Archive
DDS not commenting on future of state-operated group homes as FY ’18 funding is sharply cut
In the wake of a projected state budget deficit, Governor Baker and the Legislature have approved their deepest cuts yet in funding for state-operated group homes and other programs managed by the Department of Developmental Services.
Yet funding for privatized group homes will still increase by tens of millions of dollars under Baker’s final Fiscal Year 2018 budget, although that increase will be somewhat less than what Baker had originally proposed.
The cuts in Baker’s final budget for Fiscal 2018, which began July 1, include a $10.5 million reduction in funding for the state-operated group homes and a $2.2 million reduction in the DDS administrative account, which funds critically important service coordinators. The state-operated group homes are the hardest hit of any DDS funding account.
We have previously reported that the administration and Legislature appeared to have placed a priority on funding privatized DDS services. The final Fiscal 2018 budget may provide the sharpest indication yet of that priority, which is reflected in the chart below. The chart shows final appropriations since Fiscal 2012 for key DDS privatized and state-run program line items.

In January, when Baker submitted his Fiscal 2018 budget to the Legislature, he proposed $59.9 million in additional funding for privatized DDS group homes, while at the same time proposing a $1.8 million cut in the state-operated group home account.
The House and Senate initially largely rubber-stamped Baker’s DDS budget plans. Then, in early July, a House-Senate conference committee, working behind closed doors, recommended a cut more than five times deeper for the state-operated group homes — $10.4 million.
The governor’s final budget went even further, cutting state-operated group home funding by $10.5 million for Fiscal 2018. That amounts to a $15.6 million cut when adjusted for inflation.
Meanwhile, the governor’s final budget only moderately reduced the increase Baker had initially proposed for the privatized group home system — lowering that proposed $59.9 million increase to $47.6 million.
Similarly, the governor had initially proposed a cut of $97,000 in the DDS administrative line item, which funds the service coordinators. However, while the House and Senate initially rubber-stamped that cut, the conference committee in July deepened the cut to more than $2.1 million. The governor then further cut the administrative line item in his final budget by an additional $50,000, deepening the total cut to nearly $2.2 million.
Service coordinators are DDS employees who help ensure that clients throughout the DDS system receive the services to which they are entitled under their care plans. As COFAR has reported, service coordinators could find their jobs threatened by privatized “service brokers.”
Also slated for deepened cuts are the state-run Wrentham and Hogan developmental centers — the two remaining facilities in Massachusetts that are required to meet stringent federal Intermediate Care Facility (ICF) standards.
In January, Baker proposed a $2.4 million cut in the developmental centers line item. The conference committee more than doubled the size of that cut, to $5.4 million, and the governor’s final budget adopted the conference committee’s number.
DDS not commenting on fate of state-operated group homes
Despite the fact that the state-run group homes have been targeted for the deepest cuts in the DDS budget, DDS is apparently not commenting on whether it has any plans to phase out the state-operated group homes entirely.
After reporting in March that there had been a drop in the number of people living in state-operated group homes, we asked then outgoing DDS Commissioner Elin Howe whether DDS had any policies or plans for the phase-down or closure of those facilities in Massachusetts. We never received a response to our email query. Howe retired from her position on July 14.
In March, an assistant general counsel at DDS said that the Department had no public records pertaining to any policies or plans to close the state-operated group homes.
Even if there are no written policies regarding the phase-down of state-operated group homes, the evidence seems to be mounting that state-run DDS services are under siege in Massachusetts.
We will continue to monitor the funding levels proposed and approved for state-run DDS programs. So far, the trends do not look good. Please call your state legislators and express your concern. You can find your legislators at: https://malegislature.gov/Search/FindMyLegislator
State’s system of paying guardians and attorneys for the developmentally disabled appears secretive and poorly overseen
State payments to attorneys and corporate providers to serve as guardians of developmentally disabled clients are rising rapidly, yet the payment system appears to be secretive and subject to spotty oversight.
An investigation by COFAR shows the system in Massachusetts and regulations that support it also appear to give professional guardians an incentive to do little work representing individual clients while taking on as many clients as possible.
In addition, the fact that professional guardians are paid by the Department of Developmental Services appears to interfere with their legal obligation to act in the best interest of their disabled clients. We have found in a number of cases that both professional guardians and attorneys appointed to provide legal representation to disabled clients have sided with DDS when family members have gotten into disputes with DDS over the care of those clients.
In one case on which we have reported, a developmentally disabled woman’s state-appointed attorney has sided with a DDS-paid guardian in not allowing any family visitation of the woman for an indefinite period of time. In that case, David Barr, the father of the woman, and Ashley Barr, the woman’s sister, have been banned from all contact with her, and even from knowing her whereabouts, for more than a year and a half.
We believe this and similar cases raise questions whether DDS-paid guardians and state-paid attorneys consistently act in the best interests of their clients.
COFAR examined probate court documents and payment data involving attorneys and corporate entities paid by DDS to provide guardianship services to persons in which family members are not available or have been removed as guardians.
COFAR has also sought information on the payment of attorneys who are hired under the probate system to provide legal representation to incapacitated persons. In those cases, the court approves attorneys as counsel, and the attorneys are paid by a state agency called the Committee for Public Counsel Services (CPCS). As noted below, the CPCS did not respond to COFAR’s request for that information.
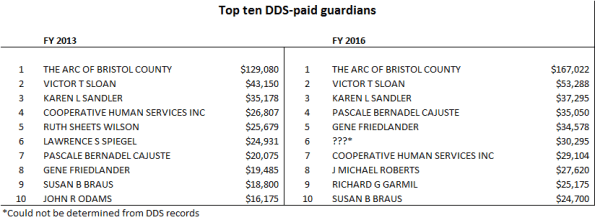
The following chart shows the top-paid DDS guardians in Fiscal Years 2013 and 2016:
COFAR considers becoming a guardian to be a critically important step for family members when loved ones with intellectual and incapacitating developmental disabilities reach the age of 18. After an individual reaches that age, only that person or a guardian acting on their behalf has legal standing to make decisions about their care in the DDS system.
Anyone wishing to become a guardian of a developmentally disabled or otherwise incapacitated person must apply to the probate court to do so. When DDS wishes to pay an attorney to serve as a professional guardian of an individual, it recommends to the court that the attorney be appointed as the guardian.
Under probate law, there are no specific qualifications required of professional guardians such as expertise in mental health issues.
Information about professional guardians and attorneys difficult to obtain
Information about what professional guardians and attorneys do for the clients they are paid to represent in the probate system can be difficult or prohibitively expensive to obtain from DDS and particularly from the CPCS.
Because the CPCS is technically a part of the judicial branch of government, it is not subject to the state Public Records law, according to an attorney we consulted with the state’s Public Records Division. The CPCS would not provide COFAR with any information about the attorneys they employ or the amounts paid to them.
DDS did provide us with a list of guardians it employs and payments made to them, in response to a Public Records request (see chart above showing the top 10 highest paid guardians in Fiscal 2013 and 2016). However, the Department said it would have to pull records from “multiple offices” in order to determine what those guardians do for their payments and how many clients they represent. That information would cost us $3,000, a department attorney wrote.
The DDS payment data also raised a number of questions that the Department did not answer. For instance, there was no guardian listed as the recipient of payments totaling $30,295 on the DDS list in Fiscal 2016. DDS stated that it had no records indicating who those payments may have gone to. (See payment chart above with “???” notation.)
DDS’s response indicates that the department does not have a centralized accounting system to keep track of invoices submitted by guardians for payment. (It appears that this money comes from the clients’ individual Medicaid accounts, but is paid through DDS.)
