Archive
Limited federal IG probe faults state’s reporting on group home abuse in MA
In one of the few investigations of the community-based system of care for the developmentally disabled, the Inspector General for the U.S. Department of Health and Human Services last week disclosed critical shortcomings in the process in Massachusetts for reporting abuse and neglect.
A report issued by the IG found that incidents of abuse and neglect in group homes were not regularly reported to investigators. The report noted that of a sample of 587 visits by group home residents to hospital emergency rooms, the group homes had failed to report 88 –or 15 percent — of them to the Department of Developmental Services.
In addition, DDS itself and the group homes did not report 58 percent of 175 “critical incidents” to the Disabled Persons Protection Commission, as required by state regulations. And 29 percent of incident reports sampled by the IG did not contain “action steps” to protect individuals involved from future injury.
COFAR has long maintained that the state’s privatized group home system is inadequately overseen and prone to abuse and neglect due to relatively low levels of pay and training, and high turnover among staff. Even the providers themselves acknowledge those problems. Yet the state routinely relicenses the providers to operate homes even though there are clear gaps in the prevention and reporting of abuse and neglect.
The Massachusetts report is the third report issued by the HHS IG thus far on abuse and neglect in individual states. Last year, the IG issued a report on New York State; and in May, the agency issued a report on Connecticut.
U.S. Senator Chris Murphy of Connecticut, who originally requested in 2013 that the HHS IG investigate abuse and neglect in group homes around the country, commented this week on the findings, at least concerning Connecticut and Massachusetts. In a statement issued on Monday, Murphy said he will introduce federal legislation to require reporting of incidents of abuse and neglect, and training of direct care staff in group homes.
Murphy’s office did not respond to a request from COFAR earlier this year for comment on the New York report. As we noted in February, the New York report contained no recommendations and no critical findings, and was only six pages long.
The Massachusetts report, in contrast, was 33 pages long. Like the Massachusetts report, the Connecticut report, which was issued in May, found numerous failures to report abuse and neglect to state authorities.
Despite its thoroughness in examining the incident reporting process in Massachusetts, we believe even the IG’s Massachusetts report was limited in its scope. We think it could have gone much further in investigating the major problems posed by the privatized residential system.
In requesting the IG investigation, Murphy’s 2013 letter to Daniel Levinson, the HHS IG, emphasized the role of privatization in causing “a race to he bottom in our health care system. Privatization of care may mean lower costs but without the proper oversight and requirements for well-trained staff,” Murphy stated.
In limiting its report primarily to findings of failures to report instances of abuse and neglect, the IG has focused on a small piece of the overall problem. The larger issue concerns not only the level of abuse and neglect in the privatized system, but the overall adequacy of care that exists in it.
The HHS IG report did not examine the impact of privatization on the quality of care in the group home system, and did not specify whether the residents whose emergency room visits the IG sampled lived in privatized or state-run group homes.
We have found that the state’s ongoing privatization of residential services has resulted in a corporate, bottom-line approach to care of the disabled. Moreover, DDS has insisted on steering people waiting for residential care to the privatized group home system, all the while failing to provide state-run homes as an option.
The case of Kathleen Murphy is an example. As we have previously reported, Kathleen’s sister and guardian, Patricia Murphy, and members of her family began trying to move Kathleen from a corporate provider-operated group home to a state-operated residence in 1998. DDS continually declined to move her, despite a federal law requiring that the Department provide disabled individuals with a choice among all available alternatives for residential care.
Patricia Murphy finally filed a federal lawsuit in 2013, which resulted in the placement of Kathleen in a state-operated residence. (By way of disclosure, Kathleen Murphy is represented in the case by Tom Frain, who is COFAR’s Board president.)
Patricia Murphy contends that Kathleen suffered nearly 16 years of physical abuse, sexual assaults, emotional torment, and medical neglect in provider-operated group homes. She says her sister was also grossly over-drugged in those facilities, and her clothing, jewelry and spending money were stolen.
The state-operated residence to which Kathleen was finally placed is “the best thing that ever happened to her,” Patricia said. She said that since moving to the state-operated group home, Kathleen has lost 45 pounds, is being fed nutritious food, is off all psychotropic drugs, and her blood pressure is under control.
Yet these experiences as reported by families are apparently of little interest to the federal government, in particular, which, like the state, is committed to further privatization of residential services for the developmentally disabled. While the U.S. Department of Justice has placed a major emphasis in recent years on investigating and closing down state-operated facilities and services for the disabled, there have been few if any comprehensive investigations of the privatized group home system.
Unfortunately, the Massachusetts Legislature has adopted a look-the-other-way attitude regarding these problems. As far as we know, no legislative committee has scheduled any hearings in recent memory on the problem of abuse and neglect in the DDS system.
Both the Legislature and the Baker administration have continued a policy of boosting funding for further privatization of services while slowly starving the much more responsive state-run group home system of budgetary support.
We hope that the IG report, limited as it was, spurs the Legislature to finally pay attention to the big issues that surround the care of persons with developmental disabilities in Massachusetts. Those issues concern privatization and its impact on abuse, neglect, and the quality of care in general.
Gov. Baker’s FY ’17 budget continues race to the bottom in care of the developmentally disabled
In his proposed Fiscal 2017 budget, which he filed last week, Governor Baker is continuing to boost funding for privatized care for the developmentally disabled at the expense of state-run care.
This continues a pattern that has crossed party lines — the Patrick administration did the same thing — of reducing both the available choices and the quality of care for people with developmental disabilities.
Privatization of human services reduces the quality of care because it reduces money spent on direct-care staffing. Direct care workers of corporate providers get lower pay and less benefits than their counterparts in state-run facilities.
Privatization reduces choice in care because it results in the closures of state-run facilities and consequently eliminates them as an option for people who might want that higher level of staffing and care.
Of course, as the linked New York Times article points out, privatizing services doesn’t necessarily result in long-term fiscal savings for state taxpayers. The money saved in hiring lower-paid workers is usually offset by higher costs such as unemployment insurance and by Medicaid and other public assistance for workers earning low incomes. We also believe any savings in privatization is also offset by the often inordinately high compensation provided to executives of the corporate providers.
Yet it appears the Baker administration still believes it will save money in using lower-paid direct-care workers. That seems to be the case with the administration’s proposal to privatize mental health services in southeastern Massachusetts. In that case, the administration appears to be implicitly backing a reduction in wages to direct-care workers after an initial contract period.
Governor’s FY ’17 DDS budget numbers
Here are some of the key numbers in Baker’s Fiscal 2017 budget proposal for the Department of Developmental Services. Note: All numbers below are adjusted for inflation using the Mass. Budget and Policy Center’s CPI index numbers. The CPI numbers show inflation running at about 1.8 percent for Fiscal 2016.
We believe that in order to gauge the level of the administration’s commitment to privatization of services for the developmentally disabled, it’s necessary to compare what has happened and is happening to the corporate provider line item with what happens to other DDS line items.
Here’s how it looks graphically, with more detailed explanation below.

