Archive
Limited federal IG probe faults state’s reporting on group home abuse in MA
In one of the few investigations of the community-based system of care for the developmentally disabled, the Inspector General for the U.S. Department of Health and Human Services last week disclosed critical shortcomings in the process in Massachusetts for reporting abuse and neglect.
A report issued by the IG found that incidents of abuse and neglect in group homes were not regularly reported to investigators. The report noted that of a sample of 587 visits by group home residents to hospital emergency rooms, the group homes had failed to report 88 –or 15 percent — of them to the Department of Developmental Services.
In addition, DDS itself and the group homes did not report 58 percent of 175 “critical incidents” to the Disabled Persons Protection Commission, as required by state regulations. And 29 percent of incident reports sampled by the IG did not contain “action steps” to protect individuals involved from future injury.
COFAR has long maintained that the state’s privatized group home system is inadequately overseen and prone to abuse and neglect due to relatively low levels of pay and training, and high turnover among staff. Even the providers themselves acknowledge those problems. Yet the state routinely relicenses the providers to operate homes even though there are clear gaps in the prevention and reporting of abuse and neglect.
The Massachusetts report is the third report issued by the HHS IG thus far on abuse and neglect in individual states. Last year, the IG issued a report on New York State; and in May, the agency issued a report on Connecticut.
U.S. Senator Chris Murphy of Connecticut, who originally requested in 2013 that the HHS IG investigate abuse and neglect in group homes around the country, commented this week on the findings, at least concerning Connecticut and Massachusetts. In a statement issued on Monday, Murphy said he will introduce federal legislation to require reporting of incidents of abuse and neglect, and training of direct care staff in group homes.
Murphy’s office did not respond to a request from COFAR earlier this year for comment on the New York report. As we noted in February, the New York report contained no recommendations and no critical findings, and was only six pages long.
The Massachusetts report, in contrast, was 33 pages long. Like the Massachusetts report, the Connecticut report, which was issued in May, found numerous failures to report abuse and neglect to state authorities.
Despite its thoroughness in examining the incident reporting process in Massachusetts, we believe even the IG’s Massachusetts report was limited in its scope. We think it could have gone much further in investigating the major problems posed by the privatized residential system.
In requesting the IG investigation, Murphy’s 2013 letter to Daniel Levinson, the HHS IG, emphasized the role of privatization in causing “a race to he bottom in our health care system. Privatization of care may mean lower costs but without the proper oversight and requirements for well-trained staff,” Murphy stated.
In limiting its report primarily to findings of failures to report instances of abuse and neglect, the IG has focused on a small piece of the overall problem. The larger issue concerns not only the level of abuse and neglect in the privatized system, but the overall adequacy of care that exists in it.
The HHS IG report did not examine the impact of privatization on the quality of care in the group home system, and did not specify whether the residents whose emergency room visits the IG sampled lived in privatized or state-run group homes.
We have found that the state’s ongoing privatization of residential services has resulted in a corporate, bottom-line approach to care of the disabled. Moreover, DDS has insisted on steering people waiting for residential care to the privatized group home system, all the while failing to provide state-run homes as an option.
The case of Kathleen Murphy is an example. As we have previously reported, Kathleen’s sister and guardian, Patricia Murphy, and members of her family began trying to move Kathleen from a corporate provider-operated group home to a state-operated residence in 1998. DDS continually declined to move her, despite a federal law requiring that the Department provide disabled individuals with a choice among all available alternatives for residential care.
Patricia Murphy finally filed a federal lawsuit in 2013, which resulted in the placement of Kathleen in a state-operated residence. (By way of disclosure, Kathleen Murphy is represented in the case by Tom Frain, who is COFAR’s Board president.)
Patricia Murphy contends that Kathleen suffered nearly 16 years of physical abuse, sexual assaults, emotional torment, and medical neglect in provider-operated group homes. She says her sister was also grossly over-drugged in those facilities, and her clothing, jewelry and spending money were stolen.
The state-operated residence to which Kathleen was finally placed is “the best thing that ever happened to her,” Patricia said. She said that since moving to the state-operated group home, Kathleen has lost 45 pounds, is being fed nutritious food, is off all psychotropic drugs, and her blood pressure is under control.
Yet these experiences as reported by families are apparently of little interest to the federal government, in particular, which, like the state, is committed to further privatization of residential services for the developmentally disabled. While the U.S. Department of Justice has placed a major emphasis in recent years on investigating and closing down state-operated facilities and services for the disabled, there have been few if any comprehensive investigations of the privatized group home system.
Unfortunately, the Massachusetts Legislature has adopted a look-the-other-way attitude regarding these problems. As far as we know, no legislative committee has scheduled any hearings in recent memory on the problem of abuse and neglect in the DDS system.
Both the Legislature and the Baker administration have continued a policy of boosting funding for further privatization of services while slowly starving the much more responsive state-run group home system of budgetary support.
We hope that the IG report, limited as it was, spurs the Legislature to finally pay attention to the big issues that surround the care of persons with developmental disabilities in Massachusetts. Those issues concern privatization and its impact on abuse, neglect, and the quality of care in general.
SJC decision could help family members denied contact with developmentally disabled loved ones
In a decision that could boost the rights of family members in guardianship disputes, the Massachusetts Supreme Judicial Court ruled last month that the grandfather of a young, intellectually disabled woman has the right to intervene in a probate court proceeding in order to gain permission to communicate with her.
It appeared the ruling could be applied to other ongoing probate court cases in which family members have been excluded from contact with loved ones in the care of the Department of Developmental Services.
The woman in the case before the SJC was identified as B.V.G. The SJC ruled that even though the grandfather was not B.V.G.’s guardian, he was an “interested person” within the meaning of the state’s Uniform Probate Code. As such, he had the right to intervene in the court proceeding in order to remove restrictions on his contact with his granddaughter.
According to the SJC ruling, B.V.G. had had a “strong relationship” with her grandfather, which both B.V.G. and the grandfather wished to maintain. However, B.V.G.’s father, who was appointed as her permanent guardian, had sought to sharply restrict or prohibit her contact with her grandfather, and, in fact, with all of her other maternal relatives.
COFAR has reported on a number of cases in which guardians of DDS clients have either made or upheld decisions to restrict contact and visitation rights of family members. Those cases have stemmed from the appointment of attorneys and other non-family members as guardians.
In the B.V.G. case, the restrictions on the grandfather’s contact with his granddaughter were imposed by another family member. The SJC ruling noted that the grandfather had been permitted by the father to send B.V.G. only one email message per day, and to receive no more than one email message from her. But the woman did not have access to email at the residential facility where she lived, so the grandfather and granddaughter effectively had no contact with each other.