Independent guardianship office proposed to address accountability issues
In one apparent effort to address at least some of the accountability issues with the current system, a bill in the Legislature (H. 3027) would establish an independent agency called a “Public Guardian,” which would have centralized authority over the hiring and payment of guardians in cases in which family members are not available to serve as guardians of incapacitated people. Under the bill, the Public Guardian would take over the responsibility from agencies such as DDS of recommending and paying guardians.
While COFAR supports the concept of an independent public guardian, we are concerned that H. 3027 specifies that the public guardian would not actually be a public agency, but rather would be a nonprofit agency. We believe the public guardian should be a public agency, which would be subject to the state Public Records Law and other legal requirements that apply to public agencies.
COFAR also strongly supports a second reform measure (H. 887), which would boost the rights of families in the DDS/probate system. The bill would require probate court judges to presume that the parents of incapacitated persons are the suitable guardians for those persons. The measure, however, has never gotten out of the Judiciary Committee.
Payments to guardians on the rise
The list provided by DDS of guardians it employs shows that the department’s total payments to guardians increased between Fiscal 2013 and 2016 from $602,474 to $800,476 – a 33% hike. The number of paid guardians rose from 68 to 80.
The highest-paid guardian was actually a corporate provider – The Arc of Bristol Country — whose total payments rose from $129,000 to $167,000 from Fiscal 2013 to 2016, a 29% increase. The payments to the Arc constituted more than 20%, or one fifth, of the total payments to all guardians in Fiscal 2016.
The second highest-paid guardian in both years was Victor Sloan, an attorney in Uxbridge. His payments from DDS rose from $43,150 in Fiscal 2013 to $53,288 in Fiscal 2016. Sloan’s website lists him a practicing attorney who does criminal defense cases and estate planning in addition to guardianships.
In email messages to Sloan and Michael Andrade, the CEO of the Arc of Bristol County, COFAR asked how many developmentally disabled clients they represented as guardians and how often they were able to visit those clients. In the case of the Arc, we asked how large their staff of guardians was and whether there was a maximum number of persons for whom each member of their staff was allowed to provide services.
Neither Sloan nor Andrade responded to our email or to a follow-up message left with each of them.
The DDS records show that payments to some guardians actually dropped between Fiscal 2013 and 2016, implying that they had lost wards. However, other guardians saw large increases in their payments, which sometimes doubled or even tripled or more in that period. For instance, payments to a Patrick Murray rose from $3,025 to $15,860 from 2013 to 2016 – a 424% increase.
In the Barr case (noted above), payments to the guardian, Dorothy Wallace, rose from $13,000 in Fiscal 2013 to $20,100 in Fiscal 2016 — a 55% increase.
The system appears to reward professional guardians with multiple clients
State regulations governing payments to guardians cap payments per client at $50 per hour, and cap the number of hours that guardians can spend serving individual clients at 24 hours per client per year [130 CMR 520.026 (E)(3)(d)]. Yet, the regulations do not appear to limit the number of clients an individual guardian can represent.
While the regulatory caps would appear to be intended to limit the amount of funding that professional guardians can receive per client, they also appear to provide an incentive to guardians to increase the number of clients they provide services to.
Based on those regulatory caps, we have calculated that Sloan was paid for providing guardianship services to at least 44 clients in Fiscal 2016. The Arc of Bristol County would have had at least 139 clients in that year. When guardians represent large numbers of clients, the ability of those guardians to act in their clients’ interest would appear to decline.
Moreover, the guardianships for which DDS has paid Sloan appear to be only a portion of the probate-court-related work that Sloan does.
Court records show that Sloan has been involved as a guardian, guardian ad litem, attorney, or as a “Rogers Monitor” for incapacitated persons in 118 cases in four separate counties between a seven-year period from Fiscal 2009 to 2015. That includes 14 persons for whom he was appointed as a Rogers Monitor, 75 persons for whom he was appointed as an attorney, 19 cases in which he was appointed as a guardian ad litem, and six cases in which he was appointed as a guardian.
Those six cases in which Sloan was appointed as a guardian appear to be in addition to our estimated 44 cases in which Sloan has been paid by DDS to be a guardian.
An annual client care plan filed in Worcester Probate and Family Court by Sloan does appear to raise questions about the amount of time Sloan spent representing a DDS client from May 2016 to May 2017.
Sloan described the client in the care plan as mildly developmentally disabled and as residing in a group home. Asked on the form to describe the “nature and frequency” of his visits with the client and his caregivers, Sloan stated only that he visited the client and his care givers “at least regularly, and have regular phone and email contact with his residential and day program staff.”
However, stating that he had visited his client “at least regularly” does not either specify the frequency of the visits nor describe their nature.
Sloan’s care plan report contained no critical remarks about the client’s care. He stated that the man’s needs “are being met in his current residential placement,” and that he was attending “an appropriate day program.”
DDS appears to have no centralized accounting system for paid guardians
In a May 10 Public Records law request, we asked DDS for information on the number of clients each paid guardian in its system had and the number of hours the guardians spent with their clients. In a response later that month, a DDS assistant general counsel stated that providing information on the number of clients and hours spent by guardians would require DDS to collect invoices from “multiple DDS offices,” which would take at least 30 hours of “search and collection time” for each of four regional offices. At a cost of $25 per hour, that would cost us at least $3,000, the assistant general counsel’s letter said.
In a subsequent letter sent to us in June, the assistant general counsel stated that it would take an estimated 14 hours of staff time to identify the invoices submitted in Fiscal 2016 from just one guardianship entity — the Arc of Bristol County.
The apparent difficulty that DDS has in locating invoices for payment from guardians in its system raises questions about the adequacy of its internal financial controls, in our view. The DDS central office does not even keep a record of the number of clients each of its guardians represents, according to the assistant general counsel’s May letter.
PriceWaterhouseCoopers notes the importance of centralized, or at least standardized internal controls in large nonprofit institutions such as colleges and universities. We believe a large public agency such as DDS should also have a centralized internal control system, and DDS may lack that with regard to the guardians it employs.
No response from the CPCS
On May 10, we also filed a request with the Committee for Public Counsel Services (CPCS) for a list of attorneys who are selected for appointment to represent clients of the DDS who are subject to guardianship, from Fiscal Year 2013 to the present.
As part of our information request, we asked for a list of the total annual payments made the attorneys from Fiscal 2013 to the present, and the total hours spent each year by those attorneys representing and visiting their clients.
We did not receive a response from the CPCS to our information request. We contacted the state Supervisor of Public Records with regard to the matter and were told that the CPCS is considered to be a part of the judicial branch of state government, which is not subject to the Public Records law.
DDS/Probate system needs reform
As noted, we see a potential conflict of interest in allowing DDS to recommend and pay guardians to represent people in the agency’s care. Along those lines, we are concerned that DDS has in a number of cases recommended attorneys, corporate providers, and other unrelated parties as guardians of individuals over the objections of family members of the individuals.
Also, in light of the increasing amounts paid to guardians by DDS, we are concerned that there is a potential for inadequate representation when paid guardians have large numbers of clients. Yet the payment system for guardians, in particular, appears to encourage those professional guardians to take on more and more clients.
We are also concerned that the system encourages DDS-paid guardians and CPCS attorneys to side together against the interests and wishes of families and individuals caught up in that system.
We think reform of the DDS/probate system is sorely needed, particularly with regard to payment of guardians and other financial practices. Those reforms should make the system more responsive to families, more transparent, and more accountable.
A public guardian may be the answer to many of these issues and problems, but, as noted, we think the public guardian should be just that — public. In the meantime, we urge the Judiciary Committee to finally vote to approve H. 887, which would boost the rights of families in the system by requiring probate judges to presume parents to be suitable guardians.
