Archive
Father and sister banned from all contact with developmentally disabled woman because they cried when they saw her
Can it really happen in America that the state can take an individual into its custody, and then not even let that person’s family know where she or he is, for months on end?
Yes, that is apparently the case if the individual is mentally ill or intellectually disabled.
In one of the more bizarre and severe instances of restrictions placed by the state on family contact, a court-appointed guardian has banned family members of an intellectually disabled woman from all contact with her because they allegedly became too emotional when they visited her. The 28-year old woman, whose name we are withholding, is dually diagnosed with intellectual disability and mental illness.
The woman’s father, David, and sister, Ashley, have not even been told for almost a year where she is living. Clinicians in at least one hospital said the family was to blame for signs of agitation and psychotic symptoms allegedly shown by the woman after the family visits.
The ban on family contact was imposed after the woman alleged that she had been sexually assaulted by the alleged boyfriend of her mother over a two-year period from 2012 to 2014. The woman’s mother, Nancy Barr, and her alleged boyfriend, John Leone, have both been arrested and are facing trial in Salem Superior Court in connection with the alleged assaults.
In addition to banning Leone and Nancy Bar from visiting the woman, a guardian with the Department of Developmental Services last Thanksgiving extended the prohibition to other family members and a family friend, who have not been implicated in the alleged crime. The only family member who is currently allowed to visit the woman is a maternal aunt, who Ashley Barr said had little prior contact with the woman and maintains little contact with either Ashley or her father.
“As far as I’m concerned, my daughter has been kidnapped,” David Barr said in an interview. Both David and Ashley said their lack of contact with their family member and lack of knowledge of her whereabouts have filled them with emotional distress. “We don’t even know where she is, and no one will tell us,” Ashley said. “It’s really, really hard to take.”
The Barr’s case is, unfortunately, not unique. We have reported on other cases (here and here) in which family contact with developmentally disabled family members has been severely restricted by the Department of Developmental Services. These restrictions also appear to happen in cases in other areas of the health care system, such as the highly publicized case of Justina Pelletier, who was held for nearly a year in a locked ward in Boston Children’s Hospital, and kept from all contact with her parents.
“This is unfortunately yet another case in which DDS and the probate court system has failed families of developmentally disabled persons,” said Colleen Lutkevich, COFAR executive director. “The family always seems to be made the focus of blame when problems occur.
“In this case,” Lutkevich added, “a young woman, who was victimized by sexual assault, is being further victimized by being isolated from members of her immediate family who could provide her with the love and support that she needs.”
David and Ashley have tried for months to get answers from the Department of Developmental Services and from the Department’s court-appointed guardian for the woman, and have gotten little information from them. They have gone to their local legislators and gotten little help, and have even gone to the media, but have been unable so far to get any news outlets to report their story.
Neither David Barr nor any other members of the woman’s family, other than her mother, are alleged to have known about the alleged sexual abuse while it was happening, and none have been charged or implicated in the crime. David Barr was divorced from Nancy Barr in 2003.
During the period of the alleged assaults, the woman had been under the care of her mother and had been living in her mother’s home. David Barr said that Nancy Barr has also been diagnosed with mental illness.
After the woman told a family friend about the alleged abuse in 2014, the friend reported the matter to police, and the woman was immediately removed from her mother’s care. She was apparently placed in a shared living arrangement in Haverhill, but that location was not disclosed at the time to any other members of the family.
In the months that followed, the family was only sporadically informed about their family member’s whereabouts. Her sister, Ashley, and her father said that virtually no information was provided to them for the first month after her removal. They were then allowed to visit her only a handful of times, either at a DDS area office or in Massachusetts hospitals to which she was admitted, reportedly after psychotic episodes. Ashley Barr currently lives and works in Rhode Island.
Last Thanksgiving, the DDS guardian, Dorothy Wallace, a psychiatric social worker, terminated all family contact with the woman. Ashley said she and her father have not been permitted to visit or call her for nearly a year, and they don’t know where she is currently living.
Guardian testifies against the family
Wallace, the DDS guardian, has declined to speak with COFAR regarding the case. In statements she provided in probate court in August 2015, she said she ordered that the family’s contact with the woman be restricted at that time because her father and sister would become overly emotional during visits with her. Wallace said clinicians in various hospitals in which the visits took place complained that the woman would be agitated and upset after the visits and that her symptoms of bipolar disorder would then become aggravated.
Wallace also contended that on one occasion, Ashley was overheard telling her sister not to listen to medical personnel at a hospital. Ashley disputes that, saying her sister had told her people were making fun of her, and that she told her not to listen to whoever was making fun of her. “Maybe someone misinterpreted me,” Ashley testified during an August 2015 probate court hearing. “I would never tell (her sister) not to listen to doctors.”
Wallace and Jill Casey, the woman’s DDS service coordinator, testified in the August 2015 probate hearing that their goal was to reunite her with her family once she was “clinically stabilized.” However, as of October 2016, more than a year later, the family has received no word from DDS as to when or if such a stabilization has occurred. Ashley Barr said her calls and text messages to both Wallace and Casey have gone unanswered.
DDS Commissioner Elin Howe responded to an email from COFAR about the case on October 6, and would say only that the case was under review. However, as of today (October 19) neither David nor Ashley had been contacted by the Department as part of that review.
Ashley acknowledged she and her father did become emotional at times during visits with her sister because she appeared upset at being kept isolated from them and often appeared to be over-medicated.
“For several visits we did cry in front of (her sister), I mean how could we not?” Ashley said. “She was alone, scared, by herself, and just went through a horrific thing for about two years. So yes, my father and I did cry, and I was an emotional mess for a very long time. Watching my sister all drugged up, she could barely talk, and given the state she was in, it was very hard to keep it in. I walked out of the room most of the time so my sister wouldn’t see me.”
In one of the last instances in which they were allowed to visit the woman, Ashley said it appeared she had not been bathed. Ashley personally gave her a shower at the hospital. Her hair was so dirty and matted, Ashley said, that she had to use an entire bottle of shampoo and conditioner to untangle it.
The enforced isolation of the woman appears to violate DDS regulations, which include the right to humane and adequate care and treatment, self-determination, least restrictive care, and integration of the person in the community. In addition, people in DDS care have a right to communicate, the right to have reasonable access to a telephone and to make and receive confidential calls, and the right to be visited and to visit others “under circumstances that are conducive to friendships and relationships…”
David Barr frustrated in gaining guardianship
Like many probate cases, this case has a complex history. David Barr has tried without success to gain guardianship of their family member following David’s divorce from her mother. In early 2015, the Essex County Probate Court passed over David and a long-time family friend, who had offered to be his daughter’s guardian, and instead appointed Wallace, the DDS-paid psychiatric social worker, who had never met the woman, as her guardian.
David Barr said he would have supported the family friend as his daughter’s guardian, but “we were totally ignored.” Barr has since filed a new petition for guardianship in probate court.
In the probate court hearing in the case in August 2015, David was described by his daughter’s DDS service coordinator as a “bully” because he allegedly swore at her when he first met her and once left a threatening message on her voice mail that he was going to “get you people.”
The Barrs had no attorney at the probate hearing, and there was consequently no cross-examination of the service coordinator. Ashley Barr says her father was threatening only to someday sue DDS over the restrictions placed on his contact with his daughter. “Not one time did my father ever mention coming after them violently,” Ashley stated in an email. “He’s trying to get his daughter back and not end up in jail.”
Ashley added that her father was not liked by some of the staff of his daughter’s day care provider agency because he would become angry and reprimand the staff following several instances in which she walked out of the provider’s facility unattended.
Restrictions on visits and information blackout began after the abuse was reported
Ashley Barr said that after the alleged abuse of her sister was discovered in October 2014 and her sister was removed from her mother’s care, “nobody would talk to us.”
Ashley said she was initially unable to get any information about her sister or her whereabouts from either the DDS service coordinator or her supervisor at DDS. She said she even contacted the police and was unable to learn anything from them. “My dad and I have no criminal record,” Ashley said, “yet we were still treated like criminals.”
Then, in November 2014, Ashley was contacted by Jill Casey, the DDS service coordinator, who said she would be allowed to visit her sister at the DDS area office in Lawrence for about an hour. David was not invited to that visit.
Ashley said she was told during the visit not to ask her sister any questions about where she was living. She said her sister “looked scared,” and said several times that she wanted to see her father and to come home.