Corporate provider residential line item (5920-2000): This is the main DDS line item supporting privatized services. It has become by far the largest line item in the DDS budget — funding under this line item exceeded $1 billion for the first time in Fiscal 2015.
The governor’s Fiscal 2017 budget would increase the corporate provider line item by $5.9 million, or 0.5 percent, over current-year funding. If the governor’s Fiscal 2017 budget is adopted, this line item will have been increased by $309 million, or 38.6 percent, since Fiscal 2012.
Chapter 257 Reserve 1599-6903: This is a reserve fund created to last year to provide even more funding for corporate providers. The governor’s budget would increase this fund by $5.7 million or 18.6 percent, to $36.2 million.
The following three line items are key indicators of the administration’s commitment to state-run services.
State-run developmental centers budget line item (5930-1000): The governor’s Fiscal 2017 budget would cut this line item by $3.18 million or 2.8 percent from the current-year appropriation. If the governor’s proposal for Fiscal 2017 is adopted, this line item will have been cut by $41.6 million, or 27.5 percent, since Fiscal 2012.
That $41.6 million cut reflects the closures since 2008 of three of six remaining developmental centers.
State-operated Residential line item (5920-2010): The governor’s Fiscal 2017 budget would cut this line item by $212,800, or 0.1 percent, from current-year funding. (In nominal dollars, the governor has proposed a $3.7 million increase in this line item, but it’s a cut when adjusted for inflation.) If the governor’s Fiscal 2017 budget is adopted, this line item will have been increased by $42.8 million, or 24.4 percent, since Fiscal 2012.
That 24.4 percent increase since Fiscal 2012 for state-operated residential care can be compared to the 38.6 percent increase in the corporate provider residential line item. Moreover, that funding increase in the state-operated residential line item is actually a result of the underlying dynamic of privatization.
As we have noted before, there has been a net increase of 40 state-run group homes over the total number in 2008; but the state has closed state-run residences even as it has built new ones. It appears the new state-run residences and the additional funding for those residences have been intended to accommodate the more than 250 people who have been transferred since 2008 from the closed developmental centers and the closed state-run homes. Those are apparently the only people who have been admitted to the new state-operated homes.
As we’ve also pointed out, the administration does not even offer state-run residential facilities as options for developmentally disabled people waiting for residential care. Privatized, corporate-run care has become the only “choice” available those people despite the fact that the federal Medicaid Law requires that developmentally disabled individuals and their guardians be informed of the available “feasible alternatives” for care.
DDS administration (5911-1003): In addition to administrative functions, this line item funds DDS service coordinators, who are responsible for ensuring that clients throughout the system are receiving services to which they are entitled. The service coordinators have seen their caseloads rise dramatically in recent years, but funding under this line item has never kept up with the caseload increases.
The governor’s Fiscal 2017 budget would cut the DDS administrative line item by $977,000, or 1.4 percent. (In nominal dollars, the governor is proposing a slight increase in this line item, but it’s a cut when adjusted for inflation.) Since Fiscal 2012, this line item will have been increased by 8.1 percent if the governor’s Fiscal 2017 budget is approved.
Other line items that demonstrate the administration’s commitment to increased DDS privatization include the following:
Community day and work 5920-2025: The governor’s budget would increase this line item by $5.6 million or 3 percent. Since Fiscal 2012, this line item will have been increased by 45 percent if the governor’s Fiscal 2017 budget is approved. It appears that some of the increase proposed for this line item reflects the transfers of people from sheltered workshops to day programs.
Employment pilot program 5920-2026: The governor’s Fiscal 2017 budget would increase this line item by $4.6 million, which is a major increase, given that the current year appropriation is just over $3 million. That proposed 150 percent increase reflects the transition from sheltered workshops to supposed integrated employment.
The pattern of privatization in Massachusetts state government has become almost permanently established even though the benefits of privatization are highly debatable. Many questions have been raised about the privatization of prisons and the privatization of education in Massachusetts and elsewhere around the country. The privatization of human services may be the biggest prize of all for government-funded contractors. We need to preserve what’s left of state-run services.
Few people moving from sheltered workshops to “integrated” jobs
While the Baker administration appears to be moving ahead with a policy of closing all remaining sheltered workshops for developmentally disabled persons in Massachusetts, records show that relatively few people so far have been transferred from the workshops to the “integrated employment settings” that are supposed to replace them.
Confirming our concerns, the data from the Department of Developmental Services show that most of those people have been transferred to community-based day programs funded by DDS or MassHealth.
This has financially benefited corporate DDS providers that run the day programs and that have been among the most vocal proponents of shutting down the sheltered workshops. In what we consider to be an example of the inappropriate influence of private interests in DDS policy, two of those provider organizations actually helped draft a key DDS document that called for the workshop closures.
According to DDS records, the number of participants in sheltered workshops dropped by 1,166 between August 2014 and August 2015 — a 61 percent reduction from the 1,913 people who had been in those programs. The number of sheltered workshop providers dropped from 39 to 14.
In that same period, the number of developmentally disabled persons in corporate-run, community-based day programs increased by 1,116, or 27 percent.
In contrast to the increase in day program use, the number of developmentally disabled people in “integrated employment” settings increased from August 2014 to 2015 by only 337, or about 6 percent. DDS said it had no records on the number of integrated workplaces that exist in Massachusetts.
Community-based day programs actually cost considerably more to run than do sheltered workshops, according to an expert in the field.
A DDS document in November 2013, titled “Blueprint for Success,” stated that it was the department’s goal to close sheltered workshops to new participants as of January 2014 and to close all remaining workshops as of June 30, 2015. The closure of all of the workshops has not yet occurred, but it appears to be likely to happen despite protective language placed in the state budget for the workshops.
The title page of the Blueprint states that the document was prepared by DDS and by the Massachusetts Association for Developmental Disabilities Providers (ADDP) and the Arc of Massachusetts. Both the ADDP and the Arc are largely supported by DDS-funded providers, which have benefited from higher DDS funding for the day programs to which most of the former sheltered workshop participants have been transferred.
The Blueprint called for a total of $26.7 million in state funding over a four-year period for the transition from sheltered workshops to mainstream work settings. But the document did not offer specifics as to how those mainstream jobs would be found.
A 2014 Blueprint Progress Report, drafted by DDS and the ADDP, stated that $3 million allotted in the Fiscal Year 2015 budget for the transition from the sheltered workshops fell short of $5.5 million that DDS and the corporate providers had requested. Nevertheless, the report stated that 31 of 39 provider agencies would receive funding to transfer participants out of the workshops.
It now appears most of the funding has gone toward community-based day programs. The expert we talked to suggested that it would have been more effective had the funding been earmarked for subsidies for employers for hiring developmentally disabled workers.
Sheltered workshops provide developmentally disabled persons with a range of assembly jobs and other types of work, usually for a small wage. But the programs have become targets of a political ideology that holds that any type of congregate care setting is institutional in nature and therefore bad for those involved. Sheltered workshops allegedly “segregate” developmentally disabled people from their peers in the wider community or in the mainstream workforce.