We will look further into these issues as we advocate for reform of the DDS/probate system.
Isolation of developmentally disabled woman continues after more than a year and a half
It has been a year and seven months since David Barr and his daughter, Ashley, were last informed by the Department of Developmental Services of the whereabouts of David’s other daughter, a young woman with a developmental disability and mental illness.
The 29-year-old woman, whose name is being withheld for privacy reasons, is being kept in an undisclosed residence. All contact with her by her father and sister was cut off for unclear reasons by a DDS-paid guardian in November of 2015.
Although Dorothy Wallace, the DDS guardian, said in August 2015 that her goal was to allow the woman to have family contact, it still hasn’t happened for reasons that have never been revealed to David or Ashley. For unknown reasons, the only family member who has been allowed to visit the woman is an aunt who has apparently agreed not to reveal the woman’s location to the woman’s father or sister.
In an email last week, Ashley Barr told COFAR that her father has personally filed in the Essex County Probate and Family Court to intervene in the case and to seek permission to visit his daughter. But to date, he has not heard from the court.
The probate court has not issued any orders barring visitation with the woman. The denial of virtually all family contact appears to be a decision of the woman’s guardian and possibly DDS.
The Barrs have been unable to afford the cost of hiring a lawyer to pursue their case in probate court. As we have reported in another case, it is extremely difficult to prevail in any probate court proceeding in Massachusetts if you are not a legal guardian or appear without a lawyer.
David and Ashley have contacted their local state legislators, but have gotten little or no help from them. COFAR has attempted to intervene with mainstream media outlets and the legislators in support of visitation for David and Ashley, also to no avail.

David and Ashley Barr
As we reported in January, the Boston-based Disability Law Center temporarily intervened in the case that month to ask a state-appointed attorney who is representing the woman to support family visits if the woman wished that. However, nothing apparently resulted from that effort.
The attorney, Melissa Coury Cote, told COFAR in March that she would not support court permission for visits to the woman by David or Ashley Barr, despite the DLC’s request. She provided no reason to us for opposing family visits other than to say that the woman had not specifically asked her to allow visits from her father and sister.
However, Ashley Barr said that her sister recently called her father on two occasions and said she missed her family and wanted to see them. The calls were apparently unauthorized. Ashley and David don’t know whose phone the woman used to contact them. They are concerned the woman may have gotten in trouble for making the calls.
Coury Cote had previously been appointed by the state Committee for Public Counsel Services (CPCS) to represent the woman on guardianship matters. Under state probate law, incapacitated adults are entitled to free legal representation although their family members are not entitled to that.
COFAR has reported on a number of cases in which DDS-paid guardians have imposed severe restrictions on family contact with persons in the DDS/probate court system; but the Barr case may be the most extreme of those cases in that in none of the other cases has a DDS client been kept in isolation for such a long period of time, and in no other case has their family not been informed of their whereabouts.
COFAR first appealed to DDS Commissioner Elin Howe last October to seek permission for the Barrs to visit their family member, but Howe declined to do so. In early April, COFAR sent an email to Howe, asking whether a timetable existed for ever reuniting Ashley and David with the woman. Howe did not respond to the query.
According to a transcript of an August 2015 court hearing on the case, Wallace and other DDS officials complained that David Barr was excessively combative in dealing with them and that David and Ashley became overly emotional when they had been allowed to visit the woman prior to the cutoff of all contact with her.
While being combative with DDS over the care provided to a loved one can occasionally result in restrictions placed on family contact, we know of no other case in which all such contact was removed for this long a period of time.
CPCS attorney was reportedly told to keep the family informed
John Byron, a friend of David Barr’s, who attended a probate court hearing on the case with David in March, said the probate court judge seemed to be moved when David said he had been prevented from any contact with the young woman and that no one was providing him with any information about her. According to Byron, the judge then told Attorney Coury Cote that she should communicate with the family and that she (the judge) didn’t want the family “kept in the dark” about the case.
Coury Cote told COFAR the judge had asked her during the hearing only to “take a few minutes to speak with father.” She denied that the judge had ordered her to keep David Barr informed about the case. At one point, Coury Cote also said that the Barrs were “not entitled to information” about their family member’s whereabouts.
We believe, however, that in light of a Supreme Judicial Court ruling last year involving the guardianship of a woman known as B.V.G. , David and Ashley Barr should be considered by the probate court to be “interested persons” in the welfare of their family member. As such, they are entitled to information about her whereabouts and to be afforded visitation and other rights.
CPCS declines to review the attorney’s conduct
In March, we appealed to Mark Larsen, director of mental health litigation with the CPCS, asking for an investigation of Coury Cote’s conduct in the case. Larsen responded within two days of our appeal to state that the attorney had no obligation “to follow your directions, those of your client (apparently Ashley and David Barr) or of the DLC. Her only obligation is to her client and her client’s wishes.” He stated that “if the family wants a change in visitation, they should consult counsel of their choosing.”
For the record, neither David nor Ashley Barr are clients of COFAR. COFAR is advocating on behalf of them, but our organization does not charge for such advocacy. Our funding comes strictly from donations made by affiliated organizations and from families.
Larsen also stated that it “appears” that Coury Cote “consulted with her client” in the case.
I wrote back to Larsen to clarify that I had not suggested, or meant to suggest, that Coury Cote should follow our or the DLC’s directions, but that it appeared to us that she “may not have fully ascertained the wishes of her client.” I also stated that Larsen’s comments implied that he did not know for a fact that the Coury Cote had consulted with her client, and that he was only assuming that to be the case.
I noted further that while the CPCS’s Assigned Counsel Manual states that an attorney should “act as a zealous advocate for the client,” the manual also states the attorney should insure “that proper procedures are followed and that the client’s interests are well represented” (my emphasis).
Larsen emailed back a two-sentence reply, badly misspelling my name and saying he had nothing to add to his prior response.
It is frustrating to us, although perhaps not surprising, that the DDS/probate court system seems so often to function against the interests of individuals and families caught up in it. One key reason for this appears to be that there is little or no accountability when professionals in the system act contrary to the interests of people who are powerless and vulnerable.
We always thought the role of legislators and the press was to represent the powerless in society. I think we’re all learning that is no longer the case.
We can only hope that when the Barrs finally do get their day in court, the judge will acknowledge the rights they have been denied and will consider the apparent wish of the young woman involved to see her family again.
In the meantime, we would urge people to call either the governor’s office (617-725-4005) or the DDS commissioner’s office (617-727-5608), and ask them to re-establish family contact in this case. If you do so, please let us know about it.
John Sullivan, founder of COFAR, dead at 97
John L. Sullivan, a founding member of COFAR and a tireless advocate for persons with developmental and intellectual disabilities, died peacefully on Thursday.
Sullivan was also a founding member of the Arc of Massachusetts and was a central figure in class action litigation in the 1970s in Massachusetts that led to improvements in the care of what is now the Department of Developmental Services. Those improvements resulted in upgrades in care and conditions in developmental centers and in the creation of a community-based system of group homes that now serves the vast majority of persons in DDS care.
In March 2012, Sullivan was presented with a lifetime achievement award by the
Department of Developmental Services.
One of Sullivan’s daughters, Jean Sullivan, is intellectually disabled and has been a resident of the Wrentham Developmental Center since 1959. Another daughter, Colleen Lutkevich, has carried on Sullivan’s work on behalf of the developmentally disabled, and has served for many years as the volunteer executive director of COFAR.

John Sullivan
“My dad worked and fought his whole life to make the system work for the least fortunate among us,” Colleen Lutkevich said. “His advice was always, ‘never be afraid.'”