A family friend, who was allowed to visit the woman around this time, said she was living in a home in Haverhill owned by a woman who had two or three other developmentally disabled persons living there. The friend said she was instructed not to tell anyone in the disabled woman’s family where she was.
The friend said she was allowed on one occasion to take the woman out of the Haverhill home for the afternoon. The woman was upset, she said, because she wanted to see her family. She also wanted to sleep over at the friend’s house, but that wasn’t permitted by the guardian.
It wasn’t until April 2015 that Ashley was next allowed a visit with her sister – this time in Arbor Fuller Hospital in Attleboro, where she was scheduled to celebrate her 27th birthday. Ashley said she was allowed a number of visits to Arbor Fuller, and David was allowed to visit as well, though a lesser number of times. It was apparently at Arbor Fuller, that Ashley and David first reacted too emotionally when they saw her.
In testimony in the August 2015 probate court hearing, Wallace, the guardian, contended that David Barr further agitated his daughter during at least one visit by telling her that she would be going home soon and that he would become her guardian. Hospital clinicians, Wallace said, subsequently asked her to terminate the family’s visitation privileges.
David Barr testified in response that he was trying only to reassure his daughter, who would become upset whenever he and Ashley had to leave. “I was just trying to provide reassurance that she would go home and that I would always be by her side and would try to get the guardianship,” David said. “She was there alone and scared. Isn’t that reassuring someone? Trying to give her confidence she isn’t going be left alone…?”
DDS and guardian repeatedly said family needed to be “educated”
During the probate court hearing, Wallace, Casey, and Barbara Green Whitbeck, a DDS attorney, repeatedly stated that they considered it necessary to “educate” David, Ashley and potentially other family members about what was in the woman’s best interest and the extent of her mental illness.
“I talked to Ashley,” Wallace testified. “She was angry and wanted to maintain the visits (with her sister). I tried to educate her that (her sister) is psychotic and symptomatic – that it can take two, three, four months (to stabilize) her. It’s not quick. I don’t think they (the family) understand the magnitude (of her illness).”
Ashley responded in an interview that she and her father felt that Wallace and Casey were being condescending in seeking to “educate” them about her sister. “We have known and talked about her conditions since day-one, 20 years ago, and about what she has been diagnosed with. It’s nothing new to us,” Ashley said. “We don’t need them to repeat things that we already know about her conditions.”
In June 2015, Ashley found out from her aunt that her sister had been admitted to Lawrence General Hospital because her psychiatric symptoms had flared up. Ashley was subsequently allowed to visit her a handful of times at Lawrence General, but David wasn’t, for reasons that were not provided to them.
After a short stay at Lawrence General, the woman was admitted to Tewksbury State Hospital. Ashley said that when she was living in Connecticut at that time and drove up to Massachusetts several times a week to visit her.
David was finally allowed to visit her at Tewksbury State in October 2015. She appeared drugged during that visit as well, according to Ashley. And that was the visit in which Ashley said she needed to use an entire bottle of shampoo and conditioner to untangle her hair.
That was also the last time either David or Ashley were permitted to visit their family member. “We were told by Dorothy Wallace we were getting her too excited and they were trying to control her medicine,” Ashley said. “That was an excuse. How else is she going to react when she sees her family and wants to go home? Of course, she’s going to get upset.”
Ashley did manage to see her sister without permission at Tewksbury State in December when she visited under an assumed name. She gave her Christmas presents during that visit. It was the last time she would see her.

David and his daughter hug good-bye at Tewksbury State Hospital.
In May, Ashley found out she was pregnant and learned that she was going to have a girl. She contacted the guardian to ask whether her sister would be allowed to come to the baby shower, which was planned for a restaurant in Andover. She said Wallace denied the request and told her that her sister would not be informed that she was pregnant.
Family friend also denied visits
The family friend who initially reported the alleged sexual abuse of the woman to police had initially been allowed to visit her, as noted earlier. However, when the friend tried to visit the woman at Tewksbury State in April on her 28th birthday, she was told that she was no longer there.
The friend said she was also told by a staff member at the hospital that she too had been placed on a no-visitor list. She said she was not given a reason for that prohibition. The friend said she understood that the only family member still allowed any contact at that point with the woman was the aunt, who had previously had little to do with her.
Ashley said David did hear from his daughter one last time in July when she apparently managed to find a cell phone and called him. She said the cell phone had a New Hampshire area code, but that the woman did not know where she was. The call was terminated after two or three minutes, she said.
“At that point, we knew she was still alive,” Ashley said. “But that’s all we knew.”
Call the Barr’s local legislators
When we at COFAR heard about this case, we contacted the office of David Barr’s local House member, State Representative Linda Dean Campbell. Both Ashley and the family friend had previously contacted Campbell’s office, but a staff member in the office indicated at that time that the office could do little to help them.
When we contacted Rep. Campbell’s office earlier this month, the staff member did offer to contact DDS on behalf of the Barrs. The staffer reported back that DDS would not discuss the case with Campbell’s office, but would pass along Campbell’s concerns to others in the Department.
You can contact Rep. Campbell’s office at 617-722-2430, or send an email to Linda.Campbell@mahouse.gov, and urge them to continue to try to work with DDS to resolve this case.
In addition, you can contact Governor Baker’s office at 617-725-4005; and DDS Commissioner Elin Howe at 617-727-5608; or email: elin.howe@state.ma.us. Say you believe David and Ashley’s visits to their family member should be restored immediately. Also, let them know that you hope and expect that as part of their review of the case, DDS officials will contact and interview both David and Ashley.
Guardianship under fire by the same groups that oppose congregate care and support privatization
Guardianship of persons with developmental disabilities is under fire in Massachusetts and elsewhere, and families could see their advocacy rights eroded as a result.
One prominent threat to guardianship appears to be embodied in a process called Supported Decision Making (SDM).
Under SDM, individual guardians are replaced by teams or “network supporters,” who enter into written agreements with disabled individuals to “help them make decisions” about their care, finances, living arrangements and other areas. The network supporters can include family members, friends, and corporate service providers, according to the Center for Public Representation, which is pushing for SDM in Massachusetts.
There are some promising aspects to SDM, but a number of concerning aspects as well.
To the extent that it can or does replace irresponsible or uncaring guardians with supportive teams, SDM would appear to have a potential to improve the lives of many people.
On the concerning side, SDM does not appear to be well designed for people with severe levels of disability. Those people are most in need of the protections of guardianship; yet, many SDM advocates paint guardianship with a broad, negative brush and don’t appear to acknowledge the value that family members, in particular, bring as guardians to the lives of their loved ones.
As Jill Barker notes in the Michigan-based DD News Blog:
Many advocates for SDM state explicitly that their goal is to eliminate guardianship. Others state that this is not what they are trying to do, but their words and actions show that they intend to make guardianship as difficult to obtain as possible.
Moreover, many of those SDM advocates appear to be from the same groups that have long opposed critically important congregate-care options for the developmentally disabled, and their language in support of SDM is similar to their longstanding ideological language in opposition to congregate care. In particular, they make the same questionable charges about guardianship that they have about congregate care — that guardianship leads to “segregation,” and that all persons under guardianship are prevented from “reaching their potential.”
We believe that like congregate care, guardianship is a necessary part of the total spectrum of care, particularly for people with the most severe levels of developmental disability, and that those choices and options shouldn’t be taken away from disabled individuals and their families.
As a result, we counsel parents of developmentally disabled children to consider obtaining guardianship rights when their child reaches the age of 18. Without such rights, family members are likely to have virtually no say in the decisions that are made by providers and the Department of Developmental Services with regard to their loved ones with developmental disabilities.
In a position paper on SDM, the VOR, a national advocacy organization for people with developmental disabilities and a COFAR affiliate, contends that SDM “could weaken protections for those who are the most vulnerable, the very people for whom guardianship laws were originally written.” The VOR adds that SDM threatens “to remove an individual who lacks the capacity to make his or her own decisions from the protection of the court and ongoing evaluation.”
Similar groups and similar language against guardianship and congregate care
The CPR and similar advocacy organizations in other states favor reducing residential options and choices, particularly when it comes to congregate care, and they use similar arguments to support the replacement of guardianship with SDM.
The CPR has supported or been involved in numerous lawsuits to close developmental centers over the objections of families of residents. Their argument has been that clinical experts know better than family members about what is in the best interest of their loved ones. Those advocates also support the dismantling of sheltered workshops and the privatization of residential services for the developmentally disabled.