“Integrated individual employment” is defined by DDS in a 2010 policy directive as “taking place in a workplace in the community where the majority of individuals do not have disabilities.” In addition, the policy directive states that the “optimal employment status is earning the prevailing wage.”
Many families of the sheltered workshop participants have countered that those programs are fully integrated into the surrounding communities and provide the participants with meaningful activities and valuable skills. Those families have also raised concerns that there are relatively few integrated or mainstream workforce jobs available for people with developmental disabilities; and that absent a sufficient number of such jobs, former sheltered workshop participants are likely to be transferred permanently to community-based day programs that do not offer the same activities or skills as the workshops did.
The contrast between the percentages of people who have been transferred to day programs and those placed in integrated employment is not alluded to in a September 2015 progress report submitted by DDS to the Legislature’s House and Senate Ways and Means Committees and to the Children, Families, and Persons with Disabilities Committee. The data noted above on the numbers of people in sheltered workshops and other programs in 2014 and 2015 can be found in tables in the report; but there was no analysis in the report of the data and no conclusions drawn based on that data.
In that five-page report, DDS Commissioner Elin Howe stated that DDS was offering training and consultation services to day program providers on the “delivery of quality, inclusive community based services…” Howe also said DDS was working “to assure that all individuals have access to and integration in the community…”
But Howe did not explain in the report how or when that access to integration in the community would be achieved by DDS. Howe’s report also provided no data or information on the types of services offered in community by day program providers or how successful those programs might have been.
The DDS’s 2010 policy directive similarly did not contain a plan for placing former sheltered workshop participants in mainstream jobs; but the policy directive did take a strong ideological stance against the workshops, going as far as to state that mainstream employment had been shown to be “a viable option… even for those individuals with the most significant level of disability…” No evidence or source was cited for that statement.
The disappearance of sheltered workshops appears to be yet another example of the erosion of cost-effective care for the developmentally disabled due to the influence of corporate interests that stand to benefit financially from it. At the very least, this case shows that a public agency should not develop policies jointly with the corporate contractors that it funds.
Andy and Stan McDonald gain a small victory in a system that has been pitted against them
In a Middlesex Probate Court hearing last Monday (October 26), Andy McDonald, an intellectually disabled man, finally got the opportunity to tell a judge his long-sought wish — that he be allowed to visit his aging parents in their Sherborn home.
As we have reported, Andy, who is 48 and lives in a group home in Westborough, has been denied permission since 1996 to visit his parents. Andy’s father, Stan, is now 80. In a ruling in 2006, former Probate Judge Edward Rockett concluded that Andy was sexually dangerous and should never be allowed to return to his childhood home.
Not only were Andy’s parents never to discuss with Andy the prospect of his ever visiting his home, but Rockett ruled that Stan must personally tell his son, in the presence of clinicians, that he would never be allowed to go home again. McDonald said he has refused to say something like that to Andy.
I will discuss Rockett’s ruling more fully below. We have noted previously that a key claim made in the ruling — that Andy was arrested in 1990 for sexually assaulting three young girls — is untrue. Andy has never been charged with a sexual offense.
Yet Rockett’s decision, and the claim in it that Andy was arrested for sexual assault, is the basis for the Department of Developmental Services’ longstanding position that Andy should never be allowed to return to Sherborn, and that the matter of visits there should never be discussed with him.
Rockett’s ruling
We think it is important to expose what we see are misstatements and a lack of a factual basis in Judge Rockett’s ruling. Rockett decision, and an appeals court ruling upholding it, were repeatedly cited during a break in the court hearing last week by a DDS attorney as reasons to oppose ever lifting the ban on home visits.
Stan was even told he would be in contempt of court if he mentioned to the judge his own wish that Andy be allowed supervised visits home. As it turned out however, it was Andy himself who brought up the subject of home visits before the judge.
Beyond that, there is a larger reason for examining Rockett’s decision, we think. Someday, Andy will be on his own; and if the conclusions in Rockett’s decision are never challenged, he may be locked up somewhere for good. One attorney contacted by Stan about his case termed Rockett’s decision “devastating.”
It therefore seemed somewhat extraordinary that there were no objections last week when Andy asked to speak to Middlesex Probate Judge Megan Christopher during the October 26 hearing. When Christopher assented to his request to speak, Andy politely asked that he be granted a supervised visit home “for a couple of hours.”
Judge Christopher didn’t flatly deny Andy’s request, but said she would schedule a new trial date in which that issue may be considered. She told Andy that what he wanted “was complicated and required more looking into.” She pointed out that “it’s not always possible to have everything you want. You understand that,” she added.
The October 26 probate hearing was held to consider the appointment of attorney Marie Dunn as Andy’s new guardian, replacing Dennis Yeaw, an attorney who had opposed home visits for Andy, also citing Rockett’s decision. In 1986, Stan and his former wife agreed to the appointment of a guardian for Andy as part of the settlement of a longstanding custody battle over him. Stan has been unsuccessful since that time in regaining his guardianship, even though his former wife, local legislators, and other supporters have publicly expressed support for that.
Andy’s arrest
Andy was arrested in Sherborn in May of 1990 for threatening an unidentified person during a telephone call, according to the district court record. The nature of the threats was not disclosed. In July of that year, he was charged with disturbing the peace in downtown Sherborn, according to a police department report. In that incident, he allegedly followed a young woman and threatened to kill her father. That same day, he was charged with assault after he punched Ellen, his stepmother. Stan and Ellen say the punch was accidental.
Andy has not exhibited any significant behavioral problems in close to a decade and has been taken on community outings to many places other than his home without any behavioral incidents, according to Stan and to his yearly clinical care plans. He is described in his latest clinical care plan as “kind and friendly to others,” and as “a polite man.”
According to the plan, Andy enjoys going to the library, going out to dinner, and seeing his father’s jazz band play. He regularly goes into the community to shop for program supplies and volunteers at Meals on Wheels.
Yet, Andy has in the past told clinicians that he has had sexual fantasies about children; and that, combined with the mistaken claim that he was arrested for sexual offenses in Sherborn in 1990, led to Rockett’s lifetime ban on him from visits home. Stan maintains that the ban on visits has caused Andy emotional harm. His latest clinical care plan states that Andy’s rapid speech and eating habits are related to anxiety, although the plan attributes that anxiety to a fear of death and bees.
One-sided view
Rockett’s decision appears to take a selective view of the history of the case.
In his ruling banning Andy from Sherborn for life, Rockett concluded that Stan “should never be considered for appointment as guardian of his son,” and that Stan “lacks common sense and has poor judgment skills.” Rockett stated that Stan and other family members, who he didn’t name, “wish to usurp the authority over the program and introduce their own ideas for clinical treatment for Andrew…”
Rockett further banned Stan from ever directly contacting any doctor, clinician, or service provider providing care to Andy.