When Sullivan’s daughter, Jean, was a toddler, he and his wife, Gladys, helped found a preschool for disabled children. Gladys died last year after a 71-year marriage to John.
Sullivan later fought for the passage of Chapter 766, the state’s special education funding law, and petitioned local school committees for special education services within area towns.
In the 1970s, while Jean was living in the Wrentham center, Sullivan became a plaintiff in the landmark Ricci v. Okin lawsuit, which was brought to challenge conditions in large institutions in Massachusetts that then housed thousands of individuals.
During that time, Sullivan became a member and then president of the Wrentham Parents Association. He also helped found the Charles River Arc, the Charles River Workshop, and later, three group homes.
Sullivan was a founding and executive board member of the Arc of Massachusetts, and organized one of the organization’s first state conventions. However, he opposed the Arc’s decision to advocate for closure of the developmental centers, contending those facilities should remain as a residential option to individuals and their families needing care.
Sullivan’s disagreement with the Arc’s direction led him to drop his membership in that organization and to found COFAR in 1983.
As he accepted his lifetime achievement award in 2012, Sullivan said he wanted to “pay tribute to the wonderful people that work day in and day out (on behalf of the intellectually disabled). They are the saints on earth.”
He was a veteran of the US Navy, and served for four years in the Pacific during World War II on a minesweeper, the USS Searle, and on a minelayer, the USS Monadnock.
Sullivan grew up in Dorchester and West Roxbury, and spent several years in school at Miramar Seminary in Duxbury, before graduating from Roslindale High School. After the war, Jack and Gladys were married, and moved to Jamaica Plain, then Dedham.
In addition to Jean Sullivan and Colleen Lutkevich, John Sullivan is survived by two other daughters, Joyce Wise and Laura Bradley.
A funeral Mass will be held on Wednesday morning, July 5 at 9:30 a.m. at St. Mary’s Church in Mansfield, with a reception to follow at the Parish Center. Donations in John’s memory can be sent to either the Wrentham Family Association or to COFAR, both c/o Colleen Lutkevich, 3 Hodges St., Mansfield, MA 02048. Donations can also be made online on COFAR’s website at www.cofar.org.
State law that boosted human services funding has helped provider CEOs more than direct-care workers
A 2008 state law, which substantially raised funding to corporate agencies running group homes for people with disabilities, has resulted in only minimal increases in wages for direct-care workers in those facilities, according to a new report from the SEIU Local 509, a Massachusetts state employee union.
Since the law known as Chapter 257 took effect, the average hourly wage for direct-care workers rose by about 14.8 percent to just $13.60 in Fiscal Year 2016, according to the SEIU report, which was released last week (and got little media coverage, btw).
In contrast, the report noted, the law helped boost total compensation for CEOs of the corporate providers by 26 percent, to an annual average of $239,500.
According to the SEIU, raising wages of direct-care workers employed by provider agencies was a key goal of Chapter 257, and yet those workers “are still struggling to earn a living wage” of $15 per hour. The union contended that the funding increases made possible by Chapter 257 “did not come with any accountability measures, leaving it up to the private agencies to determine their own spending priorities.”
The SEIU report found that human services providers in the state received a total of $51 million in net or surplus revenues (over expenses) in Fiscal 2016, which would have been more than enough to raise the wages of all direct-care workers to the $15-per-hour mark. Yet, the providers have chosen not to do so.
Last week, the state Senate approved a budget amendment that would require human services providers to spend as much as 75 percent of their state funding each year in order to boost the pay of their direct-care workers to $15 per hour. The amendment had not been approved in the House, so it will now go to a House-Senate conference committee.
The SEIU report provides confirmation of a report by COFAR in 2012 that direct-care workers in the Department of Developmental Services’ contracted system had seen their wages stagnate and even decline in recent years while the executives running the corporate agencies employing those workers were getting double-digit increases in their compensation.
In January 2015, a larger COFAR survey of some 300 state-funded providers’ nonprofit federal tax forms found that more than 600 executives employed by those companies received some $100 million per year in salaries and other compensation. By COFAR’s calculations, state taxpayers were on the hook each year for up to $85 million of that total compensation.
The SEIU report stated that during the past six years, the providers it surveyed paid out a total of $2.4 million in CEO raises. The highest total CEO compensation in the union’s survey was that of Seven Hills Foundation’s CEO who received a total of $797,482 in Fiscal 2016. Seven Hills received $125 million in state funding that year, with most of that funding coming from DDS.
The SEIU report stated that the average direct-care employee at Seven Hills makes just $12.47 per hour, more than a dollar less than the average wage for workers across all the organizations analyzed in its report.
Vinfen, the third largest provider in the state, provided its CEO with a total of $387,081 in compensation in Fiscal 2016. Vinfen spent a total of $1.7 million on compensation for its top five executives in that fiscal year.
The potential for double-digit increases in CEO compensation was not mentioned by provider-based advocacy organizations that actually sued the then Patrick administration in 2014 to speed up the implementation of higher state funding under Chapter 257.
According to the plaintiffs in the lawsuit, the higher state funding was needed quickly in order to keep up with the rising costs of heat, rent and fuel, and to increase wages to direct-care staff in order to reduce high staff turnover.
In comments in support of the provider lawsuit in 2014, one key provider lobbyist contended that time was of the essence in boosting provider funding. “…Every day that full implementation (of Chapter 257) is delayed, the imbalance and the unfairness grows,” the lobbyist said.
Yet, according to the SEIU, the providers made 3.2 percent, 2.7 percent and 2.3 percent respectively in surplus revenues on average in the Fiscal 2014, 2015 and 2016 fiscal years. The imbalance that existed was actually between executive-level salaries and direct-care wages in those provider organizations.
As a result of the lawsuit, both the Patrick administration and the incoming Baker administration approved major funding increases to the provider-run group-home line item in the DDS budget, even as it was becoming clear the state was facing major budget shortfalls in the 2015 fiscal year.
“This all suggests,” last week’s SEIU report concluded, “that the amount of state funding is not at issue in the failure to pay a living wage to direct care staff, but rather, that the root of the problem is the manner in which the providers have chosen to spend their increased revenues absent specific conditions attached to the funding.”
A look at the struggles of two families to cope with closures of sheltered workshops in Massachusetts
When Massachusetts closed its remaining sheltered workshops for people with developmental disabilities last summer, deeming the programs “segregated,” the impact of the closures on workshop participants Mark Garrity and Danny Morin was pretty much the same.
The two men continued to go every day to their respective facilities where their sheltered workshops had formerly been operated by providers funded by the Department of Developmental Services. But while the providers continued to manage the same facilities, each provider now began offering their clients traditional, DDS-funded day program activities instead.
Paid piecework and assembly work that had been given to Garrity and Morin to do in their sheltered workshops were taken away and replaced by day program activities that they couldn’t relate to. In each case, their provider agency managed to come up with a makeshift solution to the problem that allowed the men to continue doing work similar to what they had done before.

Patty Garrity and her brother, Mark Garrity
But in each case, the solutions were implemented despite a lack of clear, written standards or guidance from the federal and state governments on the type of work and activities that were now permitted for the men. Their family and guardians were confused as well, often having to rely on information passed along from program staff or family of other clients.
Even some providers acknowledge that the system functioned more smoothly for everyone when the providers were operating their programs as sheltered workshops. At that time, participating companies would ship materials to the providers, and everyone at the workshop sites would have work to do — usually simple assembly jobs or packaging or labeling tasks.
Now, those providers must either send their clients to companies that offer to provide “integrated” work for them, or must try to continue to provide some on-site work under unclear rules that sometimes result in work arrangements that are adopted verbally and on a case-by-case basis. Moreover, most of their clients are now offered only day program activities that do not involve productive work and do not pay anything.
