Archive
Critically needed federal stimulus money still hasn’t come through for DDS residential providers facing staffing shortages
Shannon Guenette still hasn’t seen any of the money even though Congress and the Biden administration released $8.7 billion in federal stimulus funds to Massachusetts last March.
“We’ve received some guidance (from the state regarding the funding), but we haven’t received any additional funds,” Guenette, executive director of Almadan, Inc., said five days prior to Thanksgiving. Almadan is a group home provider in the western part of the state to the Department of Developmental Services (DDS).
In August, Guenette told us her agency and other DDS providers throughout the state desperately needed the additional federal funding to retain workers in light of a worsening shortage of direct-care and clinical staff.
The Baker administration in Massachusetts has targeted hundreds of millions of dollars of the federal American Rescue Plan Act (ARPA) funding for human services workforce retention and recruitment.
But the state Legislature took months to come up with its own plans for distributing the funding after at least one legislative leader said they didn’t see a need for hurry.
Earlier this month, state legislators went home for their Thanksgiving recess without having reconciled Senate and House bills (S.2564 and H.4234) that specify differing distribution plans for the money.
Meanwhile, other than noting there will be three rounds of ARPA funding distribution, the administration itself has provided little clear information about the details of its distribution plan such as how many workers and which agencies would receive the money, and how much of that funding would go toward higher wages.
Under the administration’s plan, the first round of funding was supposed to augment provider rates by 10% from last July through December of this year. But, as noted, no money has reportedly been distributed for residential programs.
Repeated queries by COFAR to DDS Commissioner Jane Ryder and to Health and Human Services Secretary Marylou Sudders about the DDS staffing shortage and how to address it have gone unanswered.
Even when the ARPA money is finally distributed, we are concerned about a potentially low limit set on the amount of funding per worker under the Senate and House bills. Also of concern is a lack of clear oversight of the distribution of the funding.
And it appears at least some of the funding is intended to be used to move residents out of the state’s two remaining developmental centers and into the already overburdened privatized group home system.
A $2,000 limit per worker
Language in both the Senate and House bills would limit funding for higher wages to $2,000 per worker. It’s not clear how effective such a payment would be in recruiting and retaining workers, particularly if it is only a one-time payment.
The Senate bill would also establish an advisory panel to make recommendations to the administration regarding the “Essential Employee Premium Pay Program.” The panel’s report is due with its recommendations by March 31, 2022.
The advisory panel sounds like a potential recipe for further delay without necessarily providing a structure for ensuring that the funding goes to the workers.
The distribution of funding to workers may not have sufficient oversight
Information posted online by the administration requires DDS providers to attest or essentially promise that 90% of the additional ARPA funding they receive will be used for “compensation for their direct-care workforce.” That could include, “among other things,” hiring and retention bonuses.
While the providers will be required to submit spending reports, it isn’t clear that the administration has dedicated sufficient resources to auditing such reports and ensuring that the money is going in all cases to front-line staff.
State Auditor Suzanne Bump’s office reported in 2019 that increases in state funding to DDS and other providers resulted in surplus revenues for the providers, but that those additional revenues led to minimal increases in wages for direct-care workers.
According to Bump’s audit, while the increased state funding was at least partly intended to boost direct-care wages, it “likely did not have any material effect on improving the financial well-being of these direct-care workers.”
Some ARPA funding may be used to “divert” residents from developmental centers
According to the administration’s distribution plan, at least $44 million of the ARPA funding will be used starting in Round 2 to “divert” clients “towards community living … and away from facility-based settings.”
We are concerned that while at least some of this funding would reportedly be used to prevent the inappropriate placement of DDS clients in hospitals or nursing homes, a portion of the funding may be used to further reduce the population of facilities such as the Wrentham and Hogan developmental centers. As such, this funding would only further reduce choices in residential care for DDS clients.
The residential population at both Wrentham and Hogan have been declining in recent years, and admissions to both facilities were zero in 2020.
Providers cite need for funding and higher pay for direct-care workers
In September, a provider-based “Collaborative” provided written testimony to the state Legislature’s Ways and Means Committee chairs seeking $174 million per year for five years in ARPA funding for human services organizations. The money was being sought “to provide recruitment and retention incentives to workers to help combat the workforce crisis in the sector.”
The Provider Collaborative testimony said the $174 million would affect about 34,800 staff earning less than $60,000, and nurses and clinicians earning less than $90,000.
The Collaborative noted that low wages paid to direct-care workers are a problem. “The low rates of pay for direct-care staff… coupled with complex, difficult jobs have led providers to struggle with recruiting and retaining workers even before the COVID-19 pandemic impacted programs,” the testimony stated.
The Collaborative blamed those low wages on the state’s “rate-setting process.” We think, however, that many providers, as the state auditor noted, could afford to pay more to their workers.
Shannon Guenette told us that Almadan is currently only able to pay its staff $15.25 an hour. The Collaborative stated that the median salary for direct-care workers is $16.79 an hour. According to the Collaborative, the MIT Living Wage calculator notes a living wage for a single person in the area is $17.74 an hour.
All of this points to the need for quick action to distribute the ARPA funding. It’s unfortunate that legislative leaders don’t appear to recognize that there is, and has been, a need for hurry. There is also a need for effective oversight of the funding to make sure it gets to those workers.
DDS state-operated group homes facing a staffing and possible closure crisis
State-operated group homes for persons in Massachusetts with developmental disabilities appear to be facing a perfect storm of staffing shortages, potentially unvaccinated staff, and a possible departmental effort to shut at least some of the residences down.
The staffing shortages are also affecting the much larger network in the state of corporate provider-operated group homes funded by the Department of Developmental Services (DDS). But we are increasingly concerned that the critically important state-run DDS group home network could be facing a crisis that could threaten its long-term existence.
We often advise families whose loved ones are experiencing poor care in provider-run residences to ask for placements in available state-run group homes. Staff in the state-run network generally receive higher pay and benefits and more training than their counterparts in the provider system.
Resident moved without notice
This week, we received a report that a state-run group home in western Massachusetts was being closed and that at least one of the residents was moved without written notice as of Thursday (October 21) to a location in another town.
Earlier this month and this week, we received reports from a COFAR member that up to seven state-run homes in the southeastern region of the state had been closed because staff in them had not been vaccinated for COVID-19.
We have not been able to confirm those reports about closures of homes in southeastern Massachusetts. A DDS official privately told a COFAR member that no state-operated group homes had yet been closed in the region as of mid-October, but that some closures could happen after October 17. The official referred to the possibility of “temporary consolidations” of group homes around the state.
