staff testing, DDS may consider that it has some leeway in complying with those statements because some seemingly contradictory language can also be found in those same documents.
For instance, while the DPH guidelines state, as noted, that anyone in a residence who has close contact with a symptomatic individual should be tested, the same guidelines also contain the following statement:
Asymptomatic individuals can be recommended for diagnostic testing at the discretion of their healthcare provider, a state agency, or an employer. Individuals are encouraged to confirm with their insurance whether the test will be covered. (My emphasis)
That language in the latest DPH guidance seems to directly contradict the previously noted language in the same document that states that “all individuals” having close contact with persons who are symptomatic “should be tested.”
Meanwhile, despite the CDC’s guidelines that refer to staff with symptoms as a “high priority” for testing, another set of CDC guidelines allows infected healthcare staff to return to work without necessarily getting tested. Those latter guidelines and guidelines from the Baker administration’s COVID Command Center both appear to leave it to the discretion of the provider or individual state agencies as to whether to re-test staff returning to work after they have recovered.
Both the CDC and the state COVID Command Center refer to “test-based” and “symptom-based” strategies for returning to work.
Guidance sent by DDS last month to all group homes appears to adopt the “symptom-based strategy” for allowing a staff worker who has COVID-19 symptoms to return to work after they have recovered without being tested. Under the DDS guidance, that worker would be prohibited from working in the group home for three days after recovering from the illness. If the staff worker were to be tested at any point and the test was positive, that worker would be excluded from work for seven days from the date of the test as long as the worker showed no symptoms.
In neither of those cases does the DDS guidance require testing or re-testing for COVID-19 before that worker can return to the group home or to one of the state’s two developmental centers.
DDS has stated that “very few” staff have so far refused to cooperate with the testing program; however, we have received a number of reports from family members of some group home residents that none of the staff in those homes, or very few of them, were being tested.
The situation is different in nursing homes in which staff testing is required if the nursing homes want to receive grant money made available last month by the administration.
DDS Ombudsman Christopher Klaskin maintained last week that DDS “continues to follow the CDC and DPH (state Department of Public Health) guidance for testing in our group homes.”
Klaskin added that both the CDC and DPH “differentiate between nursing facilities (which are health care facilities) and congregate care settings (like group homes), so operational protocols issued for these two systems are different.”
In our view, however, the CDC guidelines do not appear to differentiate between healthcare facilities and congregate care settings, but rather state that workers in both types of facilities either are or potentially are priorities for COVID-19 testing.
As a result, I wrote to Klaskin on May 13, asking why DDS does not at least require re-testing of group home staff before returning to work after those persons have previously tested positive or had symptoms.
In a related development, we have written to the chairs of the House and Senate Ways and Means Committees and to a key senator, asking for a change in a separate bill (S.2695) that would require DPH to publicly report testing data on residents and staff in DDS group homes.
The bill, as currently written, requires DPH to collect and report data on residents and staff in nursing homes and other DPH long-term care facilities as well as correctional centers. But the bill does not mention DDS group homes.
As we’ve said before, we are concerned that even as Governor Baker cautiously reopens the Massachusetts economy based on encouraging data on the incidence of COVID-19 in the population of the state as a whole, the administration does not appear to be showing the same caution or concern for clients in the DDS system.
At the very least, DDS should adhere to written federal and state guidelines regarding testing of group home staff.
We are encouraging people to call the Public Health Committee, and urging them to support an amendment to Senator Eldridge’s bill (S.2657) that would make testing of DDS staff mandatory. The phone numbers are (617) 722-1532 for the office of the Senate chair of the committee, and (617) 722-2130 for the House chair.
Reopening the Massachusetts economy could add to COVID-19 risks for those with developmental disabilities
It appears that the Baker administration is examining what has been termed “encouraging” testing and hospitalization data on COVID-19 in considering whether to reopen the Massachusetts economy.
We hope the administration will consider, among other things, testing data in the Department of Developmental Services (DDS) system. If not, this could be another example of the apparent disregard the administration has shown for the risk the virus poses to people with intellectual and other developmental disabilities.
Over the past weekend, the Massachusetts State House News Service reported that the administration was looking at “a number of (COVID-19) metrics considered key to resuming economic and social activity…” That data “showed positive signs” in the most recent report from the Department of Public Health (DPH ), the news service stated.
According to the News Service, the number of COVID-19 patients hospitalized in Massachusetts has declined in 10 of the last 13 days.
But the data isn’t encouraging in the DDS group home system. So, we are concerned that reopening the economy may add to the risks that residents and staff are facing in DDS group homes, in particular. If numbers of COVID-19 cases are still rising in the DDS system, it would have safety implications for all residents in the state.