The SJC noted that the Uniform Probate Code (which is contained in the state’s general laws) allows anyone defined as an “interested person” to intervene in a guardianship proceeding in probate court. A probate court judge had previously ruled in the case that the grandfather of B.V.G. was not an interested person because he was not her guardian and because he did not demonstrate that he had a financial stake in the court proceeding.
But the SJC concluded that an individual can be considered an interested person under the Uniform Probate Code simply by being interested in an incapacitated person’s well-being. As such, the grandfather of B.V.G. was clearly an interested person, the high court concluded.
In one ongoing case on which COFAR has reported, Stan McDonald, the father of a 49-year-old intellectually disabled man, has been fighting for increased contact with his son, including visits by Andy to Stan’s home. Stan’s son, Andy, lives in a group home. Andy is currently barred from such visits, under a 2006 probate court order, which concluded he was dangerous.
COFAR has reported that the 2006 court order contained a number of factual misrepresentations regarding Andy’s alleged dangerousness.
While it would appear that Stan McDonald would be considered under the Uniform Probate Code to be an interested person in his son’s guardianship, Stan has been told that he has no right even to request home visits from Andy or to discuss such visits with him. Stan has even been threatened with contempt of court for doing so.
Stan’s wife, Ellen, who is Andy’s step-mother, was not permitted to attend a recent probate court hearing on the appointment of a new guardian for Andy, even though she, too, appears to meet the SJC’s interpretation of an interested person in the case.
As interested persons, it would seem that the McDonalds should have input into the terms of Andy’s contact with them. Although the 2006 court order barred home visits for Andy due to his alleged dangerousness, the McDonalds have repeatedly called for an independent clinical evaluation of Andy. Their requests have seemingly been ignored, possibly because they have not been considered to have standing in the case.
As we have noted, not only was the 2006 court order banning Andy’s home visits based on factual misrepresentations in the record, but Andy’s general behavior has greatly improved since that decision was issued.
Both the SJC and the Appeals Court noted in the B.V.G. case that the Uniform Probate Court requires that an incapacitated individual’s changed behavior and “expressed desires” be considered in decisions made by their guardians.
The Appeals Court pointed out that not only should a guardian consider the incapacitated person’s expressed desires, but the guardian has a duty to immediately notify the court if the person’s “condition has changed so that he or she is capable of exercising rights previously limited.”
Andy has repeatedly expressed his desire to visit his parents’ home, and even told a probate court judge of his wish last October. As noted, his behavior has changed since 2006. We are not sure that the probate court has been notified about that. We sent a letter about those issues to the former and current judges handling the McDonald case in Middlesex Probate Court, but have received no indication whether our letter would be accepted into the court record.
By the way, in its amicus brief in the SJC case, the Massachusetts Arc also supported the idea of a family member or friend having the right to intervene in a guardianship proceeding “in order to accommodate the inevitable changes during the lifetime of the person under guardianship.” (our emphasis.)
It isn’t clear to us how the SJC decision will affect cases such as the McDonald case, but we hope that it will lead to a change of attitude within both the probate court system and DDS regarding the rights and standing of family members in guardianship cases.
The attorney for B.V.G. stated at the hearing on the grandfather’s motion to intervene that “we all took it for granted that grandfather had no rights…” That presumption needs to change.
House and Senate not following their own funding plan for employment of the developmentally disabled
For the past three years, the state has been carrying out a policy of closing sheltered workshops for people with developmental disabilities and subsequently placing those people in mainstream workforce jobs.
Yet the Legislature, which bought into this policy, is failing to provide the necessary funding for it.
As the Department of Developmental Services and its corporate service providers jointly proclaimed in 2013, the policy has been to move developmentally disabled people out of sheltered workshops and into community-based day programs and ultimately to the mainstream workforce.
Sheltered workshops are settings in which developmentally disabled people work together on simple assembly-line tasks and are usually paid a small wage. The workshops have gone out of favor because they are viewed as “segregating” their participants from their non-disabled peers in the community.
Since 2013, the majority of the remaining sheltered workshops in Massachusetts have reportedly been closed. All are scheduled to be closed as of June 30 of this year.
But the problem is that the Legislature, and to some extent the administration itself, aren’t following through on the policy, which calls for beefing up funding for DDS day programs and job development staffing. Last week, the Senate joined the House in rejecting higher funding levels considered by the policy planners to be needed by both day programs and employment programs for Fiscal Year 2017.
The irony is that the Democratic-run House and Senate have proposed even less funding for these line items for Fiscal ’17 than Republican Governor Baker has.
A likely result of this apparent under-funding is that relatively few people will be placed in mainstream jobs, but rather will be sent to potentially overcrowded day programs with inadequate staffing.
Day and employment accounts were initially increased, but will now be under-funded or cut
In order to accomplish the policy for “integrated employment” of the developmentally disabled, the Legislature initially increased funding of the community-based day program line item in the state budget, and created a new line item to fund the transfers from the sheltered workshops. The idea was to increase both day program and job development staffing and training.
The new sheltered workshop transfer budget line item (5920-2026) was initially funded in Fiscal ’15 with $1 million. That amount was raised to $3 million in the current fiscal year, and the governor proposed to boost it to $7.6 million in Fiscal ’17. But the House and now the Senate are not going with the governor’s plan.
As the House did last month, the Senate last week approved a budget plan for Fiscal ’17 that will eliminate Governor Baker’s proposed $4.6 funding increase for the sheltered workshop transfer line item. Amendments proposed in both the House and Senate to restore the governor’s increase for the line item were rejected by the House and Senate leadership. As a result, the account will be level-funded next year, which amounts to a cut when adjusted for inflation.
Yet, even the governor’s proposed $4.6 million increase in this line item was $1 million too low, according to the Massachusetts Association of Developmental Disabilities Providers (ADDP). The ADDP lobbies on behalf of corporate DDS providers, which operate day and work programs throughout the state.
In addition, the Senate budget approved last week would provide $700,000 less in spending for the community day and work line item (5920-2025) than the amount the House and the governor proposed. The governor and the House proposed a 4.9 percent increase in that account for Fiscal ’17.
In an email sent to members in early May, the ADDP contended that even the 4.9 percent increase in the day and work line item was $9.8 million less than the what was needed to maintain existing services. As a result, according to the ADDP, DDS was already planning to cut 5 percent in funding for contracts with all day and employment providers.
Should the Senate’s budget plan prevail regarding the day and work line item, it would seem the cut in contract funding for day and employment providers would have to be even deeper than 5 percent.
ADDP urged higher funding and staffing for day care and employment programs
Both the ADDP and the Arc of Massachusetts have become virtual partners with DDS in the operation of the department. The Arc and the ADDP co-authored a report with DDS in 2013 that called for the closures of the sheltered workshops as of June 2015. While that goal wasn’t met, DDS is continuing to work for those closures as of this June of this year.