In August, Governor Baker issued an executive order requiring all state employees to be vaccinated by October 17 or ultimately be terminated. While the executive order apparently applies to staff in state-operated group homes and the Wrentham and Hogan Developmental Centers, the separate provider-operated DDS group home system is apparently not subject to the vaccination mandate.
It is not clear how many staff in the DDS group home system remain unvaccinated. As of last April, the last time EOHHS apparently tracked staff vaccinations, less than 50% of staff in state-operated DDS group homes were fully vaccinated, and only 51% of staff in provider-run group homes were fully vaccinated.
Administration officials not commenting
On October 14, we emailed DDS Commissioner Jane Ryder and the press office at the Executive Office of Health and Human Services (EOHHS) with questions about the reports of closures and consolidations in the state-operated group home network.
To date, Ryder has not responded to our query. A spokesperson for EOHHS said we would have to file a Public Records Request for that information. On October 15, we filed a Public Records Request, and EOHHS responded that same day that that agency did not have any records relevant to our query.
DDS regulations may be violated by sudden closures
Under DDS regulations (115 CMR 6.63), DDS clients cannot be transferred without a 45-day notice and the opportunity for a hearing unless the the Department determines that the transfer is “an emergency involving a serious or immediate threat to the health or safety of the individual or others.”
Western Mass DDS staff urge Ryder to address staffing shortages
Meanwhile, on Wednesday (October 20), the Massachusetts Nurses Association, a union that represents nurses in the DDS system as well as hospitals around the state, reported that several DDS employees in western Massachusetts had sent a letter in late September to Commissioner Ryder “imploring her to intervene in a growing patient-care crisis that is unfolding in many of the region’s DDS group homes.”
The letter stated that staffing shortages in both state-operated and provider-operated group homes were causing “significant increases” in client injuries requiring emergency room treatment, and in the placement of untrained staff in homes.
The MNA letter said some staff were being forced to work overtime due to staffing vacancies, and that one staff worker was reportedly required to work 48 hours straight.
The MNA letter to Ryder was dated September 21. The union said that as of October 20, Ryder had not responded.
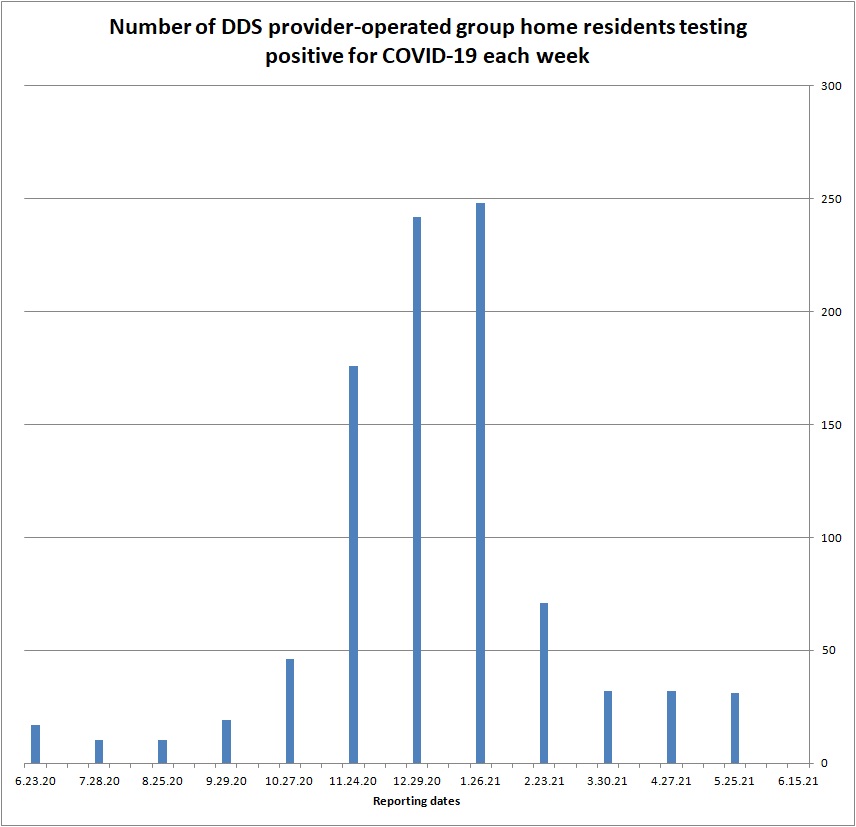
COVID rates in the DDS group home system continuing to climb slowly
In the midst of the continuing staffing and apparent vaccination problems, the latest online COVID testing report from EOHHS shows a slow, but continuing increase in individuals testing positive in DDS state and provider-run group homes. In state-operated group homes, the number of residents testing positive rose from 3 to 6.
Among staff in the state-operated group homes, the number of those testing positive rose from 11 to 12 between September 7 and October 5.
In provider-run homes, the number of residents testing positive jumped from 31 in September to 49 in early October. The administration, however, does not report the number of staff testing positive in the DDS provider-run system.
Census in state-ops and ICFs declining
Whether or not there are plans to close state-operated group homes or the Wrentham or Hogan Developmental Centers, the administration has nevertheless been letting the residential populations or census drop in these facilities. In addition, funding for these facilities has dropped or has remained flat for years. (See here and here.)
Documents provided by DDS on September 21 in response to a Public Records Request for records on the number of admissions to state-operated group homes, confirm that the census in those facilities has been declining since Fiscal Year 2015. We previously received information from DDS showing a decline in the census and virtually zero admissions in 2019 and 2020 at the Wrentham and Hogan Centers.
The census in DDS provider-operated group homes grew by an average of 124 residents per year between Fiscal Years 2008 and 2021. However, the census in state-operated group homes grew by an average of only 3 residents per year.
Moreover, since Fiscal 2015, the census in state-operated group homes has actually dropped by an average of 18 residents per year while the census in provider-operated group homes has continued to grow by an average of 83 residents per year. The number of residents in state-run group homes was almost 10% lower in Fiscal 2021 than in 2015.
The data show there have been admissions each year to the state-operated homes. But those admissions have apparently been more than offset by deaths in those residences.
Future is concerning
In sum, all of these numbers and trends are concerning, as is the administration’s policy not to respond to questions either from us or from unions such as the Mass. Nurses Association.