Data from DDS show that the number of DDS provider-operated group homes reporting residents testing positive rose from 800 to 900 homes (out of 2,100 homes) in a four-day period, from May 4 to May 7. Eight additional residents and four additional staff tested positive at the Wrentham Developmental Center during that period, while the numbers at the Hogan Regional Center held steady.
Meanwhile, DDS is continuing to test residents and staff more slowly than planned, and the Department still has not made testing of staff mandatory.
Rate of testing in DDS group homes may be stalling
While testing all residents in all demographics is crucial in determining whether and when to reopen the economy and end the lockdown, the rate of testing in the DDS system does not appear to be meeting early expectations. In fact, it may actually be slowing.
Fallon Ambulance Service started testing group homes and developmental centers throughout the DDS system a month ago, and was supposed to be ramping up to 1,000 tests a day.
However, as of April 29, Fallon was performing an average of only 405 tests a day, according to numbers we’ve analyzed from DDS. A week later, as of May 7, Fallon was actually performing an average of only 396 tests a day.
DDS reported that as of May 7, Fallon had done about 11,000 tests since starting on April 10. We are estimating that there are as many as 25,000 residents and staff in the group home system.
So, at that rate, it would still take Fallon at least another month to test the entire DDS system, and that doesn’t count retesting, which they apparently aren’t doing at all. In other words, more than half of the total residents and staff in the system still apparently have not been tested even once.
On a related note, we received a response on April 29 to a Public Records request to DDS for records on testing timelines and plans for testing all residents and staff in the system. DDS said they have no such records. They also have no records regarding the total number of staff in the provider system.
Seeking mandatory testing of staff
We also submitted written testimony today to the Legislature’s Public Health Committee to urge the adoption of legislation that would make it mandatory for staff in DDS facilities to be tested for COVID-19. As we have reported, staff are currently not required to be tested in the DDS system — a situation that leaves the residents in the system vulnerable to infected staff members who may well be asymptomatic.
The Public Health Committee is currently considering a nursing home safety bill (S.2657), filed by Senator Jamie Eldridge, which would require testing of all nursing home staff for COVID-19. We are urging the committee to amend the bill to include a provision for mandatory testing for all staff working in DDS-funded group homes.
As we understand it, the administration actually issued a requirement last month that all staff in nursing homes be tested. However, no such testing requirement has been imposed for staff in DDS facilities.
Questions about compliance with DDS guidance
We are also concerned about a possible lack of compliance among DDS group homes with the Department’s guidance on admission of staff and possibly visitors to those facilities, and on social distancing among other issues concerning care and conditions.
We received a report that staff from one group home took one or more residents to another of the provider’s group homes during the ongoing lockdown, and may have also admitted several people into a group home with no clear purpose for being there.
Late last week, we asked DDS whether the Department has policies or procedures in place for monitoring compliance by group homes with the Department’s guidance regarding the admission of staff into facilities, social distancing, proper use of personal protective equipment, and related issues.
A one-page guidance document sent last month to all providers by DDS states that there will be no one admitted to any facilities except for medically necessary reasons. Any visitors or staff must be screened and have no flu-like symptoms or a fever over 100 F. In addition, all staff should wear face masks during their shifts.
While it is important that DDS has issued this guidance, it means little if the Department has no way of determining whether the management and staff in the widely dispersed system are complying with it.
In sum, the well-being and even survival of people in the DDS system depends on the quality, speed, and thoroughness of the ongoing COVID-19 testing. The current state of that testing in the system raises many areas of concern for us.
Baker administration appears to place low priority on COVID-19 threat to the developmentally disabled
Although the pace of mobile testing for COVID-19 of residents in group homes funded by the Department of Developmental Services (DDS) appears to be picking up, the testing of staff in those facilities is reportedly haphazard.
That is because it remains voluntary for staff in DDS-funded group homes to be tested even as the Baker administration has moved to make testing of staff in nursing homes mandatory.
This is one of a number of signs that the administration is treating people with intellectual and other developmental disabilities differently than it treats the elderly and other vulnerable populations. The administration, in fact, appears to be placing a lower priority on protecting people with intellectual and other developmental disabilities from COVID-19 than it places on other populations.
We have raised repeated concerns that:
- COVID-19 testing is not mandatory for staff in DDS-funded group homes, and there are currently no efforts underway to retest either residents or staff in the group homes on a periodic basis.