The CPR is now making similar questionable claims against guardianship and in favor of SDM. In a PowerPoint presentation delivered in 2014, the CPR maintained that guardianship results in “civil death” for developmentally disabled persons, and that a key principle of SDM is that “people are not inherently incompetent.”
That latter claim, which has also been made in opposition to congregate care, seems absurd to us if it means that no individual can be found to be incompetent. Laws in Massachusetts and most other states require that people be found incompetent by courts in order to be considered for guardianship. If SDM advocates believe that no one is truly incompetent, then they must believe court rulings around the country involving thousands upon thousands of people were wrong. We don’t believe it’s possible that all, or even most, of those decisions were wrong.
Nevertheless, in a law journal article, SDM-proponent Leslie Salzman includes the following statement, which includes no citation, in a footnote:
Virtually everyone has the ability to participate in the decisions affecting his or her life, with the possible exceptions of persons who are comatose or in a persistent vegetative state. (my emphasis)
The CPR does acknowledge that some things about guardianship are good. In the 2014 PowerPoint, the CPR states that guardianship “offers a form of protection and provides some safeguards against abuse,” and that guardianship “makes it clear who is the ‘decider.’” But the CPR goes on to claim that guardianship results in a “loss of legal personhood” and a loss of civil rights such as the right to marry and vote. And the CPR contends that guardianship leads to possible exploitation by the guardian.
We disagree with the CPR’s claims. First, it does not appear to be true that a person under guardianship can’t vote. According to the Handbook for Massachusetts Guardians, which is published by the Massachusetts Guardianship Association, some incapacitated persons may have sufficient capacity to marry or vote. In those cases, the guardian can seek the court’s approval for such actions.
Also, as the Massachusetts handbook notes, current state law provides a number of protections for persons under guardianship and encourages limited guardianships when possible. Among the legal protections in place now is a requirement that guardians seek court authorization to make many major decisions for the incapacitated person – for example, admitting someone to a nursing facility for long-term care. The guardianship handbook further advises guardians to act in the incapacitated person’s best interest at all times, to do what that person desires to do, and to visit them at least monthly.
While it’s true that guardians can potentially exploit incapacitated people in their care, we are not sure that exploitation is less likely with SDM. If corporate providers, in particular, are on the SDM “network” teams, then there is a potential conflict of interest involved, since providers stand to make money by advocating for more services.
Barker points out in the DD News Blog that “guardianship abuse from family members can occur,” but she draws a crucial distinction — which SDM advocates appear to ignore — between the appointment of family members as guardians, and the appointment of attorneys, corporate entities and other professionals to that role. Family members, Baker states, are far more likely to attend to the needs and wishes of their loved ones under guardianship than are corporate or state guardians “with dozens of wards.”
Barker, who is critical of the SDM movement, adds:
Although there are horrific stories about what can happen to people under guardianship, we rarely see stories about unpaid family guardians who defend their family members against agencies and individuals who, through neglect or the intentional desire to do harm or simply to save money, exploit vulnerable people with disabilities.
We’ve witnessed this type of family support in many, many cases, such as that of Stan McDonald, who stopped clinicians and providers from giving unnecessary and dangerous anti-psychotic medications to his son, Andy.
Confusing the causes of isolation
In the law journal article, Salzman brings up many of the same arguments against guardianship that the CPR and the providers have used against congregate care, including the segregation charge. But she doesn’t appear to distinguish between degrees of intellectual or developmental disability.
For instance, Salzman states that when an incapacitated person loses their decision-making power to a guardian, they experience feelings of isolation and helplessness, which leads to a further loss in functional abilities in a “vicious cycle.” But while this might be true for relatively high-functioning persons, it is certainly less true for lower-functioning individuals. And it incorrectly assumes that all guardians, including family members, act as dictators and don’t solicit or take into account their wards’ wishes.
Salzman also appears to identify the wrong causes of the isolation she refers to. She argues that persons with developmental disabilities feel isolation due to guardianship and to living in large institutions. But we have found that the isolation felt by these individuals is not due to guardianship or living in institutions, but actually to living in community-based settings.
There is often little real community integration in these privatized settings despite their being characterized as community-based. Unfortunately, there are usually few if any other choices available to guardians among residential settings because so many congregate-care settings have now been shut down and because states like Massachusetts fail to inform people waiting for residential placements of either congregate-care or state-operated sites that remain.
The lack of congregate-care options combined with the privatization of residential care appear to have actually increased the isolation of both individuals with disabilities and their families. Family-supported networking organizations have disappeared as developmental centers have been shut down. People with developmental disabilities are often trapped in group homes in which they are rarely taken out into the community.
In Connecticut, families have lately protested the planned privatization of state-run group homes, with one family filing a lawsuit to preserve their current facilities. There are huge amounts of money to be made in privatization, in particular, and families seem to get in the way of that process.
As we noted, SDM may well work for high-functioning people, but we believe there would nevertheless have to be strict controls on it. We think that means, at the least, that corporate providers should not be permitted on the SDM “network” teams.
For lower-functioning people, our concern is that even if family members enter into SDM voluntarily, they may not realize that their decision-making power may well be diluted under those circumstances. Why would a family member want to agree to be just one vote on a team when it comes to the care of a son, daughter, brother, or sister? We are all for limited guardianships when appropriate, but that team approach doesn’t make sense to us unless it is clear that the family member has the final say in all decisions.
Rather than eliminating guardianship, it would seem we should continue to work to improve the system, particularly for incapacitated individuals and their families. One reform is to ensure that attorneys are appointed to represent all individuals under guardianship if it is requested. Another is for the Legislature to finally pass Stan McDonald’s bill that presumes family members to be the most suitable guardians for their loved ones.
More than six months later, Andy McDonald still has no legal representation in his guardianship case (with update)
UPDATE: A new attorney for Andy McDonald will be appointed this week (the week of September 5) to represent him in his guardianship case, according to Mark Larsen, the director of the Mental Health Litigation Division of the Committee for Public Counsel Services (CPCS), the state’s public defender agency.
After letting us know on Friday that his agency would “look into” why the Middlesex County Probate Court has failed since last March to appoint an attorney to represent Andy McDonald, Larsen emailed me on Sunday (Sept. 4) with news of the imminent appointment.
The failure of the probate court to appoint attorneys to represent developmentally disabled or otherwise incapacitated persons is apparently a persistent problem in Massachusetts.
In his message on Friday, Larsen stated that appointments of attorneys in guardianships are “made as needed” and requested from lists that the CPCS provides to the probate court. I asked Larsen via email how these lists are compiled and whether the attorneys are recommended by the Department of Developmental Services. Larsen said he will be out of the office until September 19 and will respond to my question at that time.
It has been more than six months since Andy McDonald’s attorney in his guardianship case resigned, and no one has yet been appointed to replace that previous attorney, according to Andy’s parents.
In addition, no up-to-date, independent clinical evaluation of Andy, who is intellectually disabled, appears to have yet been done. Such an evaluation has long been advocated by Andy’s parents, Stan and Ellen McDonald, and by the McDonalds’ local legislators and COFAR.
We’ve written about the McDonald case many times already, but it seems that every time we check in on the case, there has been some new development that works to the disadvantage of Andy and his family.
As we’ve previously noted, Andy’s parents, Stan and Ellen McDonald have been trying to overcome a devastating and factually inaccurate probate court ruling from a decade ago in which a judge concluded that Andy is so dangerous that he must be banned for life from ever returning to his hometown of Sherborn, where Stan and Ellen still live.
Stan is now 81 and Andy is 49, and Stan is not sure how much longer he will be able to visit Andy in his group home in Northborough. Stan and Ellen maintain that Andy is not dangerous and should be allowed supervised visits home. They note that even John Hinkley, who shot President Ronald Reagan in 1981, was permitted to leave institutional care last month and go back home to live with his mother, based on updated clinical evaluations.
Yet, none of those factors appears to have had any effect on the way the probate court system and the Department of Developmental Services continue to treat Andy and his family. Andy continues to be denied visits home; Stan and Ellen are rarely even informed about major events or issues regarding Andy’s guardianship; and as I noted, the Middlesex County Probate Court has failed even to appoint an attorney to represent Andy, as required by law.
The state’s Uniform Probate Code (M.G.L. c. 190B, s. 5-106) states that the probate court must appoint an attorney for a developmentally disabled or otherwise incapacitated person in a guardianship case if such an appointment is requested.