For Barbara Govoni, the mother of Danny Morin, and for Patty Garrity, the sister of Mark Garrity, the sheltered workshops were not only easier for them to deal with, they provided meaningful and satisfying activities for their respective loved ones.
“My argument is whether it was federal or state, they should not have taken away the workshops for those who can’t function in the community and disrupted their lives,” Govoni said. “I’m not opposed to finding jobs in the community or expanding day programs. I get it all has to do with money, but I feel that a group of people are being discriminated against based on the fact they had no voice or vote. They have been taken out of their element where they were comfortable.”

Barbara Govoni and her son, Danny Morin
Govoni views the policy of providing integrated employment to all developmentally disabled people as a “misguided one-size-fits-all” approach to a complex social need.
State cites federal pressure to close workshops
All sheltered workshop programs were closed in Massachusetts as of last summer as a result of requirements by the federal Centers for Medicare and Medicaid Services (CMS) that developmentally disabled people work in “integrated employment” settings in which a majority of the workers are not disabled, and that they be paid the minimum wage in those settings. Sheltered workshops were deemed “segregated” settings because they were offered solely to groups of developmentally disabled persons, and the clients were often paid only a nominal amount for the work they did.
In Massachusetts, the Baker administration claimed it had no choice but to follow the CMS rules and close all of the workshops in the state, or else the federal government would bring a lawsuit against them. But many other states have apparently not acted in the haste that Massachusetts did in shutting the programs down. DDS Commissioner Elin Howe stated late last year that Massachusetts was one of the first states in the country to close all of its workshops.
DDS and its major policy advisors, the Arc of Massachusetts and the Association of Developmental Disabilities Providers (ADDP), had actually wanted to close all of the sheltered workshops in Massachusetts as early as June of 2015. But in the wake of strong protests by families of workshop participants, the state Legislature temporarily slowed the closure process by inserting budget language in fiscal years 2014 and 2015, stating that DDS must continue to make sheltered workshops available for those clients who continued to want them.
But at the same time, the Legislature approved funding for the transfer of the participants out of the workshops and into day programs or employment programs. That move ultimately allowed the workshops to close while enabling legislators to claim they had acted to save the programs.
The closures of the sheltered workshops in Massachusetts resulted in the removal from those programs of close to 2,000 participants, but those closures do not appear to have translated into a steady flow of people into integrated employment.
Verbal permission given for on-site work
At the Road to Responsibility day program site in Braintree, which Mark Garrity attends, I met in late March with Patty Garrity and with senior staff of the provider and DDS officials to discuss Mark’s experience in making the transition from his sheltered workshop to the new system.
Like Barbara Govoni, Patty Garrity said the transition from the sheltered workshop has been difficult. Before RTR ceased operating as a sheltered workshop, Mark did a range of activities there, including collating, packaging, and other production work.
For months, after the workshop was closed in September of 2016, Mark was frustrated and angry, Patty said. RTR provided day program activities for him, but, as Patty put it, they “went over his head.” He wasn’t interested in nature walks or painting or cooking. In particular, he didn’t understand the class on money management.
In addition to his intellectual disability, Mark Garrity had suffered a traumatic brain injury in 1995 after having been hit by a car. He underwent years of rehabilitation from that accident, which had nearly killed him.
In a letter written before Mark’s sheltered workshop program was ended, Mark’s neurologist, Dr. Douglas Katz, a member of the Department of Neurology at Boston Medical Center and a professor at the Boston University School of Medicine, stated that participating in the workshop had been “an important part of his (Mark’s) rehabilitation effort…and…his life before his injury. It is an activity that is highly rewarding for Mark. He looks forward to it on a daily basis.”
Katz added that, “I understand this program is …likely to close because of new rules passed by the CMS. I think this would be a big loss for my patient Mark. I would support efforts to maintain this structured workshop for Mark and others that benefit from this service.”
As of March 2 of this year, when I first talked to Patty, RTR still had no work for Mark to do that was similar to the work he had done prior to RTR’s changeover from a sheltered workshop to a day program site. But as of March 20, RTR officials said they had found paper shredding work for Mark for two out of the four hours a day that he attended the program.
The paper shredding arrangement at RTR was done after DDS southeast regional director Richard O’Meara determined that it would not violate the CMS rules. O’Meara said the permission he gave to RTR to offer paper shredding to Mark was purely verbal. There was nothing placed in writing about it.
Hearsay information on piecework eligibility requirement
In January 2016, Govoni said, the Agawam-based Work Opportunity Center, her son’s former sheltered workshop provider, temporarily operated day programs in a function room in a local church after having closed its sheltered workshop program. “I walked in there one day (the temporary day program site),” she said, “and it appeared chaotic, with no structured activities.”
All of the Work Opportunity Center’s clients are now back at the agency’s facility. Govoni’s son gets sent out occasionally to integrated work sites and has some piecework to do at the Work Opportunity site as well. But the work is intermittent. She said she has also heard that those who want to do piecework at the Work Opportunity location will have to take a class explaining what piecework involves.
However, once again, Govoni said she has received nothing in writing about the reported class. She heard about it “through the grapevine.”
In the meantime, Govoni’s son receives a schedule of activities every month at the Work Opportunity Center. “I’m not saying it’s bad,” Govoni said, “but it’s not what he is interested in.” She said many of the activities are educational, such as lectures on geography or cooking demonstrations. Volunteer work is available as well at a local homeless shelter, and residents are taken on walks to the local library and other locations. “Danny doesn’t want to do that,” she said. “He wants to work.”
Both Govoni and Patty Garrity said Danny and Mark respectively didn’t care about making the minimum wage, and would rather work at their day program sites than get sent out to jobs in the community.
Disagreement over client and family satisfaction
If, like Barbara Govoni and Patty Garrity, family members are confused or dissatisfied by the current situation, O’Meara said, they aren’t letting him know about it. O’Meara said that he and DDS Area Director Colleen Mulligan, who was also in attendance at the March 20 meeting at RTR, are generally the first people whom family members and guardians call when there are problems with DDS care.
“I haven’t gotten a lot of complaints (about the closures of the sheltered workshops in his region),” O’Meara said. “Generally, if people are not happy, we know about it. These issues are addressed through the ISP (Individual Support Plans). I haven’t had many calls.”
Mulligan added that if problems were occurring like the ones Garrity has described, “I’m not hearing about it.”
But Garrity and some other advocates believe there may be few complaints now because the vocal protests that did occur when the workshop closures were first announced largely died down when families and guardians saw that their protests were having little effect.
A debate over integrated employment
At RTR, Chris White, the agency’s chief executive officer, maintained that even if the CMS requirements have been difficult to comply with, the requirements make sense because he believes that “everyone is capable” of working at integrated employment sites.
White’s viewpoint is in line with an August 2010 DDS policy document that states that “it has now been clearly demonstrated that individuals who were previously considered unemployable in integrated community settings can work successfully.”
But Govoni and Garrity maintained that the ideological viewpoint that the workshops segregated their participants and that integrated employment is feasible for everyone does not apply in their cases. “My son couldn’t wait to go to work (at his former sheltered workshop),” Govoni said. “He was not discriminated against. It was not a sweatshop for him, but the opposite. He doesn’t thrive in integrated sites. He would much prefer staying at the workshop where he was more comfortable. He doesn’t care what he gets paid.”
Govoni said that efforts to place her son in integrated work settings often did not work. In one case, she said, Danny was not able to do the work fast enough to satisfy the employer, and was terminated from the job. The speed of his work did not matter in the sheltered workshop.