In comments submitted to EOHHS Secretary Marylou Sudders late last year, the ADDP maintained that funding for both the community day and work line item and sheltered workshops transfer line items needed to be boosted significantly in order to fulfill the plans to close the workshops and transfer clients to mainstream jobs. A failure to boost that funding could put the state in violation of requirements issued by the federal Centers for Medicare and Medicaid Services (CMS), according to the ADDP.
The ADDP comments also noted that as of October 2015, the number of individuals receiving community based day services more than doubled from 2,656 individuals as of June 2013, to 5,422. While noting that this increase was directly related to the closures of the sheltered workshops, the ADDP stated that the majority of those persons were not receiving any other DDS-funded employment services.
The ADDP comments also pointed out that DDS day programs require significantly higher levels of staffing than the sheltered workshops did.
As we pointed out in a blog post in January, DDS records show that the number of participants in sheltered workshops dropped by 61 percent between August 2014 and August 2015, and the number of persons in corporate-run community-based day programs increased by 27 percent. Yet, the number of developmentally disabled people in “integrated employment” settings rose during that same period by only about 6 percent.
It appears that the only policy the Legislature and the administration have pursued with a real level of commitment has been closing the sheltered workshops. But that’s only half the plan. The problem with the Legislature, in particular, is that while it bought into the first half of the plan, it now has seemingly abandoned the critically important second half.
Thousands of people have or will be removed from their sheltered workshops, and the Legislature appears to be leaving an unknown number of them in the lurch.
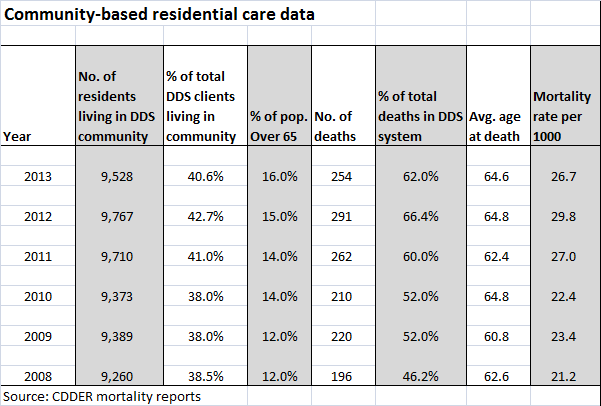
DDS mortality reports show a rise in deaths in the community system since 2008
If you do some intensive searching, you may just find a series of what seem to be fairly well-hidden reports on the Department of Developmental Services website that present data on deaths in the DDS system between the years 2001 and 2013.
We did find those reports, and reviewed them going back to 2008, the year the then Patrick administration implemented its “Community First” initiative. Within DDS, the initiative involved a major push to close large state-run developmental centers and to move the residents of those facilities to community-based group homes.
It appears to be difficult from the data in the reports to draw any firm conclusions about the total numbers of deaths in the DDS system, which have fluctuated substantially in years between 2008 and 2013. There was a low of 406 deaths in 2010 and a high of 438 deaths in 2012.
What did appear to stand out in the data was the significantly higher number of deaths in the community residential system in 2013 than in 2008. There were 196 deaths in the community residential category in 2008, and that number rose to 254 deaths in that category in 2013. That was an increase of 58 deaths per year, or about 30 percent.
The number of deaths in the community system rose in three of the five years between 2008 and 2013. There was a slight drop in the number of deaths in the community system in 2010, and a somewhat larger drop in 2013, the latest year for which the mortality reports are available. Nevertheless, the increase in the number of annual deaths between 2008 and 2013 is statistically significant.
We looked at the mortality report data for two other residential categories within the DDS system — people living at home and people in the remaining developmental centers. We did not review report data for two other categories of residential care — nursing homes, which had a relatively small number of DDS clients living in them during the 2008-2013 period, or for settings listed as “non-DDS facilities.”
In contrast to the community residential system, the numbers of deaths in the developmental centers and living-at-home categories decreased fairly steadily between 2008 and 2013.
The percentages of all deaths in the DDS system rose in the community residential category from 46.2 percent in 2008 to 62 percent in 2013, while the percentages of all deaths dropped in that time in the developmental centers and among people living at home. During that time, the percentage of DDS clients living in the community system increased only slightly — by 2.1 percent.
The data raises some questions. Did the closures of the Fernald, Monson, and Glavin developmental centers, starting in 2008, contribute to the increase in the overall death rate in the community system? Were there people living in those centers who died as a result of having been moved into the community system?
The mortality reports, which were done by the Center for Developmental Disabilities Evaluation and Research (CDDER) within UMass Medical School, do not offer any speculation or answers to that question.
CDDER’s 2010-2011 mortality report does offer some speculation about a statistically significant increase in deaths in the community system between those two years. The report states that the increase may have been due to people with “high medical needs” having been moved into the community at that time from nursing homes. But we found no discussion in any of the reports about the potential impact of moving people into the community from the developmental centers.
The CDDER reports also do not appear to differentiate between corporate-provider-run and commonwealth-operated group homes. The community residential category examined in the reports appears to lump both of those types of residential care together. This allows no comparisons to be made between the state-run and privatized group home systems with regard to the mortality rate.
The CDDER reports do provide the average ages of people in each residential setting. But the reports do not compare average levels of intellectual disability or medical conditions in each category. (Some of the reports did compare the medical causes of death in some of the residential settings, but the data didn’t indicate the percentages of residents in each setting with specific medical conditions such as cancer and heart disease.)
There is a lot of important research contained in the CDDER reports, but the omissions are concerning, though perhaps not surprising. CDDER is under contract to DDS to produce the reports, and they are not going to produce or analyze any data that DDS doesn’t want them to produce or analyze.
For years, we have been critical of the ongoing privatization of DDS services. We have raised concerns about the Patrick and now Baker administrations’ policies of under-funding state-operated care, closing existing state-operated group homes, and preventing people from choosing state-operated care as a residential option.
We have also expressed concern that care in the privatized system is not as well overseen as it should be; that staff in provider-run group homes is often underpaid and inadequately trained, and that provider executives are continuing to make huge salaries nonetheless.
We have also been critical of the closures of the developmental centers, which took place in many cases over the objections of the families of the residents in them.
One would think the DDS-sponsored mortality reports would examine the impact of both the developmental center closures and privatization of services on client deaths among other variables. That is, unless DDS would rather not get into those matters. Based on the reports, it would seem that DDS does not want CDDER looking into the impact of increasing privatization, at least on client deaths.
As a result, we can only glean some hints from the CDDER data about those issues.
According to the reports, the community residential system appears to have grown by about 2.9 percent during 2008-2013 period, which makes sense since people were being moved there from nursing homes and from developmental centers.