Last March, when Stan and Ellen arrived at the Middlesex Probate Court to attend a hearing held to appoint yet another third-party guardian for Andy, they were told that Andy’s court-appointed attorney in the case had resigned as of that day. While that DDS-recommended attorney had also not advocated for home visits, at least Andy was technically represented legally in the case.
During a break in that March 17 hearing, the then attorney told Stan that she would work with Andy’s new guardian to ensure that a new, “experienced” attorney was appointed as soon as possible to replace her. Stan said this week that as far as he knows, that hasn’t happened.
On August 1, Stan contacted the Committee for Public Counsel Services (CPCS), the state’s public defender agency, for help in getting an attorney appointed for Andy, and was told that same day by an administrator there that the organization would inquire about “getting a successor counsel appointed.” He said he has not heard anything further about the matter.
Since Stan and his former wife voluntarily relinquished their guardianship of Andy in 1986 as part of a custody battle, Andy has lived under a series of court-appointed guardians. Like many people who lose or fail early on to secure guardianship of developmentally disabled members of their families, Stan and his current wife, Ellen, have been repeatedly stymied in their efforts to obtain that guardianship.
As a result, the courts and DDS view Stan and Ellen as having no no legal standing to request a clinical evaluation of Andy or anything else relating to the case. For years, they have had to watch helplessly as court-appointed guardians, who have hardly known Andy and rarely visited him, have made major decisions about his care.
The need for an up-to-date, independent, clinical evaluation
In light of the 2006 probate court decision that concluded that Andy was dangerous, Stan and Ellen believe an independent clinical evaluation is the only way to bring about the approval of home visits for Andy. In fact, it’s not clear that any clinical evaluation was done by DDS when Andy’s latest guardian was formally appointed earlier this year.
The Uniform Probate Code requires that a petition filed for a new guardianship of a developmentally disabled individual include a “clinical team report” done within the previous 180 days. Stan said he asked for a copy of that clinical team report and was told by Andy’s DDS service coordinator that it was confidential and that he would not be allowed to see it.
Stan added that if a clinical team did in fact evaluate Andy within the past year, such a team never sought either his or Ellen’s input in that evaluation. Yet, as Andy’s parents, Stan and Ellen do appear to have at least some legal standing in Andy’s guardianship case, even if they aren’t his legal guardians.
In a recent Supreme Judicial Court case (Guardianship of B.V.G.), the high court ruled that anyone interested in the well-being of an incapacitated individual in a guardianship case is considered under the Uniform Probate Court to be an “interested person” in those proceedings. As such, they should be afforded certain rights, such as visitation rights.
Moreover, the court in the B.V.G. case specifically noted that the probate code requires that an incapacitated individual’s changed behavior and “expressed desires” be considered in decisions made by their guardians. Not only should a guardian consider the incapacitated person’s expressed desires, but the guardian has a duty to immediately notify the court if the person’s “condition has changed so that he or she is capable of exercising rights previously limited.”
Andy has expressly stated to his family and in open court his desire for home visits; and his behavior has reportedly been exemplary for more than a decade.
This leaves us with a number of questions. Has Andy’s new DDS-appointed guardian been working to keep the court informed about Andy’s current behavior and expressed desires, and has she pushed for an independent clinical evaluation of Andy? Most immediately, why hasn’t a new attorney been appointed to represent Andy?
The lack of legal representation and an independent clinical evaluation are just two of the many ways in which the system appears to have continued to fail Andy and his family just as it continues to fail countless other individuals with developmental disabilities and their families.
Proposed changes to DDS behavioral and restraints regs would subtract protections, add vagueness
The Baker administration is proposing major changes to regulations governing behavior modification techniques and restraints that are used on persons with developmental disabilities.
The Department of Developmental Services claims these changes will enable disabled individuals “to grow and reach their maximum potential,” and will limit or eliminate the use of certain types of controversial restraints, which are used during behavioral emergencies. We read the proposed changes differently, however.
In our view, the proposed changes would eliminate a large number of specific requirements and restrictions on behavioral techniques and restraints, and replace them in most cases with more vaguely worded provisions that will provide less protection against potential abuse.
For instance, DDS is proposing to scrap the current regulatory definitions of chemical, mechanical, and physical restraints as well as many of the procedures specified in the current regulations regarding those restraints. These procedures would be replaced by a process called the “Crisis Prevention, Response and Restraint curriculum” (CPRR).
It’s not clear in the proposed regulations what the CPRR curriculum is. The proposed language states that the CPRR curriculum uses “Positive Behavior Supports as the framework,” but, as I discuss below, the proposed regulations are equally vague about what the Positive Behavior Supports (PBS) involve.
According to the proposed regulations, the CPRR curriculum will or already does contain a list of “acceptable restraint techniques.” But the proposed regulations don’t appear to specify what those acceptable techniques are. Nevertheless, the proposed regulations state that there is a list of DDS-qualified CPRR Curriculum providers who will apparently instruct DDS residential and day program providers in CPRR procedures.
As noted, a lot of specific requirements in the current regulations would be deleted in the proposed regulations. For instance, requirements would be deleted that mechanical and physical restraints be authorized by either the provider agency head, an authorized physician, or a designated staff member who has had training in the safe use of those procedures.
Also deleted is language stating that any mechanical device used as a restraint must must allow for “the physical and emotional comfort of the individual in restraint.” In addition, the current regulations state that locked mechanical restraint devices requiring the use of a key for their release are prohibited. This statement is deleted as well in the proposed regulations.
It’s possible that all of these requirements are contained in the CPRR curriculum; but we think these requirements should still be spelled out in regulations, which carry the force of law.
The CPRR curriculum, whatever it is, could be changed at any time and would seem to leave it up to the discretion of DDS and the unspecified curriculum providers as to what types of restraints are acceptable and how they should be used. That could make it difficult for families or guardians to challenge the use of restraints on their loved ones if they believe those restraints are being used excessively or abusively.
This does not appear to us to be a good direction for DDS to take given the fact that the use of restraints has become increasingly controversial in recent years.
Regarding the allowable duration of restraints, the proposed regulations would appear at first glance to be an improvement over the current regulations; but even here, the proposed language appears more ambiguous than the current language.
The proposed language states that no individual can be restrained for more than 60 minutes. The current regulations allow for continuous restraints lasting up to 6 hours, and state that non-continuous restraints cannot last more than eight hours in a 24-hour period. But while the proposed language would appear to be an improvement in that regard, the language does not specify whether the 60-minute time limit applies to use of non-continuous restraints. In other words, the proposed language does not appear to prohibit multiple uses of restraints on an individual in one 24-hour period, with each use lasting 60 minutes.
Also, the proposed regulations would prohibit “chemical restraints,” which involve the use of anti-psychotic medications during behavioral emergencies. But anti-psychotic medications would still be permitted as part of an individual’s behavioral treatment.
NOTE: We do support a proposed change in the regulations that appears to introduce a specific prohibition against physical restraints that causes pressure on the lungs. Specifically prohibited under this section would be restraint in a prone position in which the individual is lying on their stomach.
Proposed changes in behavioral modification regulations
In the same set of regulations, DDS is proposing to scrap the term “behavior modification” and replace it with “positive behavior supports” (PBS). As noted above, these proposed changes raise similar concerns for us in that there seems to be less specificity in the proposed PBS system than in the current requirements, many of which would similarly be deleted.
The proposed regulations don’t even appear to clearly define PBS as much as make vague statements about the proposed system. The proposed language states, for instance, that:
PBS emphasizes the use of positive behavior approaches and recognizes that behavior is often an individual’s response or reaction to the environment and the need to communicate his or her preferences and wants to others, and, therefore, PBS focuses on environmental modifications and antecedents.
At the same time, the proposed regulations delete all references to “Level I and Level II behavioral interventions,” which are described in detail in the current regulations. These Level I and II categories appear to be replaced by “Universal and Targeted Supports,” which seem to have much more vague definitions.
The current regulations specify that Level I interventions include such things as positive reinforcement, corrective feedback, and “contingent exercise,” and “time outs” of 15 minutes or less with staff present in the room. The current regulations also state that Level II interventions include procedures that require some “physical enforcement,” and time outs of 15 minutes or less with staff present just outside the room.
In contrast, no actual examples are provided in the proposed regulations of Universal or Targeted supports. Targeted supports are defined as “practices that are implemented fairly rapidly on an ‘as needed’ basis for an individual or group of individuals at risk for developing problem behavior…” There is no indication what those practices might be.