We may learn a little more if DDS does provide records relevant to our Public Records Request concerning the reported state-operated group home closures. But in the meantime, we are left to wonder what the administration is planning to do – or is actually doing — to address the staffing shortages in the DDS system.
At the very least, we hope the administration doesn’t view the staffing shortages and the problem of unvaccinated staff as opportunities to further downsize the state-operated group home system.
Baker administration leaves DDS staff out of COVID vaccination requirement
[UPDATE: We have received unofficial information that staff of DDS state-operated group homes and at the Wrentham and Hogan Developmental Centers are subject to the vaccine mandate. It appears those staff fall under an executive order last month applying to executive branch employees.
However, the much larger corporate provider-operated group home system does not appear to be subject to the vaccine mandate.
This new information contradicts what an EOHHS spokesperson told us (see post below), which was that no congregate care staff are subject to the vaccine mandate.]
Despite a recent uptick in the number of residents in the Department of Developmental Services (DDS) system who have tested positive for COVID, the Baker administration is not including DDS system staff in a new requirement that health care workers in Massachusetts be vaccinated.
Once again, it appears, people with intellectual and developmental disabilities are subject to looser COVID protections than are the elderly or people with other types of disabilities.
According to the State House New Service, the Baker administration this month announced plans to require COVID-19 vaccinations for all staff at rest homes, assisted living residences, hospice programs, and for home care workers providing in-home, direct care services.
The administration first imposed a vaccine requirement in August on employees of skilled nursing facilities.
Last week, a spokesperson for the Executive Office of Health and Human Services (EOHHS) told COFAR that the latest vaccine mandate does not include “congregate care” staff. We had specifically asked whether the mandate includes DDS-funded group homes, developmental centers, and day programs for persons with intellectual and developmental disabilities.
Although the EOHHS spokesperson didn’t directly answer our question, DDS congregate care facilities would appear to consist of both provider-run and state-operated group homes, which together serve some 9,000 residents and employ tens of thousands of staff. [See updated information above pertaining to state-operated group homes and the developmental centers.]
The EOHHS spokesperson also did not respond to our follow-up question why DDS staff have not been included included in the vaccine mandate. DDS Commissioner Jane Ryder did not respond to an initial inquiry on the matter that we sent her on September 8.
We have raised concerns for several months about unvaccinated staff in the DDS system. It is not clear how many DDS system staff remain unvaccinated.
As of last April, the last time EOHHS apparently tracked staff vaccinations, less than 50% of staff in state-operated DDS group homes were fully vaccinated, and only 51% of staff in provider-run grop homes were fully vaccinated.
Apparent concern over staffing shortage in the DDS system
Given the lack of information or comment from the administration, we are guessing the lack of a vaccine mandate for DDS is due to a staffing shortage, which may be more acute in the DDS system than in nursing homes. It would appear the administration is concerned that requring those staff to be vaccinated would make the shortage worse.
Home care providers in Massachusetts, in fact, are already predicting the vaccine mandate will drive many of those workers to other fields.
One solution, of course, would be to pay direct care workers on the DDS system enough to retain the current workforce and recruit new caregivers. As we’ve reported, federal and state funding exists to do this. But there appears to be no sense of urgency in the state Legislature to distribute the funding, and no effort there to ensure the money will go toward those workers.
Rising number of infected residents
As the State House News Service reported last week, despite the fact that more than 4.54 million people in Massachusetts are now fully vaccinated, COVID continues to spread, apparently driven by the more infectious Delta variant.
The last two online COVID testing reports from EOHHS for congregate care facilities show an increase in residents testing positive in DDS provider-run group homes.
After declining dramatically from a high of almost 250 positive residents in January of this year to virtually zero in June and early July, there were 31 residents listed as positive in provider-run group homes as of this past week’s report (Sept. 7).
The positive COVID rate among provider-run group home residents in the DDS system had started to rise as of the August 10 EOHHS report.
EOHHS reports on COVID rates in DDS and other congregate care facilities are now provided once a month. EOHHS does not report specifically on the number of COVID-positive staff in provider-run group homes.
Importance of vaccinations of staff emphasized
The State House News Service quoted Tara Gregorio, president of the Massachusetts Senior Care Association, as stating that the administration’s vaccine mandates “will create parity, transparency, and accountability within the entire health care system, which is ultimately to the benefit of consumers and their caregivers.”
But parity, in particular, will not fully be achieved throughout the entire health and human services system if DDS staff are left out of the vaccine mandates. DDS manages a budget of more than $2 billion — the largest budget of any line agency in the EOHHS system.
We hope it finally begins to dawn on both legislators and the administration that DDS needs to be included in the staff vaccination mandates, and that those workers need to be paid enough to keep them from leaving the system.
As COVID rates drop, DDS finally lifts restrictions on visiting group homes
With numbers continuing to drop of residents testing positive for COVID-19 in the Department of Developmental Services (DDS) system, DDS has finally lifted restrictions on visitation, according to an announcement on the Department’s website.
In the announcement, dated June 14, DDS Commissioner Jane Ryder stated that DDS had “asked our residential settings to return to their pre-pandemic visitation policies and practices” with the following exceptions:
- Continued screening of all visitors for symptoms of illness and COVID-19 infection.
- Suspended visitation when a resident is isolating due to COVID infection or there is a COVID-19 outbreak at the program.
- Visitors must wear masks indoors at the home except if fully vaccinated and visiting a fully vaccinated resident in their room. Staff are still required to wear masks in group homes, regardless of vaccination status.
- Residents who are fully vaccinated may visit with loved ones who are fully vaccinated without maintaining social distancing or wearing masks, if they choose.
The relaxed visitation guidelines hopefully mean the end of the imposition of contradictory and seemingly arbitrary restrictions, in some cases, on visitation by families of loved ones in the DDS system.
Ryder’s statement came just as the most recent COVID testing data published online, on June 15, showed that positive cases have reached new lows in the DDS system.
For the first time since COVID testing data has been kept, there were zero positive cases among residents in provider-run DDS group homes, and less than 5 residents testing positive in state-run group homes. (See graph below for the testing trend for provider-run residents since June 2020.)
Source: EOHHS online data
In the weeks prior to June 15, the number of residents testing positive in the provider-run homes had held steady at close to 30, while the number testing positive in the state-run group homes had held steady at about 10.
It remains to be seen whether the lower positive rates as of June 15 will continue. The answer to that question will apparently not be known publicly until July 13, when the next results will be published.