The data show that the number of residents of the developmental centers dropped from 925 in 2008 to 550 in 2013 — a 44 percent decrease. Given that the number of residents in the centers was dropping so rapidly, the number of deaths among that population was bound to drop as well. There were 49 deaths in the centers in 2008, and 24 deaths in 2013 — a 55 percent decrease.
Among people living at home, the number of deaths also dropped between 2008 and 2013. There were 69 deaths among people living at home in 2013 — a drop of 18.8 percent from the 85 deaths listed in 2008. The total number of people living at home dropped only by 4.3 percent during that period.
Nursing homes and developmental centers had the highest mortality rates per 1,000 clients among the residential settings, according to the 2012-2013 CDDER report. The report explained that the high mortality numbers in those two settings were due to the relatively advanced age of the residents and their relatively serious health conditions.
As noted, however, the mortality reports don’t appear to have compared medical data among residents living in the various settings. The data do show that an average of more than 30 percent of the residents of the developmental centers were over the age of 65 between 2008 and 2013, compared with about 14 percent of residents in the community and 5 percent of DDS clients living at home.
As of 2013, 550 or 2.3 percent of all DDS adult clients were still living the developmental centers. That year, there were 9,528 clients living in the community system, or 40.6 percent of all DDS clients; and there were 11,822 clients living at home, or 50.4 percent of all DDS clients.
In sum, there doesn’t seem to be too much that is surprising in the data, other than the apparent increase in deaths in the community system between 2008 and 2013.
We think it’s possible that those transfers from the developmental centers may have contributed to that increase in deaths in the community system. But given that CDDER does not appear to have collected data concerning deaths of former developmental center residents, we may never know the real impact on mortality of the closures of the centers.
And unless CDDER begins differentiating between provider-run and state-operated group homes, we may never know the impact of increasing privatization on mortality rates in residential care.
DPPC and other programs for the developmentally disabled to get little or no increases next year
Last week’s House budget debate on the Fiscal 2017 state budget showed just how little, in the way of funding increases, programs for the developmentally disabled will get next year.
In that regard, the House debate was an initial test of the Legislature’s willingness to do better than Governor Baker has with his proposed Fiscal 2017 budget. The House showed it wasn’t willing to do very much.
With the exception of privatized services and one or two other programs, such as family respite services, neither Baker nor the Legislature seem to have put a priority lately on services for the developmentally disabled.
It’s tempting to think of what could be accomplished if some of the state’s $80 million film tax credit, for instance, were diverted to agencies like the Disabled Persons Protection Commission.
Governor Baker’s 2017 budget actually proposes level-funding the DPPC, which is the only state agency in Massachusetts devoted exclusively to preventing and investigating abuse and neglect of disabled persons. A zero increase in nominal dollars would actually amount to a cut in that agency’s budget when adjusted for inflation.
After House leaders last week rejected amendments proposing as much as a $1 million increase for the DPPC, the House did approve an amendment for a $100,000 boost in the agency’s $2.9 million budget. When adjusted for inflation, that would amount to an increase of about 1.5 percent.
As we reported last year, the DPPC has been beset by a chronic lack of adequate funding over the past decade and a maze of legal constraints.
State-run DDS programs will get little or no increases
The governor and now the House have also shown scant interest in raising the level of funding for state-run programs for the developmentally disabled, particularly commonwealth-operated group homes.
We had asked a legislator, on behalf of some of her constituents, to file an amendment to boost funding for the commonwealth group-home line item. The legislator’s constituents happen to have a family member in a commonwealth-operated group home, and they are concerned about the flat or declining level of funding for those facilities. The legislator, at the last minute, declined to file the amendment.
In his budget, Baker proposed less than a 2 percent increase in funding for the commonwealth-operated group home line item, which would also amount to a cut in inflation-adjusted terms. Last month, I asked Department of Developmental Services Commissioner Elin Howe about that. While Howe admitted the funding proposed for the commonwealth group homes is inadequate, she said DDS did not intend to seek an amendment in the House budget to increase that funding.
We believe the governor proposed about $500,000 less for the commonwealth-operated group homes than what DDS itself believes is needed. Howe’s response to us, however, was, “We’re just going to have to manage it.” It appears that the DDS mindset is that eventually the commonwealth-operated programs will be privatized, so it is not worth pushing for more money for those programs.
Also rejected by the House last week was an amendment that would have provided for a $3.4 million increase in the DDS administrative line item, which funds DDS service coordinators. The governor and House Ways and Means Committee have together approved only a $400,000 increase in that line item, which actually amounts to a 1.2 percent cut when adjusted for inflation. The line item for the service coordinators, like the line item for DPPC, has been continually underfunded despite rising caseloads in recent years.
Privatized DDS services
Corporate provider-operated residential services is one of the few areas in which Baker has continued to propose increased funding. In that case, we agree with the House, which apparently considered Baker’s proposed $26 million increase in the corporate provider residential line item to be enough. House leaders rejected an amendment that would have boosted the line item by $6.5 million over the governor’s increase.
The House similarly rejected amendments for increases, above what the governor had proposed, in both the community-based day care line item and a pilot program to fund transfers from sheltered workshops into community-based day care. Baker had actually proposed a $4.6 million increase in that particular program, but the House Ways and Means Committee rejected it.
When it comes to privatized services, we’ve said before that the budget is out of balance. The corporate provider residential line item has been increased too rapidly, at the expense of almost all other DDS programs.
We’ve also opposed the closures of sheltered workshops throughout the state, and the transfer of that funding to day care programs.
The increases that the House did approve
There were a few amendments that were accepted last week to increase funding:
The House did approve $50,000 to further expand Operation House Call. As we’ve reported, the program, which is run by the Arc of Massachusetts, provides instruction to students in medical and nursing schools in Massachusetts on treating people with autism and other developmental disabilities.
Operation House Call appears to be a good, though limited approach to addressing the lack of training of health care professionals. We were supporting a bill requiring a more comprehensive approach to the problem. Last month, the Public Health Committee approved that bill. But the committee then quietly approved substitute language to the bill to expand Operation House Call, and dropped the more comprehensive program.
Family supports, as mentioned, was one other area where Baker actually proposed more than a token increase in funding for next year. His Fiscal 2017 budget calls for a $6.8 million, or 12 percent, increase in that line item.
The House last week approved an additional $100,000 increase in the family support and respite line item and earmarked that increase for persons over 40.
Those proposed increases in funding for family supports are good moves. But in the final analysis, we believe the governor and Legislature need to rethink their priorities when it comes to budgeting services for the developmentally disabled.
Committee quietly changes bill to train health care professionals in dealing with developmentally disabled persons
The Massachusetts Legislature already has a reputation for a lack of transparency in the way it does business; and a case involving a bill that would provide training for medical personnel in dealing with developmentally disabled persons would seem to enhance that reputation.