- Fallon Ambulance Service is increasing the pace of its testing in DDS facilities, but is still apparently too small a company to undertake even an initial round of testing in a timely manner. As of May 4, Fallon had tested roughly 10,000 residents and staff — a rate of about 400 tests a day since the testing program began on April 10.
- The National Guard, meanwhile, is reportedly being used to test residents and staff in nursing homes and other long-term care facilities overseen by the Department of Public Health (DPH).
- The state Department of Public Health (DPH) posts daily updates on the numbers of deaths in Massachusetts and the number of persons infected with the coronavirus. But while these updates include numbers of persons in “long-term care facilities,” we have been informed that DPH defines long-term care facilities as nursing homes, rest homes, and skilled nursing facilities. DDS group homes are not included in that definition.
- There is no inclusion in the DPH updates, much less a breakout, of the numbers of persons in the DDS group homes testing positive. Group homes are nevertheless long-term care facilities that function as the homes of close to 10,000 persons throughout the state with I/DD.
On April 28, State Representatives Kay Khan and Josh Cutler, the House chair and vice chair of the Legislature’s Children, Families, and Persons with Disabilities Committee, expressed concerns similar to ours in a letter to Health and Human Services Secretary Marylou Sudders. Representatives Khan and Cutler stated that:
….information about the impact of COVID-19 on the Department of Children and Families, the Department of Developmental Services, the Department of Mental Health and the Department of Youth Services congregate care facilities is lacking. The number of positive cases and deaths due to COVID-19 are rarely mentioned in (Governor Baker’s) press briefings.
We have never, in fact, seen DDS Commissioner Jane Ryder or any other DDS officials present at any of these briefings.
DDS-funded group home testing of staff remains voluntary
The state engaged Fallon Ambulance Service last month to undertake mobile testing of an estimated 25,000 residents and staff in DDS-funded group homes and in the Hogan and Wrentham Developmental Centers.
Last week, Christopher Klaskin, the DDS ombudsman, said that the Department was “exploring” the possibility of making testing of staff mandatory, but also said that “given contractual relationships with unions across state government, the development of any mandate of this type requires input and approval.”
Klaskin did not specify whose approval would be needed. When I pressed him on that question in a subsequent email, he responded that “unions are one of several stakeholders whose input (not approval) would be needed for this type of requirement.”
We are continuing to seek an answer from DDS as to whose approval would be needed to institute a mandatory testing requirement for staff.
Klaskin also maintained that “very few” staff in group homes have refused to be tested. However, we received reports this past weekend from family members of residents in three group homes who said that while the residents were tested there, few, if any, staff were tested. Each family member was told that the reason for that is that testing of staff is voluntary.
Laura Watkins, whose son Kyle is in a group home in Framingham, said on Friday that all eight residents of the facility were tested last Wednesday and that seven of them, including her son, tested positive.
Watkins said she was told by the house manager that Fallon didn’t test any of the staff in the group home. She estimates that there are as many as 25 staff, including day program staff who are now supposed to come into the home for day activities.
Michael Person, whose daughter Maria is in a state-operated group home, said he was informed on Sunday that residents of the facility were tested on Thursday. He was told that Maria had tested negative. When he asked about testing of the staff, he was told no staff were tested because it was voluntary.
“I do not understand this,” Person said in an email. “There are three shifts going in and out of the group home, seven days a week, and it is optional for them to get tested. Does that make any sense?”
In an email to COFAR on Saturday, the mother of a resident in another group home said she was similarly told that while residents of the facility had been tested, none of the staff, other than the house manager, were tested because testing of staff is voluntary. Yet, she said, the staff “are the only people who could carry the virus into the home…It makes no sense to me.”
Continuing lack of personal protective equipment and training in DDS group homes
Watkins said she believes a factor in the spread of the virus to all or nearly all of the residents in her son’s group home was a lack of personal protective equipment (PPE) in the residence. She herself brought in handmade masks for the staff on March 22.
It was only on April 16, she said, after the state issued revised guidance, that the provider, the Justice Resource Institute, provided N95 masks to staff in the home, but no other PPE. Even so, the staff were still short eight masks.
It’s not clear that the staff are using gloves either, Watkins said. She suggested that the state’s COVID-19 Command Center send teams into all of the group homes to train all staff on PPE and other issues. “I’m finding that nobody knows what to do,” she said.
Number of group homes reporting positive cases is growing
As of May 4, a total of 890 DDS-funded group homes were reporting positive COVID-19 cases — a positive test rate in the group home system of 38%. That was up from 770 homes reporting positive cases as of April 29, just five days earlier. The positive test rate at that time among all group homes was 33%.