As of June 16, the Executive Office of Health and Human Services (EOHHS) indicated on its COVID reporting site that DDS testing data will be published only every four weeks instead of weekly, as had previously been the case during the COVID crisis.
It is still unclear how many staff in provider-run group homes in the DDS system are continuing to test positive for COVID. That information has never been included in the DDS facilities reports.
The latest report as of June 15 shows less than 5 COVID-positive staff in the state-operated group homes, and zero positive staff and zero positive residents in the Wrentham and Hogan developmental centers.
Staff vaccination rates still unclear
COVID vaccination rates among staff and residents in the DDS system are also not published online.
Based on information provided by EOHHS in response to Public Records Requests from COFAR, we last reported that as of April 9, less than 50% of staff in state-operated group homes were fully vaccinated. In provider-run group homes, only 51% of staff were fully vaccinated as of April 12.
Some 75% and 90% of residents in provider-run and state-run group homes respectively had been vaccinated as of April 12.
We filed a renewed Public Records request on Monday (June 28) with EOHHS for the latest staff and resident vaccination rates. EOHHS stated that a response will be provided by July 13.
As we have previously noted, the relatively low staff vaccination rates as of April may have been keeping COVID present in the DDS system. However, if COVID rates among residents do remain at zero or close to it in the weeks following June 15, it would almost certainly be due to a high vaccination rate among those residents.
Ryder continuing to push vaccinations for residents
In her June 14 message, however, Commissioner Ryder implied that not all DDS clients have been vaccinated. She noted that a “Homebound Vaccination Program” was available across the state to anyone with trouble getting to a vaccination site. The number is 1-833-983-0485 to schedule an in-home vaccination.
Restarting day programs
Ryder also said DDS was working with providers to return clients to in-person day and employment programs. She said, however, that those programs are currently “struggling” with staff shortages.
We have reported that day programs were also targeted for major cuts in the governor’s Fiscal Year 2022 state budget. The fiscal year began Thursday (July 1), but the budget has not yet been approved by the Legislature.
Ryder did not mention in her message that in January, Governor Baker specified a $25 million, or 11%, cut in the DDS Community Based Day and Work (CBDW) line item. A major cut in the line item could also make it difficult to return clients to in-person day programs.
The House and Senate subsequently added $15 million back to the CBDW line item, noting that the add-back would primarily be for the development of services in response to the COVID pandemic. But even the House and Senate versions would cut the line item by $10 million, or 4.2%, from the previous fiscal year.
We have previously reported that the COVID crisis resulted in a major shift to remote attendance in the CBDW programs via platforms such as Zoom. As of November 2020, 36% of day program clients were attending remotely only, according to DDS data.
As usual, it would be helpful to have more timely information from the administration about the state of the DDS system, particularly regarding COVID vaccination and testing rates for provider staff. The outlook for DDS day programs also remains cloudy as we emerge from the pandemic.
At the same time, the dropping positive COVID rates among DDS group home and facility residents, and the promised return to pre-pandemic visitation policies are very hopeful developments.
Families still restricted in visiting loved ones in DDS system even if residents have been vaccinated
Throughout the COVID-19 pandemic, we have questioned overly restrictive and sometimes contradictory family visitation policies imposed by both the Department of Developmental Services (DDS) and its residential providers.
What seems surprising is that now, with most residents in the system apparently having been vaccinated, those restrictive and contradictory policies appear to be continuing.
In response to a query sent to our members last week, several said they were continuing to be sharply restricted or even prohibited entirely from entering group homes in which their loved ones are living. Some of those family members are nevertheless allowed to take the residents home for visits.
As we have reported, while most residents of group homes and developmental centers in the DDS system appear to have been vaccinated, a significant percentage of staff have not been. Yet, the restrictions on visitation or contact appear to be aimed exclusively at family members and guardians of residents.
“To hold families and guardians to a higher standard than direct care is unfair and makes no sense,” said Thomas J. Frain, COFAR Board president. “Family visits at this time should not be any more restrictive than they were before the crisis. But some residential managers are clearly using COVID restrictions as a weapon to control family access to their loved ones.”
In an email sent Monday (May 17) to DDS Commissioner Jane Ryder, I asked why visitation restrictions were still ongoing in residences in which all residents have been vaccinated. Ryder, to date, has not responded.
DDS visitation guidance, dated March 19 of this year, continues to give providers discretion to limit the number of visitors and restrict visits under any circumstances the providers deem pose a threat to safety. The guidance document states that any such restrictions should not be arbitrary.
While the March guidance does allow visitors who are fully vaccinated to meet with vaccinated residents in their rooms, it states that providers must restrict all visitation if any staff are infected or presumed infected within the past 14 days. It apparently doesn’t matter under the policy whether all residents have been vaccinated or not.
Family members and guardians cite arbitrary restrictions
A number of other COFAR members said this past week that they have been subjected to differing and sometimes seemingly arbitrary restrictions on visitation.
Colleen Lutkevich, COFAR executive director, said all residents in her sister’s house on the Wrentham Developmental Center campus have been quarantined from May 11 through May 21 because two staff tested positive for COVID. Yet, all residents have been vaccinated, she said, and none are currently testing positive.
Frain said he, himself, was subjected to what appeared to be an arbitrary restriction by staff after his brother experienced a medical emergency in his group home in March. Frain had entered the residence along with ambulance personnel to attend to his brother.
When the emergency was over, Frain said, he was singled out by two staff members and told he alone must leave by the back door of the residence because he hadn’t been tested on entering for COVID. Frain said he complied with the order, but feels it was unnecessary and was possibly an effort to personally humiliate him as a family member.
One COFAR member said that even though her son has been vaccinated — and she believes all other residents of his group home have been vaccinated as well — she and her husband have not been allowed to enter the residence. Nevertheless, she said, they are allowed to take their son home for overnight visits.
“It makes no sense,” the COFAR member wrote in an email. “At least we can be with him, so I really can’t complain, but it would be nice to see what is going on in the house.”
As is the case with a number of families, the COFAR member said she needs to go through her son’s clothes for the seasonal change to spring. Because of the no-entry restriction, the staff brought his belongings to the backyard. “I cannot bend over,” she wrote, “so it was difficult.”
Yet we were told that in another group home even unvaccinated family members were allowed inside to their loved-one’s bedroom to change his wardrobe to spring.
Another COFAR member, who wanted to change her son’s clothing from winter to spring, said she is currently allowed to enter the residence once a week. She too can take her son home at any time.