Rockett’s decision, however, said nothing about Stan’s long-time personal advocacy on behalf of Andy, in particular his successful fight to discontinue the use on Andy of Stelazine, an anti-psychotic drug, which appears to have caused Andy’s disruptive behaviors prior to 2006. Rockett also did not mention the fact that clinicians had misdiagnosed Andy in the early 1990’s as mentally ill when, in fact, he is intellectually disabled, and that, as a result, Andy was inappropriately placed in Westborough State Hospital, a facility in which he was first put on Stelazine.
The Stelazine caused Andy to develop Tardive Dyskinesia, a disorder resulting in involuntary, repetitive body movements. Because the court-appointed guardians did little or nothing to address that problem, Stan said he personally got a court order and paid for an independent evaluation of Andy’s medications. This resulted in discontinuing the Stelazine and replacement of the prescribing doctor.
Among those who have written DDS in support of Stan’s bid for guardianship since that time has been State Representative David Linsky, who earlier this year was joined by State Senator Richard Ross in calling for a new, independent clinical evaluation of Andy.
John Carroll, a former residential counselor to Andy at the Cardinal Cushing School, wrote to DDS in 2013 to say that he had frequently observed visits to Andy by Stan and Ellen, and that “Stanley’s and Ellen’s dedication to Andy’s care and treatment in all circumstances leaves no question in my mind that Stanley McDonald is the sole individual with the knowledge, experience, and love, deserving to have responsibility for major decisions in Andy’s life as guardian.”
But Rockett didn’t see it that way. In his 2006 decision, Rockett accused Stan of failing to cooperate with Andy’s court-appointed guardians and with clinicians, and stated that Stan failed to “recognize the seriousness of Andrew’s fantasies.” He also implied in his decision that Stan had a drinking problem. He offered no evidence for that, however.
Failure to specify prohibited materials
In support of the former accusation regarding the seriousness of Andy’s fantasies, Rockett stated that “Andrew uses pictures of children as sexual stimulants,” and that Stan had provided Andy on a number of occasions with “prohibited materials.” But Rockett did not state what those prohibited materials were.
According to Stan and Ellen, the prohibited materials consisted of the following items: A piece of beach glass (which Westborough State Hospital considered dangerous), a sparkler that was lit on a birthday cake, a drawing of a baby from a Family Circus cartoon, and a photo of Andy’s niece and nephew. Ellen said a poster-sized version of the photo of Andy’s niece and nephew had been on the wall in his room in his group home with the staff’s full knowledge. “The poster seemed to us to indicate explicit authorization for Andy to have pictures of his niece and nephew,” Ellen said. “Stan did not show or give anything to Andy believing Andy would use them for any inappropriate purpose.”
Regarding the drinking issue, Rockett wrote that “Andrew has stated that his father’s drinking bothered him.” Rockett offered no further explanation of that claim, other than two follow-up statements concerning Stan’s visits to his son. One statement was that “Mr. Burch (the clinical director of Andy’s group home) had instructed Stanley McDonald not to drink during the visits.” The next line stated: “They (Stan, Andy, and Burch) went to a restaurant and Stanley McDonald immediately ordered wine. Andrew became very agitated and went to the restroom, where Mr. Burch had to quiet him down.”
Stan has never brought alcohol to Andy’s (group home) program. Andy does not like to be around Stan when he is drinking. Andy worries about the effects on Stan of alcohol and tobacco. He doesn’t want Stan to drink or smoke. He is very influenced by ads he sees on TV about the danger of drinking and driving. After that incident where Stan ordered a glass of wine in a restaurant he never again ordered an alcoholic beverage in Andy’s presence – until once very recently, when Andy didn’t express any objection. Stan does drink at Primavera (in Millis) while he is playing (in his Blue Horizon Jazz Band), and nobody has raised this as an issue – neither Andy nor staff who accompany him. Andy loves to be at Primavera when Stan is playing. He goes from table to table and talks with all of the guests and band members. Many have known him since he was a child. Nineteen years ago when Andy last visited at home Stan did not have a drink while Andy was there. Stan honors Andy’s wish and orders iced tea when we go out to supper. Stan smokes in Andy’s presence but tries to minimize it. It’s a tough habit for him to give up.
No support for statements about alleged dangerousness
Rockett’s decision also included a lengthy discussion of Andy’s alleged sexual dangerousness, starting with the mistaken claim discussed above that Andy was arrested in 1990 for sexual assault. Rockett referred three times to the arrest, and, in one instance, stated that Andy had “stalked the three neighborhood children.” As noted, there is no evidence in police or court records that anyone was sexually assaulted in those incidents, that any young children were involved, or that Andy stalked anyone.
(Even the appeals court, which upheld Rockett’s decision in 2009, stated in a footnote that “some of the fact findings adopted by the judge (Rockett) were not supported by the evidence…” The appeals court footnote specifically stated with regard to Rockett’s claims about the arrest for sexual assault and stalking three girls, “the specific facts (of the incidents in Sherborn) and the charges are not clear from the record.”)
Rockett also claimed in his decision that Andy had confessed to having “bizarre sexual fantasies” about children; yet Rockett noted that Andy “will always say what people want to hear.”
In addition, Rockett included what appears to be an unsupported and inflammatory statement by Burch that Andy was “the most dangerous person he has ever treated.”
But there is no evidence cited or presented in Rockett’s decision that Andy ever sexually assaulted anyone. Rockett stated, for instance, that in the 1990’s, when he was first admitted to his group home, Andy “attempted to attack female staff” in both his residential and day programs. But Rockett provided no details about those alleged attempted assaults.
Rockett’s decision also included two accounts about Andy’s alleged fantasies and about Andy engaging in masturbation; but while the accounts were graphic, nothing that Rockett described could be said to constitute crimes or prove that Andy was dangerous.
Ellen and Stan maintained that at least some of the statements given by clinicians regarding Andy’s alleged sexual fantasies may have stemmed from statements Andy made while participating in a group therapy program in the 1990’s in Andy’s group home, which is run by Community Resources for Justice. Participants were reportedly encouraged to discuss their sexual fantasies in the sessions.
“As I recall we were told at least some of the group members had actually offended,” Ellen said. “We weren’t told details of these sessions.”
Questions remain
Marie Dunn, the new guardian appointed last week for Andy, was not present at the October 26 court hearing. But both Andy’s court-appointed attorney and the DDS attorney encouraged Stan and Ellen to meet with Dunn. Stan is hopeful that Dunn will agree to a new, independent evaluation of Andy, and that she will support supervised home visits for him.
We hope things will finally move in a positive direction for Stan, Ellen, and Andy. We think it was a good sign that Judge Christopher allowed Andy to state his wish in open court to visit home. We also think it is a positive thing that Andy finally has a new guardian.
We strongly support at least a co-guardianship for Stan; and we hope the day comes soon when Andy can have supervised visits home once again, and that common sense will finally prevail in this case.
Federal government reviewing group home data in MA and two other states
The Inspector General in the U.S. Department of Health and Human Services has spent the past two years conducting a review of data on abuse and neglect in privatized group homes in three states, including Massachusetts.