The proposed regulations do appear to leave in place current language regarding Level III interventions, which is the most intensive level of behavior modification techniques under the current regulations. The current regulations state that Level III interventions include such things as contingent skin shock and time outs lasting more than 15 minutes. It is not clear, though, whether there is a relationship in the proposed regulations between Level III interventions and a new category called “Intensive Supports” in the proposed regulations.
In fact, there appears to be no definition or examples of Intensive Supports in the proposed regulations. The proposed regulations state that Intensive Supports should be used “when there are concerns that the health, safety, or emotional well-being of the individual, or others, is at risk, or the individual’s quality of life is seriously impeded due to challenging behavior.”
There also appears to be some confusion in the proposed regulations over the permissibility of skin shock and some other Level III interventions. In one section, the proposed language states that contingent skin shock and seclusion are prohibited practices that “are not be permitted under any circumstances.”
Yet, contingent skin shock is still listed under Level III interventions in the proposed regulations as being acceptable if it is determined that the risks as weighed against the benefits of the procedure would not pose an “unreasonable degree of physical or psychological harm.”
Also, while seclusion would be prohibited under the proposed regulations, the regulations would, as noted above, still permit time outs, which are defined as the placement of an individual alone in a room. Under the Level III intervention requirements, time outs of longer than 15 minutes are permitted if they don’t pose an unreasonable degree of physical or psychological harm.
Other deletions in the proposed changes to the behavioral modification regulations
Also included in the deleted language in this section is a requirement that behavior modification treatment plans are subject to Individual Support Plan (ISP) requirements. ISPs are written plans of supports and services for individuals that are subject to separate regulatory requirements.
The proposed behavioral modification regulations state that a “PBS Plan” would be needed for Targeted and Intensive Supports, but the proposed language does not indicate how such a plan would relate to an individual’s ISP.
Other proposed changes in the this section of the regulations include the apparent replacement of an Advisory Panel for behavior modification interventions with a “Leadership Team” for PBS interventions. At least some of the current requirements regarding qualifications of clinicians on the Advisory Panels appear to be lessened in the proposed language regarding the PBS Leadership Teams.
For instance, membership of the proposed Leadership Teams must include one senior level “qualified clinician.” A qualified clinician is defined in the proposed regulations as holding a master’s degree in psychology or another “relevant discipline” and having at least 5 years of clinical background in developmental disabilities.
Under the current regulations, the behavioral modification Advisory Panels must have at least five members, “a majority of whom shall possess doctoral level degrees in psychology, with significant training and experience in applied behavior analysis and behavioral treatment” (my emphasis).
Proposed change to privacy rights of persons with developmental disabilities
Finally, we strongly oppose a proposed change a separate section of the regulations regarding the privacy rights of persons with developmental disabilities.
Current language in this section requires that “assistance (be provided) by same gender staff for hygiene and medication administration when the partial or complete disrobing of the individual is required.” DDS is proposing to add the phrase “to the extent possible” to this language. We believe this change would have a potentially negative impact on the privacy and dignity of persons in the DDS system, and would increase the potential for abuse of those persons.
In our view, the proposed language would give providers virtually complete discretion to determine whether same-gender privacy protections were possible to provide; and we believe providers would base their decisions regarding the use of same-gender staff on their staffing needs rather than on the privacy and dignity of persons in their care.
We recognize that there may be appropriate and warranted preferences by individuals or their families or guardians for care by staff of a different gender, and we would welcome new language in the existing section of the regulation that would reflect those preferences.
In sum, we think DDS needs to go back to the drawing board with respect to this entire set of regulatory changes. At the very least, the Department should re-insert the specific protections it has deleted regarding restraints and behavioral supports.
Baker administration concedes some congregate care for the developmentally disabled is good, but will still largely prohibit it
In responses to comments made to a federally required plan for community-based care of the developmentally disabled, the Baker administration is conceding that not all congregate care is bad or should be banned.
Yet, the administration’s draft Statewide Transition Plan (STP) still appears to prohibit or restrict most new group homes from housing more than five residents; and it would apparently restrict funding for most other congregate settings, such as farm-based residential programs. The administration is currently asking for further comments on the draft STP.
The STP is a requirement of the federal Centers for Medicare and Medicaid Services (CMS), which issued a new regulation in 2014 governing community-based care receiving Medicaid funding. The CMS regulation is intended to reduce reliance on congregate care, but Massachusetts originally appeared to go even further than the CMS regulation in banning congregate care almost entirely.
Along with hundreds of people and other organizations, COFAR submitted comments in late 2014 to the original draft of the STP. It appears that like us, most of the commenters to that original plan were concerned that the state was going too far in banning virtually all possible forms of congregate care.
As we noted in our comments to the administration in 2014, the Department of Developmental Services appeared to be proposing a ban on new and potentially existing residential settings such as farmsteads, residential schools or settings that are part of residential schools, settings “that congregate a large number of people with disabilities for significant shared programming and staff,” and even new group homes with more than five residents. Not even CMS was advocating a complete ban on all of those residential options.
Now, after having received those critical comments, the state seems to be willing to continue to fund some forms of congregate care.
In its response to the comments, the Baker administration made the following statement:
The state acknowledges that CMS… has indicated that ‘it is not the intent of this rule (CMS’s 2014 regulation) to prohibit congregate settings from being considered home and community-based settings.’ The …characteristics of any setting (location, geography, physical characteristic and size) are not necessarily determinative of whether a provider can achieve compliance… (my emphasis).
Despite that apparent concession, the Baker administration’s STP states that DDS has determined that 14 corporate providers operating 57 group home sites are not complying with the new CMS regulation. This lack of compliance is because these residences apparently have “institutional qualities,” either because they house more than five residents or not enough services are provided by community-based providers.
The STP also states that some of these homes may have provided insufficient staff training in “person-centered planning.” (We have voiced concerns that while person-centered planning is touted as giving developmentally disabled individuals more control over the services they receive and how they pay for them, the process appears to put control over an individual’s funds into the hands of private companies.)
By the way, the administration stated in its responses to the STP comments that the state’s Building Code limits group home capacity to five residents. Our reading of the applicable Building Code regulation, however, is that it does not set a 5-person limit on all group homes, but rather specifies only that DDS group homes with five residents or less must be classified as single-family or two-family homes (see amendments to 780 CMR. 310.2).
These are, moreover, group homes, and not developmental centers, that DDS has identified as being too institutional. This raises a concern for us that the federal government and the state are pushing for ever smaller and more dispersed residential settings — a process that diverts more and more taxpayer money appropriated for the developmentally disabled into a grossly unregulated corporate-run service system.
While it appears under the STP as though DDS will allow these 14 providers some leeway in complying with the provisions in the plan, the providers will have to make a range of changes, including potentially relocating their residents to smaller residences. The STP indicated that this may result in an unspecified additional cost to the state.
The STP also noted that the Association of Developmental Disabilities Providers (ADDP), an influential lobbying organization for state-funded DDS providers, will be in charge of providing assistance to the providers in complying with the plan.
Anti-eviction agreements
One piece of potential good news is that the administration’s STP states that DDS will require providers to sign contractual agreements with residents of group homes that prevents arbitrary and capricious evictions. This is apparently another CMS requirement. This could address one of the key problems we’ve identified with provider-operated group homes, which is that they can currently evict residents with minimal notice, particularly in cases in which guardians or other advocates are seen as being pushy or meddlesome.
A portion of the STP also deals with non-residential care. What stood out was that DDS found that 170 community-based day programs operated by 98 providers did not meet CMS standards due to inadequate daily activities, staffing, and funding.
Administration still steeped in community-first ideology
Despite the apparent softening of its anti-congregate-care position, the administration’s STP still appears to be ideologically opposed to anything not considered sufficiently community-integrated, and therefore too institutional. In its response to some of the comments to the STP, the administration stated that it is its belief that:
…all individuals, regardless of their level of impairment, can benefit from integration and access to the community. (my emphasis)
The administration made this statement after noting that it recognized that “…individuals with significant disabilities live in some settings that presumptively do not satisfy the (CMS) community regulation.” The administration stated that it is not its intent “to force individuals to move from settings or to take away needed services and supports.” But that is exactly what DDS did when it closed or downsized four developmental centers in Massachusetts, starting in 2008.