Another provider requires a week’s notice prior to visits by family members. In yet another case, visitors are allowed in the house, but only for a maximum of 30 minutes.
COVID infection rates not correlated with restrictions on family visits
State data show the rate of COVID infection in the DDS system among both residents and staff declined earlier this year, reaching lows at the end of March. But since then, as recent weekly online state facility reports show, the decline has stalled, and rates of infection have held steady.
As of May 11, 10 residents and 14 staff in the state-operated group home system continued to test positive for COVID. As of that date, 37 residents in provider-run group homes and an unreported number of staff continued to test positive.
There were as many as 5 deaths among residents in the group home system due to COVID in the seven days prior to May 11. No data on COVID-related deaths are available for staff.
While administration officials have not responded to our requests for comment on the matter, we think the decline in the COVID rate in the DDS system from January through March was largely due to the vaccinations of most of the residents and at least some staff, which began in January.
Although data is lacking, we think the continuing presence of at least some COVID in the system since the end of March may be due to the apparent continuing resistance of a significant number of staff to getting the vaccine.
As far as we can tell, residential DDS providers have continued to impose the same types of restrictions on family visits that they imposed prior to the first vaccinations in January. So, we don’t see that those restrictions as related to the decline in COVID rates since January or to the continuing presence of infection in the system.
It’s time, as Tom Frain said, for DDS to issue new, unambiguous guidance to providers to restore visitation policies to what they were prior to the pandemic.
State House approves cuts to DDS day program funding, increases for provider group homes
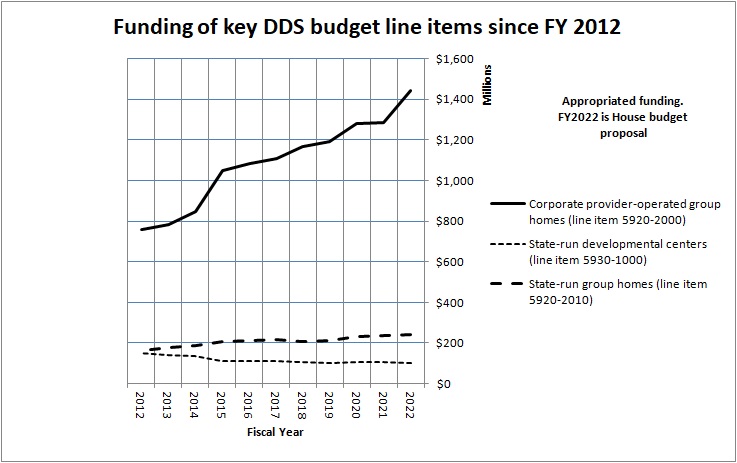
The House budget would add $100,000 to the governor’s proposed Fiscal 2022 funding for state-operated group homes (line item 5920-2010). However, when adjusted for inflation, even the House budget proposal would amount to a cut in funding for this line item of somewhat less than 1%. (We are basing that assessment on numbers from the Massachusetts Budget and Policy Center’s “Budget Browser.”)
The two remaining developmental centers would similarly see their funding cut in Fiscal Year 2022 by $2.1 million under the House budget, when adjusted for inflation (line item 5930-1000). Since Fiscal 2012, funding for the developmental center line item will have been cut by 32%.
COFAR is continuing to raise concerns regarding the ongoing under-funding of state-run DDS programs. We believe this has led to unchecked privatization of programs and services.
We are also concerned that even within provider accounts, we may be seeing a permanent pullback in funding for day programming, with much of that funding ultimately going to provider-run group homes.
Last month, we sent an issue paper raising those concerns, among others, to Senator Adam Gomez and Representative Michael Finn, the new chairs of the Legislature’s Children, Families, and Persons with Disabilities committee. You can find our issue paper here.
Staff resistance to COVID vaccine may be keeping virus in DDS system
Resistance among group home staff in the Department of Developmental Services (DDS) system to getting vaccinated against COVID-19 seems to be an ongoing problem, and we’re concerned that it may be linked to the continuing presence of COVID in the system.
The latest online weekly COVID testing data for the DDS system show that while the number of infected staff and residents in the system has declined from historic highs in December and January, the rate of that decline may have stalled in the past several weeks.
The vaccination effort in the DDS system started in December.
It is concerning that as of April 9 — some four months after the vaccination program began — less than 50% of staff in state-operated group homes were fully vaccinated, according to data provided last week by the Executive Office of Health and Human Services (EOHHS). In provider-run group homes, only 51% of staff were fully vaccinated as of April 12.
The data are as of April 12 for provider-operated group homes, and as of April 9 for state-operated group homes and the state’s two developmental centers or Intermediate Care Facilities (ICFs). The data were provided to COFAR in response to a Public Records Request. EOHHS and DDS provided data for February and March in response to a previous records request.
In the ICFs, the current level of staff vaccinations appears to be higher than in the group homes, but the numbers are still somewhat concerning. Some 68% of the staff at the Wrentham Developmental Center (WDC) and 66% at the Hogan Regional Center in Danvers were fully vaccinated as of April 9.
That this apparently low level of staff vaccinations is not simply due to a slow vaccination process appears to be borne out from the data. First of all, among residents of both state and provider-run facilities, the vaccination picture looks much brighter.
Among residents in state-run group homes, some 90% were fully vaccinated as of April 9. At WDC, 99% of residents were fully vaccinated, and 91% of residents at Hogan were fully vaccinated as of April 9.
In provider-run residences, 75% of residents were fully vaccinated, although18% had not gotten their first shot as of April 12.
The graphs below illustrate the differences in numbers of persons getting vaccinated among the different settings, and differences in vaccination levels between staff and residents.

The graphs show that relatively large numbers of staff were still unvaccinated (the orange bars) in the provider and state-operated group homes, while the numbers of unvaccinated residents in all of the settings (the yellow bars) were much lower.
Data appear to show resistance by staff to vaccinations
Vaccination data regarding state-run and provider-run group homes appears to imply that there is a relatively large group of staff that are resisting getting the vaccine.
For instance, of the 1,596 staff in DDS state-run group homes who did get a first dose of the vaccine as of Feb. 16, most appear to have gone on to get their second shot as of April 9. A total of 1,728 staff in the state-run group homes were fully vaccinated as of April 9, up from 277, as of February 16.
However, 1,966 staff had still not gotten their first shot as of February 16. And the data indicate that only 279 of those staff had gotten their first dose as of April 9. That left 1,687 staff still unvaccinated in the state-run group homes as of that April date.