The bill was quietly changed last week by the Public Health Committee without a vote — and the change appears to have greatly reduced the scope of the bill and benefited the politically connected Arc of Massachusetts.
We’re not blaming the Public Health Committee for going rogue on this matter. In fact, it appears the chairs of the Committee were doing business as usual in the Legislature, and taking their marching orders from politically connected lobbyists and who knows who else.
Last month, the Public Health Committee appeared to have demonstrated that needed legislation does occasionally move forward in the Legislature. The Committee approved what we considered an important bill (H. 1932) that would have required training of health care professionals who deal with developmentally disabled persons.
The bill had sat in the Committee for more than a year, but Representative Kate Hogan and Senator Jason Lewis, the co-chairs of the committee, made sure that the bill got voted on before the session deadline on March 17. Had they not acted when they did, the bill would have died. (That was the case with a key guardianship bill in the Judiciary Committee.)
H. 1932 first came to our attention some months ago when we were fighting with the Department of Public Health for a copy of an investigative report on a developmentally disabled man who died after being turned away twice from Lowell General Hospital. While the DPH report exonerated the hospital in the case, it also left a number of questions unanswered, including whether the emergency room staff at the hospital was trained to deal with people with developmental disabilities.
In many cases, developmentally disabled people are nonverbal, and even in cases in which they are verbal, they may report medical symptoms differently than do non-disabled people.
H. 1932 seemed to potentially address those problems in requiring that medical and other professionals to receive training in dealing with people with developmental disabilities. Given that the bill was still stuck in the Public Health Committee as of early March, I asked Rep. Hogan about the legislation during a meeting we had with her in her district office. Hogan’s aide said she would look into getting the bill out of the committee.
That appeared to be what happened. On March 21, I received a message from Hogan’s aide, saying H. 1932 had been reported favorably by the Committee. This seemed to be good news, particularly compared with what had happened at the same time to the guardian bill.
But in checking the Legislature’s online bill site earlier this week, I saw that the Public Health Committee had made a quiet substitution to H. 1932. On April 7, the Committee had substituted a new bill (S. 2211) for the bill it had reported out favorably. This new bill would expand a voluntary training and accreditation program that is geared toward medical and nursing schools. The existing program, known as Operation House Call, has been run by the Arc of Massachusetts for several years. The program provides instruction in treating people with developmental disabilities in hospital settings, including people with autism.
Here’s the key from the Arc website: “All of the participating (medical and nursing) schools provide funding toward Operation House Call.” So this appears to be an expansion of a program that has provided funding to the Arc.
The program as described in S. 2211 appears to be a good program, but it appears to be more limited in scope than H. 1932, and more limited than what had been envisioned in a second bill (S. 1180), which had also been in the Public Health Committee. That second bill would have required DPH to provide training on autism to physicians, emergency room personnel and other health care professionals. S. 1180 would also have required DPH to design a pilot program for an “autism team” in hospital emergency rooms.
H. 1932 had further contained broad language that would have required the Executive Office of Health and Human Services (EOHHS), to evaluate discrimination against developmentally disabled persons and to issue regulations to reduce the impact of “disparities in outcomes” for those people in medical settings. As we reported, there have been a number of studies showing such disparities in outcomes for people with developmental disabilities.
In our view, this whole episode is a case study in how even good legislation gets put together in secret in the Legislature, and how certain organizations like the Arc so often seem to benefit from it. We say this was done in secret. Clearly the Public Health Care Committee voted on one bill, and then another bill was quietly substituted for it by unnamed parties with no vote.
Now the substituted legislation goes to the Health Care Financing Committee, where it may secretly get changed again, very possibly to provide even more benefits to politically connected lobbyists.
Yet another frustrating morning in probate court for Stan and Ellen McDonald
Stan and Ellen McDonald spent a morning last week in probate court, and the outcome, as usual, was frustration and disappointment for them.
If any case illustrates the absolute necessity of maintaining guardianship over a person with developmental disabilities, this case is it.
Stan and his wife, Ellen, are trying to overcome a devastating court ruling from a decade ago in which a judge concluded that their son, Andy, an intellectually disabled man, is so dangerous that he must be banned for life from ever returning to his hometown of Sherborn, where Stan and Ellen still live.
We have pointed out that the 2006 ruling by former Probate Judge Edward Rockett contains factual misrepresentations about both Andy and Stan, and that the decision does not take into account changed circumstances in the case, including greatly improved behavior on Andy’s part. That ruling, however, was supported by Andy’s previous court-appointed guardian and by DDS; and Stan and Ellen have found that their opinion of the ruling doesn’t count for much.

Stan and Ellen outside a probate courtroom where they encountered yet another round of frustration and disappointment last week.
In 1986, Stan and his former wife agreed to the appointment of a guardian for Andy as part of the settlement of a longstanding custody battle over him. Since then, Stan has learned the hard way that once you agree to the appointment of a guardian from outside of the family, it can be difficult if not impossible to regain guardianship rights. And if you are not a legal guardian, you have little or no standing in probate court.
Andy is now 48 and Stan is now 80; and Stan isn’t sure how much longer he and Ellen will be able to make the trip to visit Andy in his group home in Northborough.
Lately, though, Stan and Ellen have found themselves repeatedly making an even more arduous trip — to the Middlesex Probate Court building in East Cambridge, where they have been fighting what has been a more than frustrating battle to convince the court that there would be virtually no risk in supervised home visits for Andy. But just getting up the two flights of outside and inside steps in the court building to where the elevator is located now presents a major challenge for Stan.
To say the system is stacked against Stan and Ellen would be an understatement, particularly since, at this point in their lives, they can’t afford to hire an attorney to represent them. I accompanied them to a scheduled hearing last Thursday in the courthouse. The purpose of the hearing was to appoint a new permanent guardian for Andy — needless to say another guardian from outside the family. Stan and Ellen have never met the new guardian, who was appointed on a temporary basis last October.
I can tell you that other than the clerk to the probate court judge in the case, no one at the court house appeared to be particularly helpful let alone nice to Stan or Ellen. The DDS attorney on the case, in fact, repeated a threat she first made last fall to seek contempt of court charges against Stan if he were to mention to the judge his desire for home visits from his son.
It’s strange because it is apparently perfectly okay for Andy himself, or his court-appointed attorney, to say in court that Andy desires home visits. Why Stan could end up getting sent to jail for saying the same thing is beyond me.
Last October, there seemed to be a ray of encouragement for the McDonalds. The probate judge at the time, Megan Christopher, seemed to be open to considering home visits for Andy. Andy did testify at that hearing and politely asked that he be granted a supervised visit home for a couple of hours. Christopher said she would take it under consideration.