In an August 21, 2013 letter written to U.S. Senator Chris Murphy of Connecticut, HHS Inspector General Daniel Levinson said his office had begun to examine data on admissions of persons from group homes and “nursing facilities” to hospital emergency rooms in Massachusetts, Connecticut and New York.
We obtained Levinson’s letter from the IG’s Freedom of Information Act Division. The letter promised to share the results of the IG’s findings with Senator Murphy’s office and left open the possibility of expanding the review. But the letter provided no details on how the review might be expanded.
Senator Murphy, who requested in March 2013 that the IG investigate group homes for people with developmental disabilities, has not responded to numerous requests from us for comment on the IG’s review.
It is not clear when the IG’s examination will be completed.
Despite what appear to be significant limitations in the scope of the analysis, the IG’s review appears to constitute one of the few instances in which the federal government has investigated the privatized group home system of care in the U.S. In contrast to that relative free ride given to the group home system, the federal government has filed dozens of lawsuits in recent years alleging substandard care in state-run, congregate-care facilities around the country.
There has been mounting evidence that abuse and neglect has been a continuing and growing problem in community-based, group homes. The IG investigation was requested by Murphy in the wake of a series of articles in The Hartford Courant that documented dozens of deaths, injuries, and other problems stemming from inadequate care and supervision in group homes in Connecticut.
Murphy asked the HHS IG to “focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.”
In his August 2013 letter in response to Murphy’s request, Levinson stated that for Connecticut, Massachusetts, and New York, “we are analyzing data to identify instances when Medicaid beneficiaries were transferred from group homes or nursing facilities to hospitals for emergency treatment. We are analyzing data by facility to determine whether certain facilities have excessive rates relative to those of their peers.”
Due to the way states collect the data, the IG’s analysis would include all Medicaid patients and not only those with developmental disabilities, Levinson said.
Given the vagueness of Levinson’s description of his office’s review, we have a number of questions about it. Levinson’s letter, for instance, didn’t specify what he meant by “nursing facilities,” and didn’t indicate which “peers” the emergency hospital treatment rates are being compared to. Are the group homes and nursing facilities being compared to developmental centers, for instance? It’s also not clear what the data will mean if it lumps together people with and without developmental disabilities.
Moreover, it is not clear whether the IG’s review has included data on actual deaths in group homes, which is what Murphy specifically asked the IG to examine, or whether the review has included differences in mortality rates of persons transferred from state-run to privately run care. A number of studies have shown increases in mortality rates among those transferred individuals.
The VOR, a national advocacy organization for the developmentally disabled, pointed out in recent testimony to a congressional subcommittee that higher mortality rates have been documented in Virginia, Nebraska, Tennessee, and Georgia in the wake of the DOJ’s deinstitutionalization settlements.
Based on Levinson’s letter, the IG’s review also doesn’t appear to have covered issues such as the quality of care in general in group homes, and it does not appear to be concerned with financial aspects of privatized care. All of those things are long overdue for investigations at both the federal and state levels of government. In the meantime, the federal IG’s investigation appears to be at least a step in the right direction.
The federal government’s cruel pursuit of deinstitutionalization
When is the federal government — particularly the Department of Justice — going to recognize or admit that deinstitutionalization of the developmentally disabled hasn’t worked as planned?
The DOJ seems to have closed its eyes to the realities on the ground in continuing to file lawsuits around the country to close state-run care facilities. This has caused “human harm, including death and financial and emotional hardship,” according to information compiled by the VOR, a national advocacy organization for the developmentally disabled and a COFAR affiliate.
While the DOJ has not filed such a suit against the State of Massachusetts, that may be because the state has closed, or is in the process of closing, four out of six developmental centers that were in operation as of 2008. But with two developmental centers remaining as well as other programs that the DOJ considers to be institutional, such as sheltered workshops, Massachusetts could well become a target for a lawsuit at any time.
The VOR filed testimony last month, urging a congressional subcommittee to adopt legislative language that would require the DOJ to do two very commonsense things before filing more lawsuits to close state-run facilities:
- First consult with the residents or their legal guardians “to determine residents’ needs and choices with regard to residential services and supports,” and,
- Second, do not “impose community-based treatment on patients who do not desire it.” This second requirement is consistent with the 1999 U.S. Supreme Court decision in Olmstead v. L.C.
The DOJ’s continued pursuit of class-action litigation to close developmental centers and other facilities has led to the irony that those lawsuits are generally opposed by the families of the residents on whose behalf the suits are ostensibly filed. As U.S. District Court Judge J. Leon Holmes wrote in 2011 in dismissing a lawsuit brought by the DOJ against the State of Arkansas to close the Conway Human Development Center center there:
…the United States is in the odd position of asserting that certain persons’ rights have been and are being violated while those persons – through their parents and guardians – disagree. (U.S. v. Arkansas, June 8, 2011, dismissal order).
Judge Holmes’ decision noted that evidence in the case showed that the parents and guardians of residents of the Conway Center “are overwhelmingly satisfied with the services there and believe that the Center is the least restrictive, most integrated placement appropriate for their children and wards.” Moreover, the judge’s decision stated that the weight of the evidence in the case failed to support the DOJ’s contention that care at the Conway Center was substandard.
The VOR notes that the DOJ’s Civil Rights Division has filed more than 45 legal enforcement actions in 25 states since 2009 to limit or shut down state care. On a website listing all the litigation it has filed, the DOJ includes the heading “Olmstead: Community Integration for Everyone.”
It’s not true, though, that Olmstead requires community-based care for everyone. The Supreme Court decision established a right to community-based housing and care only when:
1. The state’s treatment professionals have determined that community placement is appropriate,
2. Transfer is not opposed by the affected individual, and
3. The placement can be reasonably accommodated, taking into account the resources available to the state and the needs of others with mental disabilities.
Despite those clear conditions, the DOJ has plowed ahead with its community-integration lawsuits under the explicit assumption that all institutional care should be ended and everyone should be sent into community-based care, whether they want to go or not.
This viewpoint by the DOJ is a misinterpretation of the Olmstead decision, and it has had tragic consequences, according to the VOR. The organization pointed out in its testimony that higher mortality rates have been documented in Virginia, Nebraska, Tennessee, and Georgia in the wake of the DOJ’s deinstitutionalization settlements.
Those problems have occurred because so many of the privatized group homes to which the people formerly in the state facilities have been transferred are poorly monitored and are afflicted by high turnover and poor training of staff. Yet, that reality does not appear to have been recognized by the DOJ.
In Virginia, a state sued by the DOJ to close its state-run developmental centers, the risk of mortality for those individuals who left those centers was double that of those who stayed.
In Tennessee, DOJ lawsuits resulted in the closure of one developmental center in 2010 and the downsizing of two others. In that state, deaths among people released from institutions nearly doubled between 2009 and 2013. In addition, according to The Tennessean, a 2013 State Comptroller’s audit reported a lack of access to adequate medical and dental care, incarcerations, and hundreds of reports of abuse, and neglect and exploitation among the transferred developmental center residents.