So, in effect, while the administration says in the STP that it recognizes that some individuals live in non-community-based settings, it still maintains that all developmentally disabled individuals, regardless of their level of disability, could benefit from being moved to the community system. It is a community system, however, in which at least some of the services and supports available in “institutional” settings would most probably be taken away.
On the one hand, the administration acknowledges that it is not the size of a care setting that determines whether it is institutional or not, but rather the services provided and the commitment of the staff. Yet the administration consistently overlooks the fact that just because a care setting is small, that doesn’t guarantee it will be integrated into the community.
In a perceptive post, Jill Escher, president of The Autism Society San Francisco Bay Area, notes that the real purpose of the new CMS regulation is not to eliminate institutional care, but rather “to put the brakes on the creation of new residences and programs that cater specifically to adults with autism and other intellectual and developmental disabilities.”
In other words, programs for the developmentally disabled cost money, and the CMS is looking to save money by simply eliminating those services.
Here’s Escher’s very apt description of the impact of the CMS regulation and the transition plans of states like Massachusetts:
Though the (CMS) rules talk of “person-centered” and “outcome-oriented” services, where individuals are not “isolated” and are free from coercion and restraint, in Orwellian doublespeak fashion, civil rights and liberation is not the true endgame here. The overwhelming goal is to restrict out-of-home options.
In practice the rules mean if you’re sitting at your parents’ home doing nothing, or in your own apartment without on-site staff, that’s “community integration.” Meanwhile if you prefer a well staffed adult autism program or housing complex, where you are cared for and safe, engaged in the community, and in the company of your friends who may have similar disabilities, your choice is ironically deemed “isolating” by bureaucrats. And therefore subject to the CMS axe.
Jill Barker, who writes The DD News Blog, adds:
Congregate care, providing services to people with disabilities in group settings, is one of many practical solutions to the need for long-term care. It allows for the sharing of resources and lessening of feelings of isolation. It should not be ruled out as an option, although that appears to be the intent of many advocacy organizations.
In my opinion, there is also a quiet war on families who are offered no other alternative but to keep their adult child with DD at home with services that may not be adequate to provide the family with the relief they need and a good quality of life for their disabled family member for the long term.
The Massachusetts Legislature and governor are leaving the state’s most vulnerable citizens behind
After wrapping up its annual budget deliberations last month, the Massachusetts Legislature is practically done for the year.
There are a couple of formal sessions of the House and Senate still to be held before the end of July, and then there will be only “informal sessions” through the end of the year, which are usually for things like renaming streets. The two-year-long 189th session of the General Assembly will then come to an official end at the beginning of January of next year.
Unfortunately, you have only to glance through our July newsletter to see how little both the Legislature and the administration of Governor Charlie Baker have accomplished when it comes to the care of people with developmental disabilities. Here are some examples from the newsletter:
The Fiscal Year 2017 state budget
When it comes the Fiscal 2017 budget, the Legislature essentially rubber-stamped the funding proposals submitted last January by Baker for programs for the developmentally disabled (“‘Dismal’ FY ’17 budget approved for DDS,” Page 1).
In most of the cases in which the Legislature did make changes to the governor’s budget, the changes were not good. With only one or two exceptions, the funding proposals approved by the Democratic-controlled House and Senate were actually lower even than what the Republican governor had proposed.
As the newsletter points out in an article on Page 3, one of the Legislature’s most egregious failures was its refusal to go along with Baker’s proposed funding for a program to place disabled people in jobs in the mainstream workforce (“Legislature fails to fund jobs programs for DDS clients”). This budgetary line item was supposed to ensure that developmentally disabled persons being moved out of sheltered workshops, which are being closed by the Baker administration, would ultimately be placed in mainstream jobs.
COFAR has strongly opposed the sheltered workshops closures, arguing that those jobs in the mainstream workforce don’t really exist to replace the workshop programs. But the Legislature bought into the closures of the workshops in Fiscal 2015 by providing enough funding to the Department of Developmental Services to transfer hundreds of clients out of the workshops and initially into DDS day programs.
For the current fiscal year, however, the Legislature has not only approved $4.6 million less for the mainstream workforce jobs line item than Baker proposed, but both the Legislature and Baker are underfunding the separate day program line item by $10 million. The result will be more crowded day programs with less staff and less meaningful activities for the clients.
As the newsletter notes on Page 3, the Legislature did approve a $100,000 increase in the budget of the Disabled Persons Protection Commission, which Baker had proposed level funding. But that is less than a 2 percent increase from the previous fiscal year when adjusted for inflation, and is less than the $350,000 increase that the Senate itself had proposed.
The family rights bill
For 17 years, State Representative David Linsky has filed a bill in the Legislature that would boost the rights of family members in guardianship cases involving persons with developmental disabilities. The bill would require probate judges to presume a disabled person’s parents are suitable to be his or her guardian.
This session’s version of the bill (H. 1459) seemed for a while to have a degree of political momentum that it had never had in past years in which it would perennially die in committee. For the first time, the bill received the endorsement of the Massachusetts Developmental Disabilities Council (MDDC). The MDDC, a state-run organization that identifies priorities for care for people with those disabilities, listed the bill as one of its legislative priorities for 2015- 2016.
While the bill has long had COFAR’s support, it was also supported in this session by the Arc of Massachusetts. In fact, we know of no advocacy organization that opposes the measure. And yet the bill remained stuck in the Judiciary Committee for more than a year.
In January of this year, both Rep. Linsky and state Senator Richard Ross wrote a letter to the Judiciary Committee co-chairs, urging them to report the bill out of the committee favorably so that the measure could reach the floors of the House and Senate for enactment. Ross and Linsky are the local legislators of Stan McDonald, who has been fighting for years to gain guardianship of his developmentally disabled son, Andy.
Despite all of that support for H. 1459, the Judiciary co-chairs — Senator William Brownsberger and Rep. John Fernandes — sent the bill in March to a study, a euphemism for legislative death. (See our story on Page 5 of the newsletter: “Guardianship bill dies in committee.”)
We are still at a loss to explain why this critically important bill never gets past the committee stage in the legislative process. We think it may be that the bill is actually opposed by DDS, which does not want to lose any of its power in recommending attorneys and corporate entities as guardians of developmentally disabled individuals.
The medical training bill
After reporting on a case in which an intellectually disabled man died after having been repeatedly turned away from a hospital, we were initially heartened to see that a bill had been filed in the Legislature to require that medical personnel receive training in treating people with developmental disabilities.
The hospital case appeared to raise questions about the ability of the emergency room staff at the hospital to correctly diagnose the condition of the man who may have been non-verbal. However, the bill, like the family rights bill discussed above, appeared to be stuck in committee — in this case, the Public Health Committee.
In March, it briefly appeared that the bill (H. 1932) would advance in the legislative process. We received a notification from the Public Health Committee that the bill had been approved. But less than a month later, we found out that the committee co-chairs had actually authorized a substitute bill (S. 2211) in place of the original bill, and had done that behind closed doors and apparently without a vote of the full committee.
Instead of requiring training of hospital personnel in the treatment of developmentally disabled persons, the new bill expands an existing training and accreditation program operating in four medical and nursing schools. (See our story on Page 5 of the newsletter: “Committee quietly changes medical training legislation.”)
The training and accreditation existing program, known as Operation House Call, has been run by the Arc of Massachusetts for several years. The program provides instruction to medical and nursing school students in treating people with developmental disabilities in hospital settings, including people with autism. While Operation House Call appears to be a worthwhile program, it is much more limited in scope than what had been proposed in the original legislation.
In addition to requiring the training of actual hospital personnel, the original bill (H. 1932) would have required the Executive Office of Health and Human Services to evaluate discrimination against developmentally disabled persons and to issue regulations to reduce the impact of “disparities in outcomes” for those people in medical settings. That provision was not included in the new bill (S. 2211).
Despite its reduced scope, it now appears that even S. 2211 will never see the legislative light of day. A staff member of the Health Care Financing Committee, to which the bill was referred in April, told us today that the committee had referred the bill to a study (just as in the case of the family rights bill, discussed above).
Other DDS bills remain in limbo
Meanwhile, a whole slew of other DDS-related bills have been stalled for months in the House and Senate Ways and Means Committees, and their fates remain uncertain at best. The bills include measures to expand Turning-22 services (S. 2223), expand civil rights protections to persons with disabilities (H. 121) , and to create new housing for persons with disabilities (S. 2202).