Also as of May 4, a total of 1,127 residents and 1,223 staff in the group homes had tested positive, while 48 residents and 69 staff had tested positive at the Hogan Regional Center, and 41 residents and 42 staff had tested positive at the Wrentham Center.
There had been 44 deaths due to the virus in the DDS system as of May 4, up from 37 deaths as of April 29.
Crisis standards of care are a step in the right direction
On April 23, I listened in on a teleconference of the state Public Health Council’s monthly meeting, which touched, of course, on a range of issues relating to COVID-19 and the protection of residents throughout the state from this disease. In one respect, it was heartening to hear during that discussion that in developing crisis guidelines, an effort was made to level the playing field in allocating resources such as ventilators to persons who are seriously ill with the virus.
As we understand it, the rule now for getting a ventilator if there is a shortage is that there has to be a reasonable probability that the person will be able to survive for five years. One of the doctors on the teleconference call said this change was adopted to give equal access to ventilators and other “scarce resources” to people with disabilities.
While we appreciate that acknowledgement of the importance of equal consideration of persons with intellectual and other disabilities, we hope we can impress upon the administration the anguish that family members and guardians are feeling during this crisis.
DDS families are struggling with restrictions — as are family members of virtually all persons in long-term care facilities — on having any contact with their loved ones. But the DDS families have the added stress that comes with feeling that, overall, the administration has dismissed their concerns.,
At the very least, we think there needs to be mandatory testing of all staff, and periodic retesting of all staff and residents in the DDS system. In addition, the families in the DDS system are entitled to the same level of daily information that is being made available to families of all other long-term care residents.
DDS considering mandatory group home staff testing as COVID-19 cases continue to rise
As the number of group homes reporting positive cases of COVID-19 continues to rise in Massachusetts, a Department of Developmental Services (DDS) official said the Department is considering making staff testing for COVID-19 mandatory.
COFAR has raised a concern that there currently is not a requirement that staff working in the group homes get tested even though DDS began an effort on April 10 to test all residents and staff in more than 2,300 residences across the state.
In addition, it is not clear that DDS has any plans to test residents and staff in its facilities more than once.
COFAR maintains that infected staff may be introducing the virus into group homes and other long-term care facilities. Unless all staff are required to be tested on a periodic basis, it appears likely that positive cases and deaths will continue to increase in those residences.
Christopher Klaskin, the DDS ombudsman, told COFAR yesterday (April 27) that “mandatory testing of all employees would impact multiple EHS (Executive Office of Health and Human Services) agencies and collective bargaining agreements, and we are exploring this option.”
Klaskin added that “very few employees have refused (to be tested), and those situations are addressed on a case-by-case basis.”
In a follow-up email to Klaskin, we said it was welcome news that DDS is exploring the option of mandatory testing, but asked why DDS hasn’t made staff testing a requirement before now.
We also asked how many staff have refused to be tested. It would take only one infected staff to infect an entire group home. We also noted that because DDS is still early in the group home testing program, it is likely that the number of staff refusing to be tested will continue to grow.
An official with one DDS provider, the New England Center for Children, told Boston.com yesterday that the first case of COVID-19 in the Center’s group homes came six weeks ago from an infected staff member who was asymptomatic. The provider’s group homes were locked down even at that time.
There is similarly no requirement that all staff in nursing homes around the state be tested. More than 56% of the total deaths in the state are in nursing homes and rest homes, the Boston Globe reported this week.
Numbers of infected DDS group homes rising rapidly
Data provided to COFAR by DDS shows that over a four-day period ending Sunday (April 26), the number of DDS-funded group homes reporting positive cases of COVID-19 rose from 560 to 720, out of a total of 2,353 corporate provider-operated and state-operated residences. That is an increase from 24% to 31% in the proportion of homes reporting infected residents.
As of April 26, a total of 1,886 staff and residents in the group homes and two remaining DDS developmental centers had tested positive. That is up 252 persons from just four days earlier. There have been 30 deaths in the DDS system from COVID-19.
Repeat testing needed
Earlier this month, DDS announced that the state was contracting with Fallon Ambulance Service to begin testing staff and residents throughout the system. DDS apparently does not have a timeline for Fallon to complete its testing of what we are estimating to be 22,000 or more residents and staff in the DDS group home system.
It is also unclear whether DDS plans to have Fallon or any other entity periodically retest those individuals and staff who did test negative the first time.
COFAR President Thomas Frain termed a negative test result “a transitory label.” He added that, “Representing to the public that you are at war with the virus but aren’t retesting is akin to chasing Bin Laden across Afghanistan but allowing him free access to the Pakistan border.”