In Nebraska, a 2014 monitoring team report found that of 47 persons considered to be “medically fragile,” who were transferred from a developmental center in 2009 as a result of a DOJ settlement, 20 (or 43 percent of them) subsequently died.
In Georgia, a 2010 a DOJ settlement agreement required the closure of all state-operated developmental centers and the transfer of 1,000 persons with developmental disabilities as well as 9,000 persons with mental illness from facility-based care. In March, The Augusta Chronicle reported that of 499 individuals with profound developmental disabilities, who had been transferred from the state developmental centers under the DOJ settlement, 62 (or 12%) died unexpectedly.
The Augusta Chronicle article discussed the case of Christen Shermaine Hope Gordon, a 12-year-old girl who died in community-care after being transferred from the Central State Hospital in Milledgeville, GA. The article recounted a litany of poor decisions and poor care that appear to have led to Christen’s death.
In a letter to the DOJ in January of this year, Margaret Huss, president of Intellectual Disabilities Advocates of Nebraska, urged the DOJ to ask critical questions about the mortality figures and other data regarding the transfer to community-based care prior to filing further lawsuits to close state facilities. “An increased risk of death should not be the unintended consequences of the worthy goal of community integration,” Huss’s letter stated. As of May 1, the DOJ had not responded to her letter.
That an increased risk of abuse, neglect, and death exists in community-based care has long been recognized, but few policy makers or people elected to office have been willing to stem the tide of deinstitutionalization. In March 2013, U.S. Senator Chris Murphy of Connecticut did call for an investigation of abuse and neglect in privatized group homes around the country, in response to a series by The Hartford Courant detailing those problems in that state.
In a letter to the Office of the Inspector General in the U.S. Department of Health and Human Services, Murphy termed the level of abuse and neglect in group homes “alarming.” Murphy asked the IG “to focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.”
But more than two years after Murphy’s request, it is not clear that the HHS Inspector General ever did undertake such an investigation. The IG’s office has so far not released a report and did not respond to an email query from us on April 30, seeking information on whether an investigation has been undertaken and what its status might be.
Senator Murphy’s office also did not respond to repeated inquiries from us last week as to whether Murphy ever received a response from the IG to his call for an investigation or whether he ever followed up with the IG after his original request in 2013.
Unfortunately, lawmakers in the U.S. Senate, in particular, have also not been supportive of VOR’s proposed legislative language to require the DOJ to consult with families before filing further lawsuits against state care. While language was inserted in a House appropriations bill for the DOJ last year at VOR’s request that protections for institutional care be considered by the DOJ as appropriate for those who desire it, that language was later watered down.
We can only hope that folks begin to wake up in Washington and elsewhere to overwhelming evidence that deinstitutionalization accompanied by privatization is not working, and that someone finally steps forward to slow both of those trends.
The HW&M budget has great news for sheltered workshops, not so good news for state care in general
The great news is the House Ways and Means Committee re-inserted protective language last week in the proposed Fiscal Year 2016 state budget that would protect vital sheltered workshops from closure.
Representative Brian Dempsey, chair of the committee, who was instrumental last year in keeping the workshops open, has renewed his commitment to those facilities in this year’s budget go-round with the administration.
The bad news is that the House Ways and Means budget continues to squeeze state-run programs for the developmentally disabled and maintains the administration’s disproportionate increase in proposed funding for the corporate, provider-run group home system. But let’s look at the good news first.
Last spring, after a lobbying campaign by advocates of the workshops, Dempsey placed language in the House Ways and Means version of the current-year budget, stating that DDS “shall not reduce the availability or decrease funding for sheltered workshops serving persons with disabilities who voluntarily seek or wish to retain such employment services.” The protective language survived a House-Senate conference committee in June, largely due to Dempsey’s support.
While that protective language in the budget appeared to offer the workshops an indefinite reprieve, the proposed fiscal 2016 budget submitted by Governor Charlie Baker in March removed the language. As a result, the workshop supporters went to work once again in the past month, calling Dempsey’s office and urging their local legislators to reinstate his language.
Dempsey did reinstate the language; and in a conference call last week concerning the House Ways and Means budget plan, DDS Commissioner Elin Howe indicated that the administration did not intend to file any amendments to remove the language from the budget legislation. It also appears that organizations representing corporate DDS providers, such as the Association of Developmental Disabilities Providers, have not filed amendments to close the workshops.
It is now up to the Senate and specifically to Senator Karen Spilka, the chair of the Senate Ways and Means Committee, to follow Rep. Dempsey’s lead and insert the same protective language in the Senate budget.
The workshops first came under attack from the administration of then Governor Deval Patrick, which targeted them for closure as of this coming June, arguing that they were “segregating” disabled persons from their peers in the mainstream workforce. But families of the workshop participants fought back. They maintain that the facilities are fully integrated into the surrounding communities and provide the participants with meaningful activities and valuable skills.
Sheltered workshops provide developmentally disabled persons with a range of assembly jobs and other types of work, usually for a small wage.
Meanwhile, the bad news we were talking about largely concerns funding for DDS group homes, remaining developmental centers, and service coordinators. The House Ways and Means budget proposal would cut the developmental center line item even deeper than Governor Baker has proposed and would reduce the service coordinator line item below the amount proposed by the governor. It would also fund the state-operated group homes at a level below what DDS considers a “maintenance level.”
While the state has closed three of six existing developmental centers since 2008 and is in the process of closing a fourth, funding appropriated to run the remaining three centers may have dropped too fast to maintain existing services in those facilities. As we recently noted, years of cuts in the developmental-center line item have lately resulted in the closing of several cottages at the Wrentham Developmental Center, requiring residents to be moved from long-time residential locations.
The Wrentham Center has become a major destination for persons transferred from the developmental centers that have been closed in recent years.
While Governor Baker’s fiscal 2016 budget would cut the developmental center line item by about $375,000 from projected spending, the House Ways and Means budget would cut it by $1 million beyond that.
DDS-operated group homes would get the same amount in fiscal 2016 under the House Ways and Means budget as under the governor’s version of the budget, which amounts to a $2 million reduction from what DDS considers a “maintenance budget.”
Also, the House Ways and Means budget would fund the DDS line item that pays service coordinators at a level $538,000 less than what Baker has proposed. In March, DDS Commissioner Howe had said Baker’s budget would fund the service coordinator line item at $1.8 million below what DDS had requested. So the House Ways and Means budget further reduces that proposed funding for the service coordinators next year by more than half a million dollars.
The service coordinators, whom Howe has referred to as “the heart and soul” of DDS, are responsible for ensuring that clients throughout the system are receiving services to which they are entitled. The service coordinators have seen their caseloads rise dramatically in recent years.
In last week’s conference call, Howe noted the shortfalls in funding under the House Ways and Means budget for the developmental centers, DDS-operated group homes, and service coordinators. But in what may be a sign of the priority that this administration places on these services, Howe said the Department did not plan to seek amendments to the House budget to increase that funding.