Unless these bills are reported out by those committees before the end of this month, they would have to be approved during the informal session period. It seems unlikely that substantive bills such as these would be approved in informal sessions in which just a few legislators are present and in which each measure could be derailed based solely on an objection by one member. We’re not sure it’s even good public policy to approve substantive legislation in informal sessions.
What the Legislature and the Baker administration have accomplished has been to consistently boost funding for privatized care at the expense of state-run care. What they haven’t done is to address the many interrelated problems and issues that are endemic to the DDS system.
Those issues include continuing abuse and neglect in the largely privatized group home system. They include the marginalization of families by DDS, its providers, and the probate court system in the decision making regarding care of persons with developmental disabilities.
Those problems also include high rates of incarceration of persons with developmental disabilities in prisons. In our newsletters and blog posts, we have detailed two of these cases — one in which an intellectually disabled man was placed for an indefinite period in the Worcester House of Correction following an alleged fatal assault, and another in which an intellectually disabled resident of a group home continues to face criminal charges following an assault on staff workers.
We can’t remember the last time any legislative committees have even held hearings on these pressing and interrelated issues. A truly caring legislature and administration would work together on behalf of their state’s most vulnerable citizens. The State of Massachusetts is instead leaving its most vulnerable citizens behind.
Limited federal IG probe faults state’s reporting on group home abuse in MA
In one of the few investigations of the community-based system of care for the developmentally disabled, the Inspector General for the U.S. Department of Health and Human Services last week disclosed critical shortcomings in the process in Massachusetts for reporting abuse and neglect.
A report issued by the IG found that incidents of abuse and neglect in group homes were not regularly reported to investigators. The report noted that of a sample of 587 visits by group home residents to hospital emergency rooms, the group homes had failed to report 88 –or 15 percent — of them to the Department of Developmental Services.
In addition, DDS itself and the group homes did not report 58 percent of 175 “critical incidents” to the Disabled Persons Protection Commission, as required by state regulations. And 29 percent of incident reports sampled by the IG did not contain “action steps” to protect individuals involved from future injury.
COFAR has long maintained that the state’s privatized group home system is inadequately overseen and prone to abuse and neglect due to relatively low levels of pay and training, and high turnover among staff. Even the providers themselves acknowledge those problems. Yet the state routinely relicenses the providers to operate homes even though there are clear gaps in the prevention and reporting of abuse and neglect.
The Massachusetts report is the third report issued by the HHS IG thus far on abuse and neglect in individual states. Last year, the IG issued a report on New York State; and in May, the agency issued a report on Connecticut.
U.S. Senator Chris Murphy of Connecticut, who originally requested in 2013 that the HHS IG investigate abuse and neglect in group homes around the country, commented this week on the findings, at least concerning Connecticut and Massachusetts. In a statement issued on Monday, Murphy said he will introduce federal legislation to require reporting of incidents of abuse and neglect, and training of direct care staff in group homes.
Murphy’s office did not respond to a request from COFAR earlier this year for comment on the New York report. As we noted in February, the New York report contained no recommendations and no critical findings, and was only six pages long.
The Massachusetts report, in contrast, was 33 pages long. Like the Massachusetts report, the Connecticut report, which was issued in May, found numerous failures to report abuse and neglect to state authorities.
Despite its thoroughness in examining the incident reporting process in Massachusetts, we believe even the IG’s Massachusetts report was limited in its scope. We think it could have gone much further in investigating the major problems posed by the privatized residential system.
In requesting the IG investigation, Murphy’s 2013 letter to Daniel Levinson, the HHS IG, emphasized the role of privatization in causing “a race to he bottom in our health care system. Privatization of care may mean lower costs but without the proper oversight and requirements for well-trained staff,” Murphy stated.
In limiting its report primarily to findings of failures to report instances of abuse and neglect, the IG has focused on a small piece of the overall problem. The larger issue concerns not only the level of abuse and neglect in the privatized system, but the overall adequacy of care that exists in it.
The HHS IG report did not examine the impact of privatization on the quality of care in the group home system, and did not specify whether the residents whose emergency room visits the IG sampled lived in privatized or state-run group homes.
We have found that the state’s ongoing privatization of residential services has resulted in a corporate, bottom-line approach to care of the disabled. Moreover, DDS has insisted on steering people waiting for residential care to the privatized group home system, all the while failing to provide state-run homes as an option.
The case of Kathleen Murphy is an example. As we have previously reported, Kathleen’s sister and guardian, Patricia Murphy, and members of her family began trying to move Kathleen from a corporate provider-operated group home to a state-operated residence in 1998. DDS continually declined to move her, despite a federal law requiring that the Department provide disabled individuals with a choice among all available alternatives for residential care.
Patricia Murphy finally filed a federal lawsuit in 2013, which resulted in the placement of Kathleen in a state-operated residence. (By way of disclosure, Kathleen Murphy is represented in the case by Tom Frain, who is COFAR’s Board president.)
Patricia Murphy contends that Kathleen suffered nearly 16 years of physical abuse, sexual assaults, emotional torment, and medical neglect in provider-operated group homes. She says her sister was also grossly over-drugged in those facilities, and her clothing, jewelry and spending money were stolen.
The state-operated residence to which Kathleen was finally placed is “the best thing that ever happened to her,” Patricia said. She said that since moving to the state-operated group home, Kathleen has lost 45 pounds, is being fed nutritious food, is off all psychotropic drugs, and her blood pressure is under control.
Yet these experiences as reported by families are apparently of little interest to the federal government, in particular, which, like the state, is committed to further privatization of residential services for the developmentally disabled. While the U.S. Department of Justice has placed a major emphasis in recent years on investigating and closing down state-operated facilities and services for the disabled, there have been few if any comprehensive investigations of the privatized group home system.
Unfortunately, the Massachusetts Legislature has adopted a look-the-other-way attitude regarding these problems. As far as we know, no legislative committee has scheduled any hearings in recent memory on the problem of abuse and neglect in the DDS system.
Both the Legislature and the Baker administration have continued a policy of boosting funding for further privatization of services while slowly starving the much more responsive state-run group home system of budgetary support.
We hope that the IG report, limited as it was, spurs the Legislature to finally pay attention to the big issues that surround the care of persons with developmental disabilities in Massachusetts. Those issues concern privatization and its impact on abuse, neglect, and the quality of care in general.
SJC decision could help family members denied contact with developmentally disabled loved ones
In a decision that could boost the rights of family members in guardianship disputes, the Massachusetts Supreme Judicial Court ruled last month that the grandfather of a young, intellectually disabled woman has the right to intervene in a probate court proceeding in order to gain permission to communicate with her.
It appeared the ruling could be applied to other ongoing probate court cases in which family members have been excluded from contact with loved ones in the care of the Department of Developmental Services.
The woman in the case before the SJC was identified as B.V.G. The SJC ruled that even though the grandfather was not B.V.G.’s guardian, he was an “interested person” within the meaning of the state’s Uniform Probate Code. As such, he had the right to intervene in the court proceeding in order to remove restrictions on his contact with his granddaughter.
According to the SJC ruling, B.V.G. had had a “strong relationship” with her grandfather, which both B.V.G. and the grandfather wished to maintain. However, B.V.G.’s father, who was appointed as her permanent guardian, had sought to sharply restrict or prohibit her contact with her grandfather, and, in fact, with all of her other maternal relatives.
COFAR has reported on a number of cases in which guardians of DDS clients have either made or upheld decisions to restrict contact and visitation rights of family members. Those cases have stemmed from the appointment of attorneys and other non-family members as guardians.
In the B.V.G. case, the restrictions on the grandfather’s contact with his granddaughter were imposed by another family member. The SJC ruling noted that the grandfather had been permitted by the father to send B.V.G. only one email message per day, and to receive no more than one email message from her. But the woman did not have access to email at the residential facility where she lived, so the grandfather and granddaughter effectively had no contact with each other.
The SJC noted that the Uniform Probate Code (which is contained in the state’s general laws) allows anyone defined as an “interested person” to intervene in a guardianship proceeding in probate court. A probate court judge had previously ruled in the case that the grandfather of B.V.G. was not an interested person because he was not her guardian and because he did not demonstrate that he had a financial stake in the court proceeding.
But the SJC concluded that an individual can be considered an interested person under the Uniform Probate Code simply by being interested in an incapacitated person’s well-being. As such, the grandfather of B.V.G. was clearly an interested person, the high court concluded.