But shortly after the October hearing, Christopher was re-assigned to another courthouse, and all of her cases went to another judge, Randy J. Kaplan. It’s not that we have any reason to believe Judge Kaplan will be less sympathetic to the McDonalds, but it’s as if the whole ordeal of the October hearing never happened, and the McDonalds had to begin again with a new judge.
Last week, when Stan and Ellen arrived at the probate court, Andy wasn’t there. Andy’s attorney told Stan that Andy had said he didn’t want to make the trip to the court that day. And then Andy’s attorney let Stan know that she was resigning from the case as of that day. So, as far as we know, no one in the McDonald family has legal representation in the case right now.
When Stan and Ellen’s case was finally called at close to noon, there was a short conversation between the DDS attorney, Andy’s attorney, and Judge Kaplan at the bench. The court officer then announced that the hearing would be closed, and all non-parties had to leave. That included me, but it also included Ellen, who has no legal standing in the case. This was not the case with Judge Christopher, who had let Ellen, myself, and another advocate for the McDonalds remain in the hearing she presided over last fall.
In last week’s hearing, Stan alone was allowed to stay, apparently because he is on record as having objected to the appointment of the new, non-family guardian for Andy. So, Stan was by himself in there, without legal representation and being threatened with contempt of court if he said the wrong thing as far as the DDS attorney was concerned.
The hearing itself was over in minutes. It was essentially continued until June 2.
At this point, we think the only hope for home visits for Andy lies in having an independent clinical evaluation done to determine whether he really is dangerous. Actually, we have been calling for this for two years.
We don’t think Andy is dangerous and we don’t think anyone who knows or cares for him regularly believes he is. But whether to have an independent evaluation is a decision that can only be made by Andy’s new guardian.
As usual, Stan and Ellen, the people most directly involved and affected, have no say in it.
Sen. Brownsberger and Rep. Fernandes once again order family rights bill sent into legislative black hole
More than a year after an important family rights bill (H. 1459) for persons with developmental disabilities was sent to the Legislature’s Judiciary Committee, the committee co-chairs have decided it’s time to study the measure.
Yes, we understand that as of yesterday, three days before the Thursday drop-dead date for bills that have not been voted on in committees in the current legislative session, Senator William Brownsberger and Representative John Fernandes ordered H. 1459 sent to yet another legislative study.
Of course, we know what a study really means in Massachusetts Legislature-speak. It’s a euphemism for a legislative graveyard, or to use another metaphor, a legislative black hole from which nothing ever emerges. No study will ever be done on H. 1459. It will have to be refiled as a new bill next year if it is ever to see the light of day again.
Since the bill is only technically still alive, but is in actuality dead, I think we can refer to it in the past tense. The bill proposed that a spouse or parent be presumed in probate court to be the proper person to be a guardian of a developmentally disabled or otherwise incapacitated person unless competent evidence is introduced to the contrary.
We consider H. 1459 to have been a critically important rights measure for family members of people with disabilities — particularly developmental disabilities — who are routinely overruled in decisions about the care of their loved ones in probate court proceedings by medical and clinical “experts,” state agencies, probate court judges, and service providers.
In many of those cases, developmentally disabled people are viewed as valuable funding sources, particularly by privatized group home providers who get billions of dollars in taxpayer money to provide those people with residential services. That is why the Department of Developmental Services, which is intent on further privatization of its services, is particularly eager to get attorneys and corporate providers appointed in probate court as guardians. Those non-family guardians are much more likely than are family members to cooperate with DDS’s privatization agenda.
State Sen. William Brownsberger (left) and Rep. John Fernandes (center), co-chairs of the Judiciary Committee, confer with a legislative aide during a committee hearing in June 2015 on H. 1459 and related bills. It now appears they were probably discussing their legislative “black hole” strategy for many of those bills.
If Brownsberger and Fernandes and other members of the Legislature really cared about the issues that H. 1459 is concerned with, they would have acted on the bill by now. In fact, they had 17 years to study it, including the entire year and two months that the bill sat in the Judiciary Committee in the current session with no action on it. This bill has been repeatedly filed since 1999, and we know it has been sent to similar “studies” in past legislative sessions. But apparently, no one has learned a thing about the bill in those past studies, and we’re sure that will be the case yet again.
As we reported last month, this legislative session initially appeared to be different with regard to H. 1459. While COFAR has long supported the measure, it garnered the support last year for the first time of other major advocacy organizations for the developmentally disabled, including the Massachusetts Developmental Disabilities Council, which is technically part of the Baker administration. The MDDC listed H. 1459 as one of its legislative priorities for 2015-2016.
The Judiciary Committee did hold a public hearing on H. 1459 last June. COFAR, the MDDC and other organizations submitted testimony in support of the measure. As far as we know, the bill was not controversial, and no one raised any opposition to it at the hearing.
But the months dragged on and the Judiciary Committee did nothing about the bill. In January, State Sen. Richard Ross and Rep. David Linsky sent a letter to Brownsberger and Fernandes, urging them to finally pass the bill and saying it had their full support. Their letter noted that in light of continuing budget cuts to service coordinators in the DDS system, “family guardians are particularly crucial in managing their child’s transition and medical decisions.” But the letter apparently had no effect.
Ross and Linsky are the local legislators of Stan McDonald, who has been fighting unsuccessfully against DDS for years to gain guardianship of his developmentally disabled son, Andy. It is Linsky who has repeatedly filed the guardianship bill since 1999 on behalf of McDonald and an unknown number of other people who are in similar positions.
We may never find out the real reason that the guardianship bill can never get through the legislative process. But it’s my guess that DDS, for reasons discussed above, does not like the legislation. And experience has taught us that legislators on Beacon Hill rarely, if ever, challenge the authority of agencies like DDS or their lobbyists and corporate providers.
HHS IG’s Office defends 6-page report on abuse and neglect of disabled in NY State
The Inspector General’s Office for the U.S. Department of Health and Human Services has responded to our questions about the methodology underlying their report on abuse and neglect in residential facilities for the developmentally disabled in New York State.
As a spokesperson for the Office put it, in an email accompanying the Office’s responses, “I think you will see we were quite thorough in our work.”
I’ll summarize the Office’s responses below. But we have to disagree with the suggestion that this report was thorough. A six-page report (actually four pages if you leave out the methodology section) that contains no recommendations concerning a subject as serious and complex as abuse and neglect in a system with thousands of residential facilities and tens of thousands of program recipients cannot by definition be thorough.
As we noted previously, Senator Chris Murphy of Connecticut had asked HHS Inspector General Daniel Levinson in 2013 to investigate the privatized group home system around the country in the wake of exposes in both The Hartford Courant and The New York Times that revealed horrendous cases of abuse and neglect in group homes in their respective states.