As a result, the number of unvaccinated staff in the state-run group home system dropped by only 7.8% between February 16 and April 9, declining from 55.2% to 47.4%.
Decline in COVID-19 in the DDS system may have stalled
As some staff have apparently continued to resist getting vaccinated, the rate of decline of COVID in the DDS system appears to have stalled.
For DDS state-operated group homes, a low in the infection rate was reached as of March 30, when 9 residents and 12 staff tested positive. That is compared to highs of 43 residents testing positive in January, and 111 staff testing positive in December.
But as of April 20, the latest date for online data, the number of COVID positive residents in the state-operated group homes was still at 9, and the number of positive staff had crept up to 14.
In the provider-operated group homes, a low of 29 positive residents was reached as of March 23. That number was up to 31 residents as of April 20. No information is made available by the administration, for unknown reasons, on the number of staff testing positive in provider-operated homes.
At the Hogan Center, no staff or residents have tested positive since February; but at WDC, as many as 5 staff tested positive as of April 13 and April 20. No exact number is given for 5 or fewer persons testing positive in a given setting. Zero residents at WDC have tested positive since January.
So it may be the case that as long as at least some staff are continuing to resist getting vaccinated, the number of staff and possibly even of residents in the DDS system who get COVID may never reach zero.
There have been no deaths in either ICF from COVID since last November. But there have continued to be as many as five deaths per week in the group homes as recently as of April 13. That lower number of deaths in the ICFs may also reflect the fact that the vaccination rate among staff and residents in the ICFs has been higher than in the group homes.
We can only speculate as to whether the administration considers it a problem that the vaccination rate among staff in the DDS system is still as low as it is. Neither Health and Human Services Secretary Mary Lou Sudders nor DDS Commissioner Jane Ryder has responded to our multiple requests for comment about the vaccination process in the DDS system.
Until and unless the Baker administration decides that the public has a right to know their thinking on this, we will have to keep guessing.
COVID-19 vaccinations appear to be working in the DDS system, but information is lacking
Data received last week from the state show that as of early March, more than 80% of residents and a little over 50% of staff in residential facilities directly run by the Department of Developmental Services (DDS) had been fully vaccinated for COVID-19.
One would assume that by now, all residents in the DDS system and most of the staff have been vaccinated. But the numbers are almost a month old, and DDS said it does not have vaccination data on residents or staff in provider-run homes.
DDS provided the vaccination numbers for the sate-run facilities on March 29 in response to a Public Records Request we had sent on February 18.
Vaccination data also provided on March 29 by the Executive Office of Health and Human Services (EOHHS) in response to the same Public Records Request does include numbers on vaccinations of residents and staff in provider-run homes. But the EOHHS data is even more out of date than the DDS data.
A spreadsheet provided by EOHHS is dated February 23. The EOHHS data showed that as of February 23, 24% of staff and 38% of residents in the DDS provider-run group home system had been fully vaccinated. EOHHS is the state’s umbrella human services agency, and DDS is located under it.
The chart below, based on the DDS data, therefore shows the most up-to-date information we have from the administration on vaccinations in the DDS system:

On April 1, I submitted a new Public Records Request to EOHHS, this time asking for current data on vaccinations in both provider-run group homes and state-run residential programs.
In addition to the lack of up-to-date vaccination data, both EOHHS and DDS said they did not have any records on numbers of staff or residents refusing vaccinations. We think the difficulty involved in getting this information on vaccinations in the system is troubling.
Since last May, the Baker administration has been posting at least some information in its online weekly state facilities reports on COVID test results of residents and at least some staff in the DDS system. But getting information on vaccinations is another story.
COVID test results continue to be promising
Those COVID test results continue to be encouraging, apparently reflecting the large numbers of residents and staff that have been vaccinated.
As of the March 30 state facilities report, residents testing positive in both state and provider-run group homes declined to some of their lowest levels since the COVID crisis began. There have been no residents or staff testing positive at either the Hogan Regional Center or the Wrentham Developmental Center since late February. There have been no deaths of any residents in either facility due to COVID since last November.
The numbers of infected residents and staff in DDS state-operated group homes and in the two developmental centers have also declined to all-time lows since the crisis began.
As of March 30, 9 residents and 12 staff in state-operated group homes tested positive, compared to highs of 43 residents testing positive in January, and 111 staff testing positive in December.
In the provider-run group home system, 32 residents tested positive as of March 30, compared to a high of 305 in January. As we have previously noted, no information is made available by the administration, for unknown reasons, on the number of staff testing positive in DDS provider-operated homes.
Administration won’t comment on the vaccinations or test results
In February, I emailed both EOHHS Secretary Mary Lou Sudders and DDS Commissioner Jane Ryder, asking for comment on whether the vaccines were responsible for the declining numbers of infected persons in the DDS system even at that early period in the vaccination effort. Neither Sudders nor Ryder ever responded. Why the administration won’t comment on this is perplexing.
Month-long delay in providing records
On February 18, I filed an initial Public Records Request with both EOHHS and DDS, asking for:
1. Records and internal emails that discuss projected timeframes for vaccinating residents and staff in DDS residential facilities; and
2. Records indicating the number of residents and staff who have been vaccinated in DDS residential facilities, broken down by type of facility.
On February 23, I additionally asked for:
3. Records indicating the number of staff and residents in the residential facilities who have refused vaccinations.
As noted, neither DDS nor EOHHS responded with any records until March 29. In its response, DDS stated that it had no internal emails discussing vaccination time frames. While EOHHS did indicate that it had such emails, the agency said it would only provide them if we were willing to pay $1,150 for search and redaction fees.
Also, as noted, both agencies said they had no records on numbers of individuals refusing vaccines.
While DDS had no internal emails on vaccine timelines, the Department stated that the administration had placed residents and staff in congregate care settings under Phase 1 of its vaccine distribution plan. Phase 1 ran from December 2020 through February 2021.
What we know now
At this point, all we can say with any degree of certainty is that most of the residents in state-run congregate care facilities in the DDS system have probably been vaccinated by now. The rest is pretty much conjecture despite our repeated efforts to get more concrete information out of the administration. Those efforts have now included filing two Public Records Requests.
In a letter, dated March 24, to the “DDS community,” Ryder maintained that the administration had heard the “voice” of that community in responding over the past year to the pandemic. “Your voice was instrumental in driving and shaping these developments. You let us know when our policies and protocols went too far – or not far enough,” she wrote.