At the same time, the House Ways and Means budget preserves a major funding increase to the corporate providers in the coming fiscal year. The Ways and Means plan provides for the same $35 million increase from the current year for the DDS corporate residential line item that Baker has proposed. As of July, this line item will have been increased by more than 28 percent since the filing of a lawsuit by the corporate providers in June 2014 against the then Patrick administration.
While we understand that direct-care workers in corporate, provider-operated group homes are woefully underpaid, it’s not clear how much of the additional funding being sent to the providers is, or will be, going to those workers. As we have noted, the hundreds of executives working for those provider agencies in Massachusetts have been making out quite well.
The Baker administration is apparently fine with that state of affairs. Terming the House Ways and Means plan “a very reasonable budget,” Howe pointed out that it would add $17 million to the DDS bottom line compared to the governor’s budget. Under the House Ways and Means budget, the Community Day and Work line item would be almost $10 million higher than what the governor proposed.
The House Ways and Means budget also would provide $12.4 million under a new DDS line item to implement the expansion of DDS eligibility to people with autism, Prader-Willi, and Smith-Magenis Syndrome.
While that expansion of eligibility funding is certainly needed, the Senate has a lot of other work in store for it as well. We hope that in addition to protecting the sheltered workshops, the Senate begins to address the imbalance in the budget between corporate and state-run DDS care.
Human service providers’ lawsuit boosts their state funding despite deficit
While programs and services are being cut throughout state government as a result of projected budget shortfalls, corporate human services providers have gotten hundreds of millions of dollars in additional state funding due, at least in part, to a lawsuit they filed against the state.
The irony is that the U.S. Supreme Court has just ruled in a separate case that providers cannot sue to raise Medicaid service rates. So, it’s not clear to us that the Massachusetts providers were on solid legal ground in filing their lawsuit.
In June 2014, the providers sued the then Patrick administration, arguing that the administration was not boosting state funding to them fast enough to satisfy a timetable set in a 2008 law known as Chapter 257. Chapter 257 established formulas and timetables for increasing provider funding rates.
As a result of the lawsuit, both the Patrick administration and the incoming Baker administration approved major funding increases to the provider-run group-home line item in the Department of Developmental Services budget, even as it was becoming clear the state was facing major budget shortfalls in the current and coming fiscal years.
In a press release issued on March 4, the day he submitted his Fiscal Year 2016 budget to the Legislature, Governor Baker stated that his administration had allocated $30 million “to resolve litigation and adjust Chapter 257 rates for human service providers.”
The $30 million referred to in the governor’s press release may have understated the impact of the lawsuit. Baker’s proposed funding for the provider group-home line item in the DDS budget for fiscal 2016 is more than $230 million higher than the amount appropriated for that line item in fiscal 2014 when the provider lawsuit was filed. That is a 28 percent increase.
In contrast, the line item for the state developmental centers would be cut in that same period by almost 9 percent, and state-operated group homes would get an increase of about 13 percent in that time period.
In what sounds like a similar lawsuit to the the litigation in Massachusetts, service providers in Idaho had argued in federal court that Idaho had failed to raise Medicaid payments to them as outlined in a federally approved formula. But the U.S. Supreme Court ruled on March 31 that private providers cannot sue for higher Medicaid reimbursement rates.
In the suit filed by the Massachusetts providers, state Superior Court Judge Mitchell Kaplan ruled in January that the state had violated Chapter 257 by not setting higher rates for providers. In response to the suit, the then Patrick administration had initially argued that Chapter 257 could be fulfilled only if the state itself had adequate revenues to do so.
But Judge Kaplan ruled that the state had to comply with the higher rates required under Chapter 257 regardless of whether the funding was available or not. That would mean that in order to fulfill the requirements of Chapter 257, funding would have to be cut in other areas, which is what has happened.
Like the Idaho providers, the Massachusetts providers had argued that the inadequacy of the state funding was causing them to fail to keep up with rising costs and was resulting in lower paid staff and high staff turnover as well as poorer quality services. We have maintained, though, that the funding has been adequate to support high salaries for executives running the provider corporations. Close to $100 million a year is spent on those executive salaries in Massachusetts.
As we’ve noted before, the major funding increases in the provider line item in the past year have increased an already existing imbalance in funding between that line item and accounts for state-run services.
One example of that imbalance is the state-run developmental center line item, which will be some $10.6 million less under Baker’s fiscal 2016 budget than it was in fiscal 2014. This has led to the necessity of closing several cottages at the Wrentham Developmental Center in the past several months, requiring residents to be moved from long-time residential locations.
An April 2 memo sent to Wrentham Center staff referred to an “immense challenge” in meeting budget constraints facing the Center in the current fiscal year, and a “yet another difficult budget forecast for Fiscal Year 2016.”
At the time the Massachusetts providers filed their suit, a spokesman for the providers explained that they had rejected an offer from the then Patrick administration to meet them more than part-way by providing 90 percent of the full funding increase specified under Chapter 257 as of January 2015.
“…in the end, it wasn’t enough,” the spokesman for the providers said. “At this point, we’ve been as patient as we can be and the law is the law and we want the Commonwealth to abide by the law. Every day that full implementation is delayed, the imbalance and the unfairness grows.”
The providers and the Baker administration, however, do not seem to be as concerned about the continuing and growing imbalance in funding between provider and state-run services.
Public Health Department needs to release report on death of developmentally disabled man
The Department of Public Health has completed an investigation of the case of a developmentally disabled man who died en route to Lowell General Hospital in February 2012 after having been turned away from the hospital twice without any significant treatment.
We may never know, however, what the result of the investigation is. The Department, citing the deceased man’s privacy rights, won’t release the report.
We are appealing this denial to the state’s Public Records Division, arguing that the potential public interest in knowing what happened in this case outweighs the privacy rights of a deceased individual. Our view is that the real potential wrong to this person was done when he was denied treatment by the hospital. The public, we think, deserves to know what happened here and so do persons with developmental disabilities and their families and guardians.
This case suggests possible inadequate training of health care personnel in the treatment of developmentally disabled persons, which is an issue of concern to advocates for the disabled and to many policymakers.
The National Council on Disability, with which we have had our disagreements, maintains that:
The absence of professional training…for health care practitioners is one of the most significant barriers preventing people with disabilities from receiving appropriate and effective health care.
The man was a former resident of the Fernald Developmental Center. He had been living in a group home in Chelmsford and was attending a day program in Lowell on the morning of February 6, 2012, when the staff at the day program made the first call to 911 to take him to the hospital. He had reportedly been having difficulty breathing and was sweating profusely. The hospital released the man shortly after his arrival, however, and sent him back to his group home, according to sources.
By about 8 a.m. the following morning, the man was slumped over in his wheelchair and sweating heavily, a source said. A group home staff member called 911 shortly afterward.
A Disabled Persons Protection Commission (DPPC) complaint form stated that the man was observed at the hospital on the morning of February 7 to be sweating profusely, but his vital signs were good when he arrived. According to the complaint form, the man was sent home with a prescription (the name of which was redacted). According to sources, this was the second time he had been sent away by the hospital.