A group home in Hudson Falls, NY, where a worker allegedly sexually assaulted a developmentally disabled woman, according to a New York Times report
The report released by the IG on New York State’s residential system is the first of three reports that the Office plans to issue in response to Murphy’s request. Two additional reports are expected to be released, based on similar reviews in Massachusetts and Connecticut.
What the IG actually did in the first report was to conduct a review of the outcomes of hospital emergency room visits by residents of a selected sample of 12 Intermediate Care Facilities (ICFs) in New York State. Those 12 ICFs were selected because more than 70 percent of the residents in each of the facilities had had an ER visit in 2012 and 2013.
While some of the ER visits were due to alleged abuse and neglect, the IG concluded that the incidents were reported to the appropriate agencies, and that the “vast majority” of the ER visits were due to underlying medical conditions of the residents. The report noted that it contained no recommendations, and essentially concluded that the IG had found nothing wrong in the system.
Senator Murphy has not responded to queries from us as to whether he is satisfied with the IG’s work so far in response to his call for the investigation.
Below are the key questions we posed to the IG about the New York report and a summarization of the IG’s responses (not necessarily in the order we posed the questions):
1. What about deaths?
As we previously stated, the IG’s review appears to have been limited to outcomes of persons sent to ERs from a sample of ICFs. Sen. Murphy’s letter to the IG in 2013 specifically requested that Levinson investigate preventable deaths in group homes. In limiting his review to persons taken to ER’s, didn’t Levinson’s study miss deaths in which no one was taken to an ER?
The IG’s response stated that they reviewed all reported deaths involving the 109 residents of the facilities examined during the audit period. There were a total of 12 reported deaths among the residents in seven of the 12 ICFs. All 12 reported deaths were from natural causes, the IG stated.
This response demonstrates to us just how limited the selected sample of facilities was that the IG chose to review. The New York Times reported in 2011 that 1,200 deaths in group homes in the past decade “have been attributed to either unnatural or unknown causes.”
In 2013, The Courant reported “dozens of developmentally disabled people who died in public and private group homes, institutions and nursing homes from 2004 through 2010 in cases where investigators cited abuse, neglect or medical error as a factor.”
2. Why was the IG review limited to ICFs, when, in fact, many group homes in New York State are not ICFs?
As we noted, ICFs are a distinct category of residential facility for the developmentally disabled. They are required to meet strict federal standards for care under the federal Medicaid statute, and tend to serve profoundly disabled and medically involved people.
Also, it’s not clear how many, if any, of the ICFs examined by the IG actually were group homes. Many group homes operate under the Home and Community Based Settings (HCBS) waiver to the federal Medicaid statute, which exempts those homes from ICF requirements.
In their response, the IG’s Office stated that they first used a state computer database to identify Medicaid claims submitted by more than 1,100 residential providers for close to 41,000 intellectually disabled Medicaid beneficiaries in New York State.
The IG then determined that close to 23,000 of those beneficiaries had some 146,000 ER visits charged to Medicaid totaling $1.6 million.
The IG next determined that those beneficiaries resided in 33 state-operated and 395 privately operated ICFs. Of that total of 428 ICFs, the IG selected 12 for which more than 70 percent of the residents had had an ER visit. The review involved 109 residents of those 12 ICFs.
But it still isn’t clear to us how many, if any, of the facilities reviewed were actual group homes, which tend to have 6 residents or fewer in them, or why the IG appears to have limited their review to ICFs.
In their response, the IG stated that four of the 12 ICFs in their sample were actually “HCBS Waiver ICFs.” I sent the IG’s Office a follow-up email to try to clarify this. As I noted, it is our understanding that a group home or other facility that operates under the HCBS waiver is not considered an ICF, but is an “alternative” to an ICF. I haven’t yet received a response to that request for a clarification.
The IG’s Office also hasn’t responded to a second follow-up question as to how many, if any, of the 12 ICFs reviewed were actual group homes. Senator Murphy had asked for an investigation of group homes.
3. Could there be an overlooked variable biasing the results as a result of the IG’s methodology? For instance, might a group of ICFs have a high percentage of patients admitted to ERs because those are the ICFs with the most medically fragile patients?
The IG’s response to this was that “the entire population in ICF’s is a fragile population,” and that “no bias was involved” in their method of selecting the 12 ICFs for review.
But this answer doesn’t respond to the question, which assumes that there are some differences in the average degree of medical fragility of residents in different ICFs. Our guess is the IG’s sample is likely to have consisted of the ICFs housing the sickest residents on average. Those residents would be the most likely to die of “natural causes” rather than abuse or neglect. So that might provide one reason why the IG did not find evidence of abuse or neglect in the deaths of the residents in those facilities.
3. Why did the IG look at data for only two years — 2012 and 2013? Shouldn’t the IG have examined data over at least a 10-year period?
The IG’s response was that the process of identifying the Medicaid claims for 41,000 beneficiaries over two years took “a great deal of time and manpower,” and that the Office didn’t have the time or resources to do more.
5. Did the investigators interview staff, families etc. in any of the facilities?
The IG responded that all 12 ICFs were visited and that staff and beneficiary records were reviewed. Apparently no staff or family members were interviewed.
In critiquing this report, we’re not trying to criticize the IG’s other investigations or audits of the health and human services system. We think the IG took the wrong approach to this particular investigation. It was an approach that took them nowhere, and the report reflects that. To that extent, it was a huge missed opportunity. As we noted in our last post, federal investigations of the privatized group home system have been few and far between.
Rather than using a questionable methodology to try to come up with their own data on abuse and neglect, the IG could have reviewed existing records on abuse and neglect that are available in state agencies in New York State. At the very least, the IG could have tried to confirm the findings of the Times and the Courant. Better yet, they could have looked at what actions have been taken in each state to address the newspapers’ findings, and whether those actions have resulted in any improvements that might have been reflected in the state agency data.
It probably goes without saying that the IG should have interviewed families of residents of the facilities they examined.
Despite any implications that might be drawn from the IG’s New York report, we’re sure the problem of abuse and neglect in the group home system has not gone away. A systematic federal investigation of this problem is still sorely needed.
Is Senator Chris Murphy really just fine with this IG’s report on abuse of the disabled?
It’s hard to believe the Inspector General for the U.S. Department of Health and Human Services has come up with a report about abuse and neglect of the developmentally disabled in New York State that doesn’t have any recommendations in it.
And it’s hard to believe that U.S. Senator Chris Murphy of Connecticut, who had asked for the IG investigation, is okay with this report. Well, we don’t really know how he feels about it. We have been unable so far to elicit a comment from his office about it.
The IG took two and a half years to do this report, which was released last September (although we have only now seen it), and the results seem cursory to say the least. Moreover, the methodology the IG used in the 6-page report (that page count includes an appendix on that methodology) seems questionable.
Based on that methodology, the IG essentially found no problems in New York’s group home system. Well, it’s not clear exactly what types of residential facilities were actually examined. More about that and the IG’s methodology below.