Referring to the need for repeat testing in nursing homes, Simon Johnson, a professor at the MIT Sloan School of Management and a cofounder of the COVID-19 Policy Alliance, told the Boston Globe that a single round of testing is a “recipe for disaster.”
Johnson said the state needs to move “as quickly as possible to help implement a regular comprehensive surveillance testing program for all residents and staff, so we know who is infected and who is not.” Not only do some people carry the virus without displaying symptoms, some may test negative even though they have already been infected, Johnson told the newspaper.
State may be in violation of Medicaid waiver requirements
In an email to Klaskin and DDS General Counsel Marianne Meacham on Saturday, COFAR asked whether the lack of mandatory staff testing so far is a potential violation of client safety “assurances” under the federal Medicaid Home and Community Based Waiver.
The Waiver, which authorizes Medicaid funding for group homes and other community-based programs, states that states must provide assurances that “necessary safeguards have been taken to protect the health and welfare of the beneficiaries of the services.”
Klaskin responded that DDS and all EHS agencies follow testing protocols from the Centers for Disease Control and Prevention, “so they meet all federal safety regulations.” He added that DDS “must adhere to (the testing protocols) to meet our waiver requirements and safeguards.”
Klaskin added that “pop-up” testing locations are being set up across the state, “giving state and provider staff across multiple shifts another option for testing.”
We are continuing to monitor the testing of group homes across the commonwealth, and are hopeful DDS will make the right changes, particularly making the testing mandatory and repetitive. If that happens, we think and hope the numbers testing positive will peak sooner than they otherwise would, and will start to diminish.
DDS COVID-19 testing is underway, but pace is slow and it’s voluntary for staff
While the Department of Developmental Services is now moving to test all residents in group homes throughout the state for COVID-19, COFAR is concerned about the slow pace of the testing and about a potentially major gap in the process.
That gap concerns the voluntary nature of the testing of staff in the thousands of group homes in the state. DDS officials acknowledged that staff can opt out of the testing and still continue to work in group homes.
More than 1,300 residents and staff of DDS group homes and developmental centers had tested positive for COVID-19 as of April 19, according to numbers that we are now beginning to get from DDS.
In the DDS group home system, 518 residents and 653 staff had tested positive, including both provider and state-employee staff.
More information has been available about the situation in the developmental centers than in the group homes.
As of April 19, 46 residents and 90 staff had tested positive at the Hogan Regional Center in Danvers. There has been one death at the center.
In the Wrentham Developmental Center, 14 residents and 13 staff have tested positive.
As of Wednesday, most clients at Hogan with COVID-19 were reported to have mild symptoms. Many were in recovery and had completed a 14-day quarantine period and were symptom free. Workers at Hogan are reported to be fully gowned, gloved, and masked.
Staff testing is voluntary
Christopher Klaskin, the DDS ombudsman, said this week that staff in group homes can opt not to be tested even if residents in the homes in which they work are symptomatic or have tested positive. Under current DDS guidelines, the staff have to have their temperature taken before entering the residences and can’t have a temperature above 100.0 degrees.
COFAR is questioning the voluntary nature of the staff COVID-19 testing, arguing that staff who are positive but asymptomatic could be bringing the virus into group homes where the virus could then spread rapidly.
“Unless all staff and residents are tested, the virus still has the upper hand,” COFAR Board President Thomas Frain said.
Colleen M. Lutkevich, COFAR’s executive director, said the organization has received reports that testing of staff is not being offered by some providers and that each provider is making their own decision about it. Taking temperatures but not actually testing staff for the virus “misses all of the asymptomatic carriers in this vulnerable population,” Lutkevich said in an email to DDS.
Guidance issued by DDS to all providers on April 13 does not include any specific testing requirements for staff or residents other than stating that the permission of a guardian is needed before residents can be tested. DDS officials have stated that it would be unusual for a guardian to refuse to consent to testing of a resident for COVID-19.
Regarding staff, the DDS guidance states only that a staff member who does test positive for COVID-19, but who does not show symptoms of the virus, is excluded from working in the residence for at least seven days from the date of the test. A staff member who tests positive and who does have symptoms is excluded from working for three days after they have recovered from the illness and at least seven days since the symptoms first appeared.
Slow start to the testing
COFAR is also concerned about what appears to be a slow start to the testing of residents and staff in the group homes. Earlier this month, DDS announced that the state was contracting with Fallon Ambulance Service to begin testing staff and residents throughout the system.