Ryder added that, “DDS remains committed to hearing your voice, and keeping you informed and engaged as we go.”
If Commissioner Ryder is truly committed to hearing our voice and keeping the DDS community informed, she can start by providing up-to-date information on vaccine distribution in the system, and by responding to our repeated requests for her comment on these matters.
DDS numbers show pre-COVID drop in mainstream employment of DDS clients
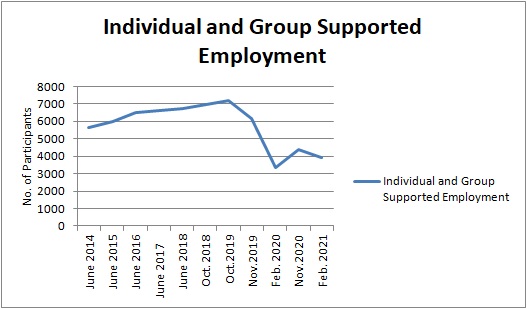
Despite continuing clams by the state that people with developmental disabilities are finding jobs and thriving in the mainstream workforce, newly provided state data show a steep drop in “supported” or “integrated employment” for those persons as of early 2020.
A comparison of the new data from the Department of Developmental Services (DDS) with data previously available from the Department reveals a 53% drop-off in “group and individual supported employment” between October 2019 and February 2020. (See graph below)
As the graph shows, the employment numbers actually rebounded a little bit as of November 2020, which was during the COVID period, but then dropped again as of February 2021.
Source: DDS
The employment numbers starting from November 2019 were provided by DDS to COFAR on March 9 in response to a Public Records Request. The previous numbers from June 2014 through October 2019 are from an online DDS December 2019 “Employment First Progress Report.”
The drop in the number of DDS clients in “individual and group supported employment” positions is prior to the COVID crisis, so COVID-19 and its impact could not be the cause.
The DDS data raise further questions about the state’s claims in closing all sheltered workshops as of 2016 that DDS clients would find better and more fulfilling work opportunities in the mainstream workforce.
Baker administration officials since 2016 have attempted to put a positive spin on the situation, with then DDS Commissioner Elin Howe maintaining that year that “there are now more people working in individual jobs in the community than ever before.” But even then, it appeared the administration was gaming the numbers.
The DDS 2019 “Employment First Progress Report” continued to try to cast mainstream employment prospects for developmentally disabled persons in the most positive light. While recognizing a “difficulty in obtaining job opportunities for individuals with more significant disabilities,” the progress report nevertheless touted:
An increase in the total number of individuals now employed, earning minimum wage or higher, and receiving the same benefits as other employees;
An increase in the number of individuals earning minimum wage or higher in small Group-Supported employment services to 71%; and
Continued evolution of Community-Based Day Support programs that support individuals on their pathway to future employment via skill-building and other meaningful activities.
But COFAR and a number of family members have pointed out that what actually occurred in the wake of the closures of the sheltered workshops was the transfer of thousands of clients to day programs where there was little or nothing for them to do. It appeared early on that the numbers of available job opportunities in “integrated” or or mainstream settings was extremely limited.
DDS does not yet appear to have published a further progress report on integrated employment since the December 2019 report.
DDS day programs continue to draw clients, but more than a third began attending remotely
As we have previously noted, the numbers of Massachusetts DDS clients placed in Community-Based Day and Work (CBDW) programs since the closures of the sheltered workshops has outpaced the number of clients who have been given integrated employment opportunities.
The newly provided data from DDS show a 22% drop in overall CBDW participation during the initial months of the COVID crisis — from February 2020 through November 2020. But the numbers began to rise after that; and as of February of this year, the number of day program participants hit an all-time high of 7,569 clients.

Source: DDS
Nevertheless, the COVID crisis resulted in a major shift to remote attendance in the day programs via platforms such as Zoom. As of November 2020, 36% of day program clients were attending remotely only, according to the March 9 DDS data. DDS did not provide figures after November 2020 on the number attending remotely.
Due to that remote attendance rate, CBDW programs are now being subjected to proposed funding cuts by Governor Baker in his Fiscal Year 2022 budget.
That is apparently further bad news for integrated employment prospects because the CBDW line item in the DDS budget is used, in part, to fund job skills training and other activities to help DDS clients make the transition to the mainstream workforce.
No response from Commissioner Ryder
On March 16, I sent an email query to DDS Commissioner Jane Ryder, asking for a comment on the apparent drop in client participation in integrated employment, and for her assessment of possible reasons for it. Ryder so far has not responded to my request.
DDS said it does not possess records relating to the future of CBDW programs
In its March 9 response to our Public Records Request, DDS stated that the Department does not possess any records concerning projections of the number of clients who will be enrolled in CBDW programs in FY22 and beyond, or concerning the number of such programs that will exist, the financial viability of such programs, or the number of clients who will attend remotely.
One question the DDS response leaves us with is whether it implies that DDS does not engage in planning regarding CBDW programming.
Need is greater than ever for work opportunities in day programs
It seems clear that the administration’s integrated employment promises for persons with developmental disabilities were not being realized even prior to the COVID crisis.
Recognizing that problem, we had supported a bill in 2019 (H.88), which would have required that meaningful work activities be provided in CBDW programs themselves. Unfortunately, the language in the bill was subsequently replaced by the Children, Families, and Persons with Disabilities Committee with language establishing yet another Commission on the Status of Persons with Disabilities.
What the latest DDS data confirms, in our view, is that the administration and Legislature need to rethink the ideology that led to the closures of the sheltered workshops, and take substantive action to provide work opportunities to people with developmental disabilities.
Records imply ‘strong’ disagreement in Baker administration last summer over mandatory COVID testing of DDS staff
Top administrators in the Baker administration appeared to strongly disagree last summer over whether to require testing of staff for COVID-19 in group homes and other residential facilities for persons with developmental disabilities, according to emails received under a state Public Records Law request.
The emails, provided earlier this month to COFAR by the Department of Public Health (DPH), appear to imply that as late as last July, both Health and Human Services Secretary Marylou Sudders and Assistant Secretary for MassHealth Daniel Tsai strongly opposed mandatory testing of staff in residential facilities in the Department of Developmental Services (DDS) system.
At the same time, the emails indicated that DPH Commissioner Monica Bharel and members of her office supported mandatory testing.
Sudders has not responded to a request for comment on the matter. In an email to COFAR sent today (February 25), Jennifer Barrelle, Bharel’s chief of staff, said Sudders “was supportive of mandatory testing…” However, Barrelle’s email was unclear as to when Sudders’ support began.