Moreover, Govoni and Garrity maintained that even if integrated employment arrangements were feasible for everyone, there are not enough such jobs available to fulfill the demand now that the sheltered workshops are no longer available.
White said there were about 109 clients at RTR who were involved in “integrated group employment” at various job sites. That number was expected to rise this spring to about 120, he said.
At the same time, some 200 clients remained in RTR’s day program. White maintained, however, that those clients were happy with the activities they were doing, and that some were “on a retirement track.”
But it may be an open question whether all or most former workshop clients are really happy in day programs, or whether they simply have no choice but to remain in them.
Even DDS Commissioner Elin Howe appears to acknowledge that the state and its providers have been unable to find mainstream workforce jobs for a significant number of former workshop participants. While Howe made public remarks last year that we believe painted an overly rosy picture of the integrated employment situation, she did acknowledge that “many people transitioned (from sheltered workshops) to Community Based Day Support programs,” although she did not say how many.
Meanwhile, the Legislature has slowed funding for the transition to integrated employment. In order to carry out the administration’s integrated employment policy, the Legislature initially increased funding of the community-based day program line item in the state budget, and created a new line item to fund the transfers from the sheltered workshops. The idea was to increase both day program and job development staffing and training.
The new sheltered workshop transfer budget line item was initially funded in Fiscal 2015 with $1 million. That amount was raised to $3 million in Fiscal 2016, and the governor proposed to boost it to $7.6 million in Fiscal 2017. But the House and the Senate did not go along with the governor’s plan. The Legislature level-funded the line item for Fiscal 2017. The line item was not included in the governor’s budget for Fiscal 2018.
We agree with Garrity and Govoni that the case has not been made that integrated employment is suitable for all people with developmental disabilities, and it is apparent that not enough integrated work opportunities even exist for all of those that could benefit from it.
We think the federal government needs to rethink its flawed ideology regarding sheltered workshops, particularly the questionable claim that they are discriminatory and segregate their participants. The experience of Mark Garrity and Danny Morin provide further evidence that that claim is untrue.
MassHealth audit casts doubt on claimed savings in privatizing state services
Last year, State Auditor Suzanne Bump approved a proposal to privatize mental health services in southeastern Massachusetts after the for-profit Massachusetts Behavioral Health Partnership (MBHP) claimed it could save $7 million in doing so.
The auditor’s review under the Pacheco Law required Bump’s office to compare the proposed costs of privatizing the services with continuing to carry them out with state employees in the Department of Mental Health.
In a report released yesterday, the auditor maintains that MassHealth, the state’s Medicaid administration agency, made questionable, improper, or duplicate payments to MBHP totaling $193 million between July 2010 and 2015. Those allegedly improper payments appear to have been made under the same contract with MBHP that served as the vehicle for privatizing the mental health services last year.
Under that umbrella contract, known as the Primary Care Clinician Plan, MassHealth paid MBHP more than $2.6 billion between 2010 and 2015.
Given the finding that MassHealth’s total payments to MBHP include $193 million in questionable, improper, or duplicate payments, it would seem it has just gotten harder to argue that privatization of human services has been a great deal for the state.
In fact, it seems possible that one of the reasons MBHP was able to offer bids from two providers for privatizing the mental health services that were $7 million lower than what the state employees could offer was that the company knew it could more than make the money back in duplicate payments from MassHealth.
A description of the MBHP billing arrangement by the state auditor paints a picture of the company as a middle-man between MassHealth and providers of actual services under the Primary Care Clinician Plan (PCCP) contract.
According to the audit, the Commonwealth pays MBHP a fixed monthly fee under the PCCP contract for each member enrolled in MBHP. MBHP then “recruits and oversees networks of third-party direct care providers who assume responsibility for providing a range of covered behavioral-health care.” MBHP subsequently “pays the providers using the monthly…premiums received from the Commonwealth.”
MBHP’s real role here appears to be as a pass-through of state funds. What MBHP really seems to add to the process is an apparently large layer of bureaucracy.
We have noted that MBHP is a politically connected company whose parent companies manage the behavioral health benefits of 70 percent of MassHealth members. In April 2015, Scott Taberner, previously the chief financial officer at MBHP, was named Chief of Behavioral Health and Supportive Care in MassHealth.
As we pointed out, Taberner was put in a position to manage the contract with the company he used to work for.
State employee unions, including the Service Employees International Local 509, the Massachusetts Nurses Association, and the American Federation of State, County, and Municipal Employees Council 93 did challenge Bump’s initial approval of the privatization arrangement with MBHP last year for the southeastern Massachusetts mental health services.
The unions maintained that the lower bids submitted for the privatization contract assumed major cuts in staffing at mental health facilities in southeastern Massachusetts, which would be likely to result in lower-quality services. They argued that the Pacheco Law requires that service quality not be affected.
The Pacheco Law requires a state agency seeking to privatize services to submit to the state auditor a comparison of a bid or bids from outside contractors with a bid from existing employees based on the cost of providing the services in-house “in the most cost-efficient manner.” If the state auditor concurs that the outside bidder’s proposed contract is less expensive and equal or better in quality than what existing employees have proposed, the privatization plan will be likely to be approved. If not, the auditor is likely to rule that the service must stay in-house.
In December, the state Supreme Judicial Court upheld Bump’s Pacheco Law review.
An SEIU official said to us yesterday the union is reviewing the auditor’s latest audit. We think that at the very least, the audit calls into question the savings claim in privatizing the southeastern Massachusetts mental health services.
More broadly, the audit of the MassHealth-MBHP contract calls into question MassHealth’s system of internal controls in managing state’s $13 billion Medicaid program.
It appears the MassHealth internal control system is so inadequate that the administration was unaware that hundreds of millions of dollars in improper payments were being made to its major contractor. Yet the administration was eager to reward MBHP’s efforts to eliminate state employees and cut staffing for mental health services in order to save a reported $7 million.
The MassHealth-MBHP debacle should serve as a warning to legislators and others that privatizing state services is not an automatic panacea to problems in service delivery and to high costs. Privatization comes with potentially high costs of its own, particularly when the state forsakes its role, as it appears to have done in this case, of adequately managing and overseeing its contracts with service providers.
Data show a recent decline in the developmentally disabled population in state-run residential care
Data provided by the Baker administration show that the number of residents in remaining state-run residential programs for the developmentally disabled has begun to decline, raising questions about the state’s policy for the future of state-run services.
The data, which were provided under a Public Records Law request, indicate that the previous fiscal year (2016) may have been the peak year for the residential population in state-operated group homes and the Wrentham and Hogan developmental centers.
The graph below, which is based on the DDS data, shows the number of residents living in state-operated group homes each year since Fiscal Year 2008:

As we have frequently pointed out, the administration appears to have placed a priority on funding privatized residential services offered by corporate providers to the Department of Developmental Services. A question remains, however, as to whether the administration’s policy also entails phasing out state-operated care.
While Governor Baker’s Fiscal 2018 budget proposes $59.9 million in additional funding for privatized group homes, his budget proposes a $1.8 million cut in the state-operated group home account. That would amount to a $6.9 million cut in that account when adjusted for inflation.
Similarly, the governor is proposing a $2.4 million cut in the state-run developmental centers line item. That’s a $4.9 million cut when adjusted for inflation.
DDS operates or manages both state-run and privatized systems of residential care in Massachusetts. The state-run system, which is now much smaller than the privatized system, includes the two remaining developmental centers and the state-operated group homes.
The ultimate elimination of state-run residential services would take away a key element of choice for individuals and families in the DDS system. State-run residential centers and group homes provide residential care to some of the most profoundly disabled persons in the commonwealth, and they tend to employ staff with higher levels of training and lower rates of turnover than do corporate-run facilities.