Klaskin said DDS does not have a timeline for Fallon to complete its testing of what we are estimating to be 22,000 or more residents and staff in the DDS group home system. It’s unclear why the National Guard is apparently being used to test residents and staff in Department of Public Health (DPH) nursing homes and other long-term care facilities, but not in DDS facilities.
DDS reported that as of April 19, 1,964 residents and staff had been tested in DDS group homes and at the Wrentham and Hogan centers by Fallon. This averages to less than 196 tests a day over the first 10 days in the group homes.
In an email sent to a COFAR Board member earlier this month, DDS Commissioner Jane Ryder stated that Fallon had the capacity to do up to 1,000 tests a day.
DDS does not have data on total test numbers in group homes
It is apparently not possible to compare the number of residents and staff testing positive in DDS-funded group homes with the total number actually tested.
As noted, a total of 518 residents and 653 staff have tested positive in the group homes. That number, however, includes people tested before Fallon started, Klaskin said.
While Fallon has tested 1,964 residents in the past 10 days, Klaskin said DDS doesn’t have information on the total of the number of persons tested prior to Fallon. So there appears to be no way to compare apples to apples in that respect.
DDS testing numbers not broken out by either COVID-19 Command Center or DPH
DPH, meanwhile, continues to track and publicly report detailed numbers on COVID-19 cases in nursing homes and other long-term care facilities that the department oversees. But DPH does not report numbers on DDS long-term care facilities, including the group homes and developmental centers.
Even though the administration’s COVID-19 Command Center has begun putting out information that includes DDS facilities, the numbers for those DDS facilities are not broken out from the totals.
For instance, a Command Center report stated that as of April 19, 3,743 tests were done at 206 group homes and “care sites” involving 2,297 clients and 1,146 staff among facilities funded by DDS, DPH, the Department of Children and Families, and the Department of Mental Health. That information is potentially of limited value unless it were to show a breakdown of the numbers in the facilities for each of those agencies.
As we have noted to legislators and policymakers, the families and guardians of close to 10,000 DDS residential clients are still largely being left in the dark because so little information about their loved ones is forthcoming from the administration.
We have contacted the chairs of the Legislature’s Children, Families, and Persons with Disabilities Committee and asked them, among others, to follow up with the administration to urge improvements in these DDS testing and reporting practices.
Administration withholding information on COVID-19 conditions in DDS system
Even as the Baker administration reports daily on COVID-19 infection rates among most of the population in Massachusetts, numbers of infected persons with intellectual and developmental disabilities appear to be being kept under wraps.
Information is coming out sporadically and anecdotally from the media and individuals on the ground.
The Boston Globe and other outlets reported this week that as of Tuesday, 276 people in Department of Developmental Services (DDS) residential settings statewide had tested positive as had 321 staff. Nine people receiving services from DDS had died from COVID-19.
Among the anecdotal information we’re getting:
- While testing was completed last Sunday of residents at the Wrentham and Hogan Developmental Centers, the staff at Wrentham apparently did not get tested, as the administration had reported. DDS Commissioner Jane Ryder said late yesterday that testing of the Wrentham staff will now take place this weekend.
- WCVB reported yesterday (April 17) that 40% of residents in three units at the Hogan Center had tested positive for the virus, according to the Massachusetts Nurses Association. The union said that 44 residents and 55 staff members have also tested positive.
While the Department of Public Health (DPH) provides daily updates on deaths and infections due to COVID-19 throughout the state, information has only been provided sporadically by the administration, and on a selective basis to the media, about the situation in the DDS system.
The number of deaths and COVID-19 positive cases in the DDS system appears to be rarely if ever mentioned in press briefings held by Governor Charlie Baker and Health and Human Services Secretary Marylou Sudders.
This raises a question whether the administration is placing a lower priority on protecting the DDS population from the virus than it is placing on other long-term care populations such as the elderly and even chronically ill.
Joe Corrigan, a COFAR member and member of the Wrentham Center Board, expressed his frustration in an email yesterday to Sudders and and DDS Commissioner Jane Ryder. He wrote,
Tell us where the decisions are being made. Tell us what the tipping point is for getting real and complete attention to (the Wrentham Developmental Center) and all DDS. Tell us where our loved ones stand in the pecking order vs. the poor souls at soldiers homes, nursing homes.
COFAR has requested information on numerous occasions on testing results in the DDS system from Sudders and Ryder, and has gotten only limited answers and often no response. We were forced on Thursday to file a Public Records Law request with EOHHS, DDS, and DPH for records on the timeline for testing in the DDS and DPH systems.
Staff not tested at Wrentham Center
As we reported on Wednesday, the administration has engaged Fallon Ambulance Service, a private company, to carry out the testing throughout the DDS group home system and apparently in the state-run developmental centers.