We understand that the IG has not yet released additional reports done on Connecticut and Massachusetts, also in response to Murphy’s request. But if those latter reports have employed the same methodology and lack of apparent rigor as the report on New York, we would expect to see similar non-findings and non-recommendations in them.
In March 2013, Sen. Murphy had asked the IG to investigate the privatized group home industry around the country in the wake of major newspaper exposes in both his state of Connecticut and in New York State about poor care and worse in those facilities.
Both The Hartford Courant in Connecticut and The New York Times had found numerous instances of horrendous abuse and neglect (here and here) in the group home systems in those states that resulted in many cases in deaths of disabled people and serious injuries. In case after case, vulnerable and disabled people were found to have been subjected to sexual and other types of assaults, inadequate care, and substandard conditions in facilities with underpaid and poorly trained staff.
As the Times noted in one of its articles, while the staff of these group homes may have been poorly compensated, the executives of the state-funded companies running the homes were often generously paid.
While the privatized group home industry sprang up in response to reports of abuse and neglect in large institutions in the 1970s, the Courant and Times articles, and many similar media exposes in other states, have more recently raised the question whether group homes have become the new warehouses for developmentally disabled people.
To give Murphy credit, he was one of the few prominent elected officials to express public concern about the group home industry in the wake of the Courant and Times exposes. In 2013, shortly after he was elected a senator in Connecticut, he seemed to be outraged by the Courant’s findings, in particular. He wrote a strong letter to Daniel Levinson, the HHS IG. Murphy’s letter opened by stating:
I write to you today to request that you undertake an immediate investigation into the alarming number of deaths and cases of abuse of developmentally disabled individuals in group homes. In particular, I would like you to focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.
Citing accounts of abuse and neglect in Connecticut, New York, Massachusetts, Virginia, Louisiana, and Texas, Murphy’s letter added:
These examples and countless others from across the nation are indicative of a larger problem of the race to he bottom in our health care system. Privatization of care may mean lower costs but without the proper oversight and requirements for well-trained staff.
Murphy’s letter to Levinson noted that prior to his becoming a U.S. senator, he had led the charge in the Connecticut Legislature in 2005 to enact a moratorium on conversations of state-run group homes into privately run residences, which are nevertheless publicly funded.
Since 2013, however, Murphy seems to have gone silent on this issue. His office has never responded to queries from us in the past two years about his call for the IG investigation, and we’ve received no response to a call to Murphy’s office last week and to an email this week, asking if Murphy is satisfied with the IG’s work so far.
Our questions and concerns about the IG’s report primarily have to do with the IG’s apparent decision to conduct a much more limited review than what Senator Murphy had asked for. Coupled with the sharply limited nature of the review is what appears to be a vagueness about what was examined. The report doesn’t appear to fully specify, for instance, which types of residential facilities were included in the review.
The report says that the review was limited to Intermediate Care Facilities (ICFs) in New York State in which at least 70 percent of their intellectually disabled Medicaid beneficiaries had an ER visit from 2012 through 2013. This resulted in a review of cases involving 109 persons at 12 ICFs.
ICFs are a distinct category of residential facility for the developmentally disabled. They are required to meet strict federal standards for care under the federal Medicaid statute, and tend to serve profoundly disabled and medically involved people.
The IG’s report stated that New York State has both state-run and privately run ICFs, and that the privately run facilities have less than 30 beds. All that is stated in the report is that the sample of ICFs selected by the IG included two state-run ICFs and 10 privately run ICFs. The report, however, doesn’t say whether any of the ICFs were actual group homes, which tend to have far fewer than 30 beds.
Here is the single finding or conclusion of the IG’s report:
ICFs in New York with high rates of ER visits by intellectually disabled Medicaid beneficiaries under their care reported … these visits, as required, and potential neglect or abuse was reported and investigated (by the appropriate state agencies). However, the vast majority of ER visits we reviewed resulted from circumstances associated with the Medicaid beneficiaries’ underlying medical conditions—not from neglect or abuse. Accordingly, this report contains no recommendations…
In written comments on our draft report, the health department stated that it was pleased that we had no recommendations.
While it’s not surprising the health department is pleased by the lack of recommendations in the report, we would think that, at the very least, taxpayers, who paid for this two-and-a-half-year investigation would have preferred the investigation to have resulted in recommendations. But more importantly, how is it possible that an investigation of a topic of this magnitude and complexity could essentially find nothing wrong? Particularly, when we know there is a lot wrong with the system.
Here are some of the questions we’ve posed to the IG regarding the methodology used in the report: (We’re still waiting for their reply.)
1. Why was the IG review limited to ICFs, when, in fact, many group homes in New York State are not ICFs?
As noted above, it’s not clear how many, if any, of the ICFs examined by the IG actually were group homes. Moreover, the report doesn’t appear to mention the Home and Community Based Settings (HCBS) waiver to the Medicaid statute under which most group homes operate. The waiver exempts those homes from ICF requirements.
New York State does appear to have privately run group homes that operate under the HCBS waiver. Were group homes, which do not operate under ICF rules, included in the review? If not, why not?
2. Could there be an overlooked variable biasing the results as a result of the IG’s methodology? For instance, might a group of ICFs have a high percentage of patients admitted to ERs because those are the ICFs with the most medically fragile patients?
3. Why did the IG look at data for only two years — 2012 and 2013? Shouldn’t the IG have examined data over at least a 10-year period?
4. What about deaths? The review appears to have been limited to outcomes of persons sent to ERs from a sample of ICFs.
Sen. Murphy’s letter to the IG in 2013 specifically requested that Levinson investigate preventable deaths in group homes. In limiting his review to persons taken to ER’s, didn’t Levinson’s study miss deaths in which no one was taken to an ER?
5. Did the investigators interview staff, families etc. in any of the facilities?
One of the reasons we’re so disappointed in the IG’s New York report is that it appeared to be one of the few instances in which the federal government had undertaken an investigation of privatized healthcare. In recent years, state-run care has been a persistent focus of federal investigations, while privatized care appears to have gotten a free pass. Between 2009 and last year, the U.S. Justice Department had filed more than 45 legal enforcement actions in 25 states to limit or shut down state care.
The reason for that apparent bias against state-run care appears to be, in part, an ideology held by the the current and previous administrations against institutional or congregate care, which is primarily state-run. That ideology has become so fervent, in fact, that only the smallest group-home settings are considered acceptable by federal organizations such as the National Council on Disability.
But there has been a persistent drumbeat of information about poor care in these smaller, privatized settings, and a lack of oversight of them. But all the HHS IG has produced so far in response to this drumbeat is a six-page report that has no recommendations. We have to hope Senator Murphy isn’t satisfied with that.