COFAR has sent a follow-up Public Records request to DDS, seeking any policy documents that concern the future of state-operated care in Massachusetts.
The administration of then Governor Deval Patrick began closing the remaining developmental centers in Massachusetts in Fiscal 2008, reducing the number of those federally overseen facilities from six to two. Most of the residents in the now-closed developmental centers were transferred either to the Wrentham center or to state-operated group homes, leading to an initial surge in the residential populations in those facilities. But those residential population numbers now appear to be dropping.
According to the DDS data, the number of residents in state-operated group homes rose from just over 1,000 in 2008, when four of the six developmental centers were targeted for closure, to roughly 1,150 in Fiscal 2016. As of the current fiscal year, that number had dropped to about 1,130.
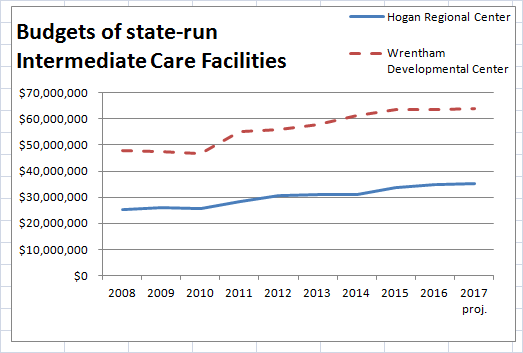
As the graph below shows, both a population surge and drop-off have also occurred at the Wrentham Developmental Center since Fiscal 2008:

The DDS data appear to provide further confirmation of COFAR’s contention that state-run residential facilities are not being offered as residential choices to persons waiting for residential care in the DDS system. We believe that if those facilities were routinely offered as choices, the number of residents in them would either continue to rise or remain steady, but would not be declining.
If DDS is failing to offer state-run group homes and developmental centers as options to people waiting for residential care, that situation would appear to be in violation of federal laws, which require that all available services be offered as options.
The Home and Community Based waiver of the Medicaid Law (42 U.S.C., Section 1396), requires that intellectually disabled individuals and their guardians be informed of the available “feasible alternatives” for care. In addition, the federal Rehabilitation Act (29 U.S.C., Section 794) states that no disabled person may be excluded or denied benefits from any program receiving federal funding.
We think the DDS data closely track the closures of the Fernald, Monson, and Glavin developmental centers, starting in Fiscal 2008, and the transfer of the residents of those facilities primarily to the state-operated group homes and the Wrentham center.
But as we reported in 2014, while 49 new state-operated group homes were built between 2008 and 2014, 28 state-operated homes were closed during that period. The new state-operated homes appear to have been intended to accommodate only the residents of the homes that were being closed and the residents transferred from the developmental centers.
Nevertheless, an undisclosed number of disabled individuals are reportedly waiting for residential services in Massachusetts, although the state does not maintain an official waiting list that would publicly identify the number of people waiting. The Massachusetts Developmental Disabilities Council has continued to cite a 2010 survey indicating that some 600 people were waiting for residential services in the state, and up to 3,000 people were waiting for family support services.
As noted, the administration appears to be attempting to meet the demand for residential care by boosting funding to corporate residential providers. While that hasn’t prevented the budgets of state-run developmental centers from increasing, those budgets may be leveling off.
The DDS data, which includes information about the Wrentham and Hogan developmental center budgets, shows increases in those budgets between Fiscal 2008 and 2015. Wrentham’s budget, in particular, appears to have leveled off, starting in Fiscal 2015.
It is unclear if or when the administration intends to phase out state-run DDS residential care, but the initial data are cause for concern. If you have a loved one in a state-run facility or are seeking care in a state-run setting, please let your local legislators know about this situation.
You can find your legislators at this link.
Harvard researcher looks for the key to understanding the link between Down syndrome and Alzheimer’s disease
The link between Down syndrome and Alzheimer’s disease has become the subject of increasing scientific interest, and a major new study is seeking to shed further light on that connection.
Dr. Florence Lai of Harvard University, McLean Hospital in Belmont, and Massachusetts General Hospital, is the lead Massachusetts investigator in a multi-center, five-year study funded by the National Institutes of Health.

Dr. Florence Lai
In an interview with COFAR, Dr. Lai said the study is seeking “biomarkers” that may predict the onset of Alzheimer’s disease and enable researchers to learn more about Down syndrome. It is intended to be “the most comprehensive study of the links between Down syndrome and Alzheimer’s disease up to this point.”
Lai and her colleagues, Dr. Diana Rosas, a neurologist, and Dr. Margaret Pulsifer, a psychologist, are in charge of the Massachusetts portion of the study.
While the average person with Down syndrome develops symptoms of Alzheimer’s disease in their early 50’s, some may not develop the dementia until the age of 70, and a very few escape it altogether.
“The study seeks, among other things, to learn the reasons for that variation,” Dr. Lai said.
The Massachusetts General Hospital’s facility at the Charlestown Navy Yard is one of seven sites around the country and England that are coordinating their research efforts as part of the study. The other sites include Columbia University (New York City), the University of California Irvine, the University of Pittsburgh, Cambridge University (UK), the University of Arizona (Phoenix), and the University of Wisconsin (Madison).
The NIH study represents a natural progression in Dr. Lai’s clinical practice and research. Over several decades, she has evaluated and followed some 750 individuals with Down syndrome, including Joanna Bezubka, a cousin of COFAR Board member and former president, George Mavridis. In 2013, Mavridis published a compelling memoir about his experience in caring for Joanna, who died of Alzheimer’s disease in 2012 at the age of 60.

George Mavridis and Joanna Bezubka on Joanna’s 60th birthday. Joanna, who had Down Syndrome, died in 2012 at the age of 60 of Alzheimer’s Disease. She had been one of Dr. Lai’s clinical patients.
In a recent letter to Mavridis, Lai said that her hunch that women with Down syndrome who developed menopause early were more likely to develop Alzheimer’s disease earlier, led to an earlier multi-year NIH study by a colleague who proved the hypothesis.
Another hunch of hers that immunological factors in Down syndrome might be involved in Alzheimer’s disease is now the subject of intense scientific interest with many researchers concentrating on neuro-inflammation as a causative factor.
Those avenues of inquiry “may pave the way to think outside the box for potential treatments for AD (Alzheimer’s disease),” Lai wrote to Mavridis.
In her interview with COFAR, Dr. Lai said scientists have discovered that people with Down syndrome are genetically predisposed to create large concentrations in their brains of amyloid protein, which is connected with destruction of brain cells in Alzheimer’s disease.
The gene for the precursor of amyloid protein is located on Chromosome 21. Since people with Down syndrome have an extra copy of Chromosome 21, Dr. Lai explained, they “make the amyloid earlier and more of it. That may be the reason for the high incidence of Alzheimer’s disease in people with Down syndrome.”
In order to learn more about the impact of the amyloid protein and other potential biomarkers of Alzheimer disease, the NIH study is designed to collect a broad range of information from the participants in the study, including information on their health history, cognitive functioning, immune and genetic factors, and daily living activities. The information is obtained from cognitive testing, from blood samples that are sent to specialized labs around the country, and from caregivers of the participants.
The study also includes an MRI brain scan of the subjects and an optional PET scan (Positron Emission Tomography), which involves the introduction of a small dose of radioactive material to examine the presence of amyloid protein in the brain. Another optional part of the study includes analyzing the cerebral spinal fluid obtained from a spinal tap.
The 3-year NIH study is limited to adults over the age of 40 with Down Syndrome at three of the sites (including Charlestown) and over age 25 at the other four sites. At the MGH Charlestown site, the study involves three cycles of visits with each cycle involving two to three visits of up to five hours each. The second and third cycles each take place 16 months after the previous cycle.