However, contrary to reports from the administration, testing of staff has apparently still has not occurred at the Wrentham Center. The administration had reported that all residents and staff in the Hogan and Wrentham Centers had been tested last Sunday.
Earlier this week, a Wrentham staff member told COFAR Executive Director Colleen M. Lutkevich that, “at this time only the residents (at Wrentham) were tested.” The staff member added in an email that direct care staff were “doing a wonderful job of taking care of the residents at this time, but the reality is they are also the ones that will be bringing the virus in. There have been several residents that have tested positive, but there still has not been any testing of the staff.”
Yesterday, a DDS official told Lutkevich that Fallon Ambulance said they “would work with us to come back to Wrentham to test the staff there,” but that he had “no specifics on when they may schedule us.” Late yesterday, however, Ryder informed Lutkevich that the testing would take place this weekend.
In his email to Sudders and Ryder, Corrigan pointed to the continued lack of testing of staff at the Wrentham Center as a critical problem:
I have no doubt that (administrators and staff at the Wrentham Center) are doing much with little in terms of distancing, etc. but please tell me what is the sense of testing residents without testing the staff who come and go daily and have to be the ones who brought in the virus to the already affected and, no doubt, growing number of victims.
Crisis highlights problem with privatized care
The testing problems are potentially compounded in the DDS group home system. Some 8,800 residents are dispersed around the state in more than 2,000 group homes, most of which are operated by corporate nonprofit providers to DDS. We are estimating that there are some 14,000 to 15,000 direct-care staff serving those residents. All of those people have become potential or actual targets of the virus.
No information has so far been forthcoming from the administration on how long the Fallon testing program will take in the group homes. Fallon is reportedly capable of testing between 500 and 1,000 individuals per day. We are already hearing anecdotal reports about delays in scheduled testing by Fallon in some group homes.
Fallon is facing the prospect of having to test at least 22,000 residents and staff in the residences. That apparently doesn’t count the clinicians, physical and occupational therapists, nurses and others who may still be visiting those homes and might not be there when the testing is being done in a particular home. We also have no information on testing plans for staff that is not working the shifts at the time of the mobile testers are there.
Group home model presents logistical problems
The COVID-19 crisis appears to show how potentially poorly the privatized care model is at protecting people during pandemics. DDS was reportedly able to test all residents and staff in the state run developmental centers in one day, with the apparent exception, however, of staff at the Wrentham Center.
Due to the highly decentralized nature of the privatized group home system, it is probably impossible to do the necessary testing within a relatively short time frame unless the administration was to call in the National Guard or another source of large-scale assistance. This raises the question whether the administration considered that, and if so, why they rejected it with respect to the DDS system, but have adopted it for the DPH nursing homes.
It further appears that within the privatized community-based system, highly compensated executives should have been doing strategic planning for the potential occurrence of a pandemic such as this one, and apparently did not do that planning.
A single testing site for group homes might make more sense
COFAR President Thomas Frain suggested that given the wide dispersal of group homes around the state, it might make more sense to test all group home residents at one site such as Gillette Stadium in Foxborough.
Frain suggested that if testing at a site such as Gillette were made available and each group home took just one resident per day to the site for testing, all residents and direct-care staff could potentially be tested in as little as 10 days. That is based on Frain’s calculation that there are some 2,500 group homes in total, containing some 25,000 residents and staff.
“Instead of ambulances traversing the commonwealth, they could have put all of those ambulance people at a single testing site swabbing people,” Frain said. Some people who could not be transported, would have to be tested at their residences, and Fallon could do that.
In the final analysis, we think a quote from the late U.S. District Court Judge Joseph L. Tauro is unfortunately highly relevant to the situation today. Judge Tauro wrote:
The (intellectually disabled) have no potent political constituency. They must rely on the good will of those of us more fortunate than they, and the constitution…
DDS plans to test everyone in the system for COVID-19, but timeline still unclear
The Department of Developmental Services (DDS) intends to test residents in all group homes in the state for COVID-19, DDS Commissioner Jane Ryder and other department officials told COFAR yesterday.
In a conference call, Ryder and other officials described a broad testing program that has already been completed in the state’s two developmental centers. As of this past Friday, the mobile testing program began in both state and corporate provider-operated group homes across the commonwealth.
Ryder said the group home testing program is being carried out by Fallon Ambulance Service in partnership with MassHealth. The ambulance service, which employs a team of testers, is based in Quincy, but operates across the state.