Sudders’ agency, the Executive Office of Health and Human Services (EOHHS), oversees departments such as DDS and DPH. By mid-August, EOHHS finally issued a directive requiring testing of staff throughout the human services system. However, this was some five months after the pandemic became a full-blown crisis in the state.
The apparent opposition by Sudders and Tsai at the top of the human services secretariat as late as July could help explain the lengthy delay in implementing the mandatory testing of residential staff.
COFAR and other advocacy organizations had urged mandatory testing as early as April 2020, arguing that staff were potentially a major source of the introduction of the virus in group homes and other residential facilities. Sudders and other administration officials have never explained why it took so long to finally require staff to be tested.
I sent emails on Sunday (February 21) to both Sudders and Bharel, asking for their comment on the newly provided emails. As noted, Sudders has not responded.
In one internal DPH email, dated July 8, 2020, Bharel stated to several members of her office that she had just spoken with Assistant EOHHS Secretary Tsai:
…and he feels strongly and say (sic) the Secretary (Sudders) does too — around mandatory testing for staff. But he is willing to think it through and learn more. We can discuss at our 10 am call Friday- I know folks on this email have strong beliefs.
Bharel didn’t say in the email what those beliefs were — just that Sudders, Tsai, and “folks on this email” had “strong beliefs” about mandatory testing of staff. The implication, however, was that Sudders and Tsai had different beliefs than did Bharel and her team.
Meanwhile, an internal DPH discussion document in July recommended mandatory testing of congregate care staff.
In her July 8 email, Bharel asked a member of her office to find other instances around the country in which staff testing was mandatory, apparently in order to help make the case to Sudders and Tsai for mandatory testing in Massachusetts.
Bharel further asked in the email whether there was “a model for how many staff need to be tested to feel the surveillance (ongoing testing of staff) is enough? 50%? 60%? How do you decide?”
In her email to COFAR today, Barrelle said that in implementing the mandatory testing program, the administration was involved in negotiations with state employee unions. At least one union filed unfair labor charges against the state for the mandatory testing program, she said.
“You are incorrectly interpreting that Secretary Sudders was opposed to mandatory staff testing,” Barrelle’s email to COFAR stated. “Secretary Sudders was supportive of mandatory testing and rolled it out across all congregate care programs within health and human services within weeks of these (July internal DPH) emails.”
Barrelle’s email to COFAR was not clear, however, as to whether Sudders’ support for mandatory testing may have only begun after July.
DPH office found examples of mandatory staff testing
In a July 9, 2020, email in response to Bharel’s query to her office about other jurisdictions that had implemented mandatory staff testing, the office member provided links to online media accounts in July of testing requirements for staff in colleges and private sector settings.
The office member then noted that in June, the State of Connecticut had begun requiring staff in nursing homes and congregate care settings in that state to be tested for the virus. That was some two months before the Baker administration in Massachusetts issued its mandatory testing directive.
DPH July discussion document recommended staff testing
In addition to the July emails within DPH, a document slated for discussion in Bharel’s office in July included, as a “key question for discussion,” whether COVID testing should be a “mandatory requirement” of staff in state-operated facilities, including hospitals and congregate care facilities.
Option A, which was recommended in the discussion document, was “Yes, testing is a mandatory requirement in state-operated facilities with a goal of achieving full (~90%) compliance.” It wasn’t clear whether this option did or did not include provider-operated facilities.
Under Option A, staff would be given three chances to comply with testing, with a first refusal resulting in a 5-day leave; a second refusal resulting in a 14-day leave; and a third refusal resulting in termination of employment.
Option B was “No, staff are able to refuse testing.”
This second option stated that without mandatory testing, “experience demonstrates that to-date, state-operated facilities are able to achieve 50-65% compliance when access barriers (e.g., shift timing) are limited to the extent possible.”
EOHHS guidance on staff testing, which, as noted, was issued in August by the administration, does not appear to refer to any penalties for staff testing refusals.
Records came from DPH, but not from EOHHS
We initially filed Public Records Law requests last May with EOHHS, DPH, and DDS for internal emails regarding the mandatory testing issue. In June, after EOHHS indicated their responsive records would be voluminous, we modified our request to limit it to emails between Sudders and her executive team.
We received the emails noted above from DPH on February 1. We never received any records from DDS.
On September 30, after two appeals, EOHHS provided us with just one internal email, dated May 22, which consisted solely of a reprint of a blog post that we had published about mandatory testing a few days previously (COFAR Blog: DDS may be flouting state and federal guidelines in failing to make testing of group home staff mandatory).
That sole EOHHS email did not include Sudders on the thread and contained no comment on the subject of mandatory testing or our blog post. Given EOHHS’s initial claim that they had a large number of responsive emails, we again appealed to the Public Records Division, contending it was unlikely there was only one email in existence in the agency on the issue.
On October 15, 2020, the Public Records Supervisor ordered EOHHS to identify other potentially responsive records within 10 days to our original public records request. But EOHHS never acted in compliance with the Supervisor’s order. We received no further communications from EOHHS.
In our email to Sudders on Sunday, we asked why EOHHS still had not complied with the Public Records Supervisor’s October 15 order regarding our records request, and whether the agency intends to comply with it.
Administration still does not report COVID testing results for provider-based staff
In addition to being slow to require testing of staff in the DDS system, the administration has had a spotty record of reporting the results of that testing.
It was not until May that EOHHS began publicly reporting testing data in the DDS system; but the reporting system has continued to have major gaps in it. Those reports contain no information, for instance, on the number of infected staff in DDS provider-run residences, which constitute, by far, the largest network of DDS group homes.
Starting in November, weekly state facility reports had begun showing results of testing on provider staff in all EOHHS human services group homes. But not only were those reports not broken down by individual agency, such as DDS, the reports started combining provider-run group home results with state-run group homes as of February 16 of this year (see final page).
We previously reported that eight emails we did receive from EOHHS in August, based on a separate Public Records Request, showed a consensus in that agency to reduce public reporting of testing data in the human services system.
EOHHS’s lack of commitment to keeping the public informed about the impact of COVID-19 on the DDS system is disturbing. It is also concerning that EOHHS was apparently not in favor for five months of mandatory testing of staff for the virus.
The lack of such testing potentially exposed thousands of residents of DDS facilities to infection. Had mandatory staff testing occurred earlier, an untold number of COVID cases among residents and staff in the system may have been prevented.