Although the study was initially funded in September 2015, it took about a year to “harmonize the procedures at all the sites,” Dr. Lai said, and to receive the necessary approvals from the participating institutions including the Research Review Committee of the Department of Developmental Services in the case of Massachusetts. Lai said the researchers at the seven study sites hope to recruit up to 700 individuals to participate in the study.
Lai said that although the NIH authorized the multi-million dollar study in 2015, the federal agency recently announced that it will be forced to cut some of the funding. She noted that the study is expensive to perform. A large number of specialized personnel is needed, and doing the brain scans is “very costly.”
At the MGH site, about 20 participants have been recruited so far and have been through a preliminary visit, Lai said. They receive a modest payment for their participation. The information collected is anonymous, she said. Even the researchers analyze only coded, aggregate data.
Continuing to treat Down Syndrome patients
Apart from the NIH study, Drs. Lai and Rosas continue to clinically treat, test, and follow the life histories of patients with Down syndrome at McLean hospital. They see each patient once a year and generate neurological evaluations which are shared with caregivers and family.
Lai has collected hundreds of blood samples, some of which have been stored at a Harvard-affiliated facility at -80 degrees C. However, the samples have lain dormant for many years due to a lack of funding needed to analyze them. Lai noted that many of her colleagues have experienced the same funding frustrations, and have had to supplement federal funding with industry grants and philanthropic donations.
It was actually due to the generosity of several families of her patients, Lai said, that she herself was able to start a Down Syndrome Fund for Alzheimer Research at MGH. The Fund got a boost of several thousand dollars a few years ago when a member of the MGH Board of Directors called Lai to thank her for her care of a patient with Down syndrome whom he knew personally.
Lai said that if the Down Syndrome Fund ever does get more sizeable contributions, her “dream” is to team up with colleagues to fully analyze the stored blood samples, and “to encourage a younger generation of clinicians and investigators to devote their energies to care for and study those with Down syndrome.”
Persons interested in learning more about the NIH study at MGH can call 617-726-9045 or 617-724-2227.
Those interested in an evaluation and follow-up with Drs. Lai and Rosas at the McLean Hospital Aging and Developmental Disabilities Clinic can call 617-855-2354.
Dental practitioner bills could undercut care of the developmentally disabled
Sometimes even well-intentioned bills in the Legislature can have unintended impacts, and we’re concerned about two such bills that authorize mid-level dental practitioners to perform basic dental procedures in order to address under-served populations around the state.
Versions of one of the bills are being promoted in several states, including Massachusetts, by the Pew Charitable Trusts. The second bill is being promoted by the Massachusetts Dental Society.
While we appreciate the intent behind the bills, we are concerned that passage of either one as currently written could actually result in the loss of existing services to clients of the Department of Developmental Services.
If either bill is enacted, many DDS clients, who are currently served by experienced dentists, could be switched by the administration to less skilled and experienced practitioners as a money-saving measure.
Backers of the Pew Trusts bill (S. 1169) point out that large numbers of adults and children in this and other states around the country are unable to access dental care either because they live in under-served areas or because only about a third of U.S. dentists accept publicly provided health insurance.
Under S. 1169, practitioners known as “dental therapists” would work under supervisory agreements with dentists, and would be authorized to do such things as fill cavities, extract teeth, and apply crowns. While this may work well for patients in the general population, we don’t think it is workable for many people with developmental disabilities who require dentists with advanced skills and significant experience.
As such, we would not support either S. 1169 or the competing bill from the Massachusetts Dental Society (S. 142) unless either bill contained language specifying that dentists must continue to treat persons with developmental disabilities.
The primary sponsors of S. 1169, Senator Harriette Chandler and Representative Smitty Pignatelli, maintain that hundreds of thousands of children covered by Masshealth in Massachusetts do not regularly see a dentist.
However, it has apparently not been as difficult to find a dentist for people with intellectual and developmental disabilities (ID/DD). Right now, the availability of dental services to persons with ID/DD appears to be quite high in Massachusetts. The Massachusetts Developmental Disabilities Council’s (MDDC) State Plan for Fiscal 2017 states that between 90% and 97% of DDS clients have continued to receive annual dental exams.
Some 7,000 developmentally disabled persons in Massachusetts receive dental care in seven state-funded clinics run by the Tufts University School of Dental Medicine. Pediatric dentistry is offered by Franciscan Hospital for Children.
Despite that high level of service provision, we have seen in the past that administrations have proposed elimination of some of the Tufts clinics in order to save money. Strong opposition from families of DDS clients helped to preserve at least one such clinic temporarily at the now closed Fernald Developmental Center, but that clinic was ultimately closed.
Our concern is that as currently written, either S. 1169 or S. 142 might actually give the Baker administration an excuse to reduce funding for the Tufts clinics because those clients could now presumably be served by the dental therapists or hygienists, as authorized by the legislation. If that is the case, there could be an increasing impetus to close additional Tufts facilities for those clients.
Moreover, while S. 1169 requires that the dental therapists receive training in treating people with ID/DD, the therapists would certainly not have the expertise or experience of the dentists in the Tufts clinics. The bill actually doesn’t specify the amount of training the dental therapists would be required to receive.
The Tufts Dental school declined to comment on either bill. Dentists themselves in Massachusetts oppose S. 1169, arguing that it does not provide for sufficient training of the dental therapists or direct supervision of them in all cases. The dentists also fear the use of dental therapists could lead to reduced reimbursement rates from insurance companies.
The Dental Society’s bill (S. 142) would establish more stringent educational and supervisory requirements regarding mid-level practitioners than does S. 1169. The Dental Society bill would require, for instance, that mid-level practitioners, which S. 142 refers to as public health dental practitioners, be under the direct, on-site supervision of a dentist at all times.
If either bill does pass, we would urge that language be added to prohibit the dental therapists or public health dental practitioners from having authorization to treat people with ID/DD unless an individual’s guardian specifically requested it.
We think that language along those lines would potentially protect existing dental services for people with ID/DD. Allowing guardians to request the therapists or public health dental practitioners would keep those options open if full dental services were not available for a developmentally disabled individual.
We emailed a Pew Charitable Trusts dental campaign officer on February 17 to express our concerns about the S. 1169, but have not as yet received a response from him.
Last week, I also contacted a legislative aide to Senator Chandler, who defended S. 1169, contending that it would would not result in reduced services to persons with ID/DD, but would “strengthen Tufts” and allow them to provide the same services at a “slightly lower cost.”
The aide said he would convey our concerns to Senator Chandler and would try to arrange for someone from Pew to get back to us with their response to our concerns. As noted, that hasn’t happened yet.
No one from Rep. Pignatelli’s office has yet responded to an email we sent early last week.
S. 1169, which currently has 30 co-sponsors from the House and Senate, has been referred to the Legislature’s Public Health Committee. Please call the Committee at (617) 722-1206 and urge them to insert language into the legislation to prevent dental therapists from treating people with developmental disabilities unless a guardian requests that. Or you can email the co-chairs of the Committee — Senator Jason Lewis ( Jason.Lewis@masenate.gov) and Representative Kate Hogan (Kate.Hogan@mahouse.gov).
The Massachusetts Dental Society’s bill (S. 142) has been referred to the Consumer Protection and Professional Licensure Committee. That bill should also be amended to include our protective language. Please call that Committee at(617) 722-1612. Or you can email the co-chairs — Senator Barbara L’Italien (barbara.l’italien@masenate.gov) and Representative Jennifer Benson (Jennifer.Benson@mahouse.gov).