Ryder said residents and staff will be “prioritized” for testing if they exhibit flu-like symptoms. COFAR has raised questions about that policy and has called for immediate testing of all residents whether they are symptomatic or not.
Company will test in thousands of group homes in Massachusetts
There are 2,100 provider-run group homes dispersed around the state in Massachusetts, housing more than 7,800 residents, according to DDS. There are another 1,066 residents of state-operated group homes. During Tuesday’s conference call, the DDS officials did not offer a timeline for completing the tests, which are also intended to include staff in the residences.
Given that National Guard personnel are currently being used to test residents in nursing homes and other long-term care facilities in the state, COFAR has suggested that the National Guard might also be deployed to speed up the testing process in DDS group homes.
The testing consists of the use of nasopharyngeal swabs, which are considered the most reliable type of test. Results take from 24 to 72 hours to obtain, Ryder said.
We asked how many mobile testers Fallon Ambulance currently has and how quickly the testing can actually be done. No one answered that question during Tuesday’s conference call, although Ryder told a COFAR Board member in an email on Monday that “Fallon (Ambulance Service) has the ability to perform between 500 to 1,000 test per day.”
COFAR Board President Thomas Frain said an official with Fallon told him that given that the ambulance company is facing the prospect of testing close to 9,000 residents in both the state-run and provider-run group homes as well as an undetermined number of staff in those facilities, the testing was a “long-term” project.
DDS General Counsel Marianne Meacham said guardians can also arrange to have residents tested by their primary care doctors, and that the mobile testing program is seen as an addition to that.
DDS Chief of Staff Chris Thompson added that guardians and family can obtain “telemedical appointments” with MassHealth to discuss symptoms. They should go to www.buoy.com/mass
Questions about prioritizing residents for testing
COFAR has questioned the DDS policy of testing group home residents showing flu-like symptoms before testing anyone else. Frain maintained that research shows asymptomatic residents can be just as likely to transmit the virus as those exhibiting symptoms.
Frain noted an NPR report this week concerning a nursing home in King County, Washington in which a third of the 82 residents tested positive for the coronavirus in mid-March. Half of those were free of fever, malaise and coughing when they were swabbed for the virus, though most went on to develop symptoms. The coronavirus “spread rapidly through the facility just two weeks after it was introduced by a health care provider, despite the nursing home’s policy of isolating residents with signs of COVID-19.”
Information on test results
In Tuesday’s conference call, we reiterated our call on DDS to publicly report infection rates of persons in the DDS system, and asked about getting periodic reports on the results of the mobile testing. Meacham said DDS will provide COFAR with testing numbers when the Department has data “from at least a full week so that we have a sense of the progress of testing our community.”
Alternative sites for relocated residents
Ryder said that for those residents who are symptomatic and need to be relocated from their residences, DDS has identified three sites at the Wrentham and Hogan Centers and at the former Templeton Developmental Center where there are spaces that can be used to quarantine individuals. Ryder said these are not planned to be medical facilities.
New COVID-19 guidance document for providers
Thompson also outlined highlights of a “comprehensive” residential program guidance document just issued and shared with providers. The 16-page document updates the EOHHS guidance document of March 25. There is also a one-page summary document for all group home managers and staff.
Highlights include:
- A requirement that all staff wear face masks during shifts. Those should be surgical masks when possible or else cloth masks that comply with CDC guidelines. In emergencies, providers can ask for personal protective equipment from the Massachusetts Emergency Management Agency (MEMA).
- Staff will have their temperature taken prior to entering any residence. Anyone with a temperature of 100.4 or higher will not be allowed to enter.
- Staff who test positive but show no symptoms will be restricted from working for at least 7 days. If they do have symptoms, they must stay away from work for at 3 days after they have recovered and at least 7 days after the first symptoms appeared.
- If a resident shows symptoms or tests positive, the decision whether to provide on-site care or move the person to another location will be made on a case-by-case basis after consulting the local board of health. The family or guardian would have to be notified of any decision to relocate someone. (See discussion above about alternative sites at Wrentham, Hogan, and Templeton.)
Meacham provided the following links to the Department’s new guidance document and to its updated COVID-19 information on its website:
- DDS Residential Program Guidance: https://www.mass.gov/doc/dds-residential-program-guidance-dds-updated-april-13/download
- DDS One Page Guidance for Group Home Staff: https://www.mass.gov/doc/dds-one-page-guidance-for-group-home-staff-dds-april-13/download
- Coronavirus Update for DDS Individuals and Families: https://www.mass.gov/news/coronavirus-update-for-individuals-and-families-april-14
Please stay tuned for further information as we get it from DDS and other sources, including the promised test results.