The DPPC complaint form stated that shortly after arriving back at the group home, the man began to vomit and then lost consciousness, and that the staff began mouth-to-mouth CPR until paramedics arrived. The group home received a call from the hospital later that afternoon that the man had died.
Because the man’s death appeared to have been connected with his treatment or lack of treatment by the hospital, the DPPC referred the case to the Department of Public Health for investigation.
Did the apparent failure of Lowell General Hospital to properly diagnose this man’s illness and provide him with adequate treatment result from a lack of training in disability issues? Did the Public Health Department consider that question in their investigation of this case? Unless the Department releases its report, we will never know the answers to those questions.
While the Public Health Department’s position is that a state law [(M.G.L. c. 66A, s. 2(k)] prohibits them from releasing medical information about an individual, even if that person is deceased, we are not in agreement with their interpretation.
First, there do not appear to be consistent policies among state agencies in releasing investigative reports on deaths of developmentally disabled persons. The Disabled Persons Protection Commission (DPPC) has released a number of these reports to us after redacting what they considered to be identifying information.
Secondly, while we have blogged about this case, we have never used the name of the individual involved or tried to publicly identify him. A Department of Public Health attorney wrote to us, though, that even if we did not use the individual’s name in a blog post about the investigative report, “it is possible for someone to utilize the information that is available (age and date of death) and potentially come up with the patient’s name.” While that is possible, we do not understand why anyone would do that in this case. It seems farfetched.
Third, even if it were true that someone might reveal the identity of the individual involved, there appears to be case law that limits privacy rights of deceased individuals. A Hofstra Law Review article notes that “while postmortem medical confidentiality exists, it is much narrower than the privacy protections guaranteed to the living.” In Massachusetts, case law involving privacy rights after death does not appear to have been settled. (See Ajemian v. Yahoo!, Inc.)
Finally, the privacy statute cited by the Public Health Department [(M.G.L. c. 66A, s. 2(k)] states only that the Department must:
maintain procedures to ensure that no personal data are made available in response to a demand for data made by means of compulsory legal process, unless the data subject has been notified of such demand in reasonable time that he may seek to have the process quashed.
This seems to imply that the person involved has to be living. And, as attorney Steve Sheehy notes in a comment to this post below, at most this statute would require notice to the deceased person’s executor or representative.
Prior to filing our appeal, I asked the Public Health Department attorney whether it might be possible to provide us with a copy of the investigative report with explicit personal data or medical information redacted. As I noted, our interest is whether the Department has investigated or commented on the hospital’s procedures for training staff to treat persons with developmental disabilities.
To the extent that the Department’s report addresses hospital policies and procedures in this case, it would probably not be necessarily for us to know specific medical details about this individual. To date, I have not received an answer from the Department to my query.
Unfortunately, this is not an isolated case of apparent institutional secrecy. When it comes to deciding whether to make public reports of potential mismanagement by human services or health care facilities, the natural instinct of public managers and administrators seems to be to keep it all secret and cite privacy rights as the reason. That has certainly been the practice at the DPPC, but at least, as noted, the DPPC has released redacted reports.
We hope the Public Records Division, which is part of the office of Secretary of the Commonwealth Bill Galvin, will make the right decision and order the Public Health Department to make known the results of its investigation of this troubling Lowell General Hospital case.
Compensation of provider executives in MA reaches $100 million
More than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation, according to our updated survey of the providers’ nonprofit federal tax forms.
By our calculations, state taxpayers are on the hook each year for up to $85 million of that total compensation.
We reviewed the federal tax forms for some 300 state-funded, corporate providers, most of which provide residential and day services to persons with developmental disabilities.
The following is a summary chart of our latest survey results (click on the chart to enlarge):

For the complete survey chart, click here.
We first released our survey about a year ago, when we found that more than 550 executives working for some 250 state-funded corporate providers of services to people with developmental disabilities in Massachusetts received a total of $80.5 million in annual compensation.
COFAR has also previously raised concerns that increasing amounts of money going to provider executives have not translated into higher pay for direct-care workers in Massachusetts.
The latest survey reports on 635 executives who received total annual compensation of $102.4 million and average annual compensation per employee of $161,231. The survey was based on provider tax forms filed in either the 2011 or 2012 tax years. Those tax forms are available online at www.guidestar.org.
The survey sample included 100 CEO’s and presidents, making an average of $210,227 in salaries and benefits; and 107 executive directors receiving an average of $130,835 in compensation. As the chart above shows, the survey also included 67 chief financial officers, 31 chief operating officers, 100 vice presidents, 110 directors, and 120 other officers, all earning, on average, over $100,000 a year.
A state regulation limits state payments to provider executives to $158,101, as of fiscal year 2013. Money earned by executives above the state cap is supposed to come from sources other than state funds.
Based on this regulation, we calculated that provider executives are eligible for up to $85 million a year in state funding to cover those total salary and benefits costs. Our calculation was based on identifying the companies paying executives at or above the state threshold of $158,101, and assuming that amount as the maximum state payment for each of those companies’ executives.
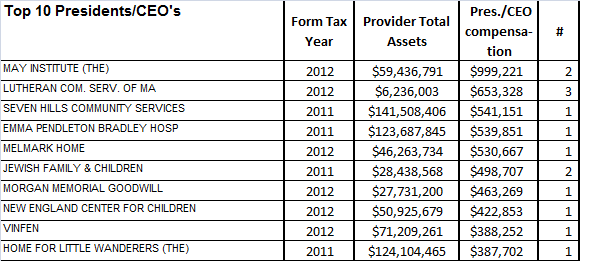
Among the top-paying providers in our latest survey was the May Institute, which paid two employees a total of $999,221 in the 2012 tax year. Both employees were listed as president and CEO of the provider. The May Institute’s federal tax form shows that one of the two employees, Walter Christian, worked for the company until December 2012 and received a total of $725,674 in salary and benefits in that tax year, which started on July 1, 2012. Christian was replaced as president and CEO by Lauren Solotar, who received a total of $273,547 in that same tax year, which ended on June 30, 2013.
Despite the regulation capping compensation payments by the state, the state auditor reported in May 2013 that the state had improperly reimbursed the May Institute, a corporate provider to the Department of Developmental Services, for hundreds of thousands of dollars paid to company executives in excess of that cap. COFAR had previously reported in 2011 that the state may have paid Christian and other executives of the May Institute more than the state’s regulatory limit on individual executive salaries.
The following charts show the top earning presidents/CEO’s and executive directors in our latest survey and the number of those executives holding each title in each company:

Most of the providers surveyed are under contract to the Department of Developmental Services, which manages or provides services to people with intellectual disabilities who are over the age of 22. The providers operate group homes and provide day programs, transportation and other services to tens of thousands of intellectually disabled persons in the DDS system.
As we have noted, the state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in fiscal 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
More financial information about nonprofit corporate providers, including compensation of executives, can be found at www.guidestar.org.