In one ongoing case on which COFAR has reported, Stan McDonald, the father of a 49-year-old intellectually disabled man, has been fighting for increased contact with his son, including visits by Andy to Stan’s home. Stan’s son, Andy, lives in a group home. Andy is currently barred from such visits, under a 2006 probate court order, which concluded he was dangerous.
COFAR has reported that the 2006 court order contained a number of factual misrepresentations regarding Andy’s alleged dangerousness.
While it would appear that Stan McDonald would be considered under the Uniform Probate Code to be an interested person in his son’s guardianship, Stan has been told that he has no right even to request home visits from Andy or to discuss such visits with him. Stan has even been threatened with contempt of court for doing so.
Stan’s wife, Ellen, who is Andy’s step-mother, was not permitted to attend a recent probate court hearing on the appointment of a new guardian for Andy, even though she, too, appears to meet the SJC’s interpretation of an interested person in the case.
As interested persons, it would seem that the McDonalds should have input into the terms of Andy’s contact with them. Although the 2006 court order barred home visits for Andy due to his alleged dangerousness, the McDonalds have repeatedly called for an independent clinical evaluation of Andy. Their requests have seemingly been ignored, possibly because they have not been considered to have standing in the case.
As we have noted, not only was the 2006 court order banning Andy’s home visits based on factual misrepresentations in the record, but Andy’s general behavior has greatly improved since that decision was issued.
Both the SJC and the Appeals Court noted in the B.V.G. case that the Uniform Probate Court requires that an incapacitated individual’s changed behavior and “expressed desires” be considered in decisions made by their guardians.
The Appeals Court pointed out that not only should a guardian consider the incapacitated person’s expressed desires, but the guardian has a duty to immediately notify the court if the person’s “condition has changed so that he or she is capable of exercising rights previously limited.”
Andy has repeatedly expressed his desire to visit his parents’ home, and even told a probate court judge of his wish last October. As noted, his behavior has changed since 2006. We are not sure that the probate court has been notified about that. We sent a letter about those issues to the former and current judges handling the McDonald case in Middlesex Probate Court, but have received no indication whether our letter would be accepted into the court record.
By the way, in its amicus brief in the SJC case, the Massachusetts Arc also supported the idea of a family member or friend having the right to intervene in a guardianship proceeding “in order to accommodate the inevitable changes during the lifetime of the person under guardianship.” (our emphasis.)
It isn’t clear to us how the SJC decision will affect cases such as the McDonald case, but we hope that it will lead to a change of attitude within both the probate court system and DDS regarding the rights and standing of family members in guardianship cases.
The attorney for B.V.G. stated at the hearing on the grandfather’s motion to intervene that “we all took it for granted that grandfather had no rights…” That presumption needs to change.
House and Senate not following their own funding plan for employment of the developmentally disabled
For the past three years, the state has been carrying out a policy of closing sheltered workshops for people with developmental disabilities and subsequently placing those people in mainstream workforce jobs.
Yet the Legislature, which bought into this policy, is failing to provide the necessary funding for it.
As the Department of Developmental Services and its corporate service providers jointly proclaimed in 2013, the policy has been to move developmentally disabled people out of sheltered workshops and into community-based day programs and ultimately to the mainstream workforce.
Sheltered workshops are settings in which developmentally disabled people work together on simple assembly-line tasks and are usually paid a small wage. The workshops have gone out of favor because they are viewed as “segregating” their participants from their non-disabled peers in the community.
Since 2013, the majority of the remaining sheltered workshops in Massachusetts have reportedly been closed. All are scheduled to be closed as of June 30 of this year.
But the problem is that the Legislature, and to some extent the administration itself, aren’t following through on the policy, which calls for beefing up funding for DDS day programs and job development staffing. Last week, the Senate joined the House in rejecting higher funding levels considered by the policy planners to be needed by both day programs and employment programs for Fiscal Year 2017.
The irony is that the Democratic-run House and Senate have proposed even less funding for these line items for Fiscal ’17 than Republican Governor Baker has.
A likely result of this apparent under-funding is that relatively few people will be placed in mainstream jobs, but rather will be sent to potentially overcrowded day programs with inadequate staffing.
Day and employment accounts were initially increased, but will now be under-funded or cut
In order to accomplish the policy for “integrated employment” of the developmentally disabled, the Legislature initially increased funding of the community-based day program line item in the state budget, and created a new line item to fund the transfers from the sheltered workshops. The idea was to increase both day program and job development staffing and training.
The new sheltered workshop transfer budget line item (5920-2026) was initially funded in Fiscal ’15 with $1 million. That amount was raised to $3 million in the current fiscal year, and the governor proposed to boost it to $7.6 million in Fiscal ’17. But the House and now the Senate are not going with the governor’s plan.
As the House did last month, the Senate last week approved a budget plan for Fiscal ’17 that will eliminate Governor Baker’s proposed $4.6 funding increase for the sheltered workshop transfer line item. Amendments proposed in both the House and Senate to restore the governor’s increase for the line item were rejected by the House and Senate leadership. As a result, the account will be level-funded next year, which amounts to a cut when adjusted for inflation.
Yet, even the governor’s proposed $4.6 million increase in this line item was $1 million too low, according to the Massachusetts Association of Developmental Disabilities Providers (ADDP). The ADDP lobbies on behalf of corporate DDS providers, which operate day and work programs throughout the state.
In addition, the Senate budget approved last week would provide $700,000 less in spending for the community day and work line item (5920-2025) than the amount the House and the governor proposed. The governor and the House proposed a 4.9 percent increase in that account for Fiscal ’17.
In an email sent to members in early May, the ADDP contended that even the 4.9 percent increase in the day and work line item was $9.8 million less than the what was needed to maintain existing services. As a result, according to the ADDP, DDS was already planning to cut 5 percent in funding for contracts with all day and employment providers.
Should the Senate’s budget plan prevail regarding the day and work line item, it would seem the cut in contract funding for day and employment providers would have to be even deeper than 5 percent.
ADDP urged higher funding and staffing for day care and employment programs
Both the ADDP and the Arc of Massachusetts have become virtual partners with DDS in the operation of the department. The Arc and the ADDP co-authored a report with DDS in 2013 that called for the closures of the sheltered workshops as of June 2015. While that goal wasn’t met, DDS is continuing to work for those closures as of this June of this year.
In comments submitted to EOHHS Secretary Marylou Sudders late last year, the ADDP maintained that funding for both the community day and work line item and sheltered workshops transfer line items needed to be boosted significantly in order to fulfill the plans to close the workshops and transfer clients to mainstream jobs. A failure to boost that funding could put the state in violation of requirements issued by the federal Centers for Medicare and Medicaid Services (CMS), according to the ADDP.
The ADDP comments also noted that as of October 2015, the number of individuals receiving community based day services more than doubled from 2,656 individuals as of June 2013, to 5,422. While noting that this increase was directly related to the closures of the sheltered workshops, the ADDP stated that the majority of those persons were not receiving any other DDS-funded employment services.
The ADDP comments also pointed out that DDS day programs require significantly higher levels of staffing than the sheltered workshops did.
As we pointed out in a blog post in January, DDS records show that the number of participants in sheltered workshops dropped by 61 percent between August 2014 and August 2015, and the number of persons in corporate-run community-based day programs increased by 27 percent. Yet, the number of developmentally disabled people in “integrated employment” settings rose during that same period by only about 6 percent.
It appears that the only policy the Legislature and the administration have pursued with a real level of commitment has been closing the sheltered workshops. But that’s only half the plan. The problem with the Legislature, in particular, is that while it bought into the first half of the plan, it now has seemingly abandoned the critically important second half.
Thousands of people have or will be removed from their sheltered workshops, and the Legislature appears to be leaving an unknown number of them in the lurch.
DDS mortality reports show a rise in deaths in the community system since 2008
If you do some intensive searching, you may just find a series of what seem to be fairly well-hidden reports on the Department of Developmental Services website that present data on deaths in the DDS system between the years 2001 and 2013.
We did find those reports, and reviewed them going back to 2008, the year the then Patrick administration implemented its “Community First” initiative. Within DDS, the initiative involved a major push to close large state-run developmental centers and to move the residents of those facilities to community-based group homes.
It appears to be difficult from the data in the reports to draw any firm conclusions about the total numbers of deaths in the DDS system, which have fluctuated substantially in years between 2008 and 2013. There was a low of 406 deaths in 2010 and a high of 438 deaths in 2012.
What did appear to stand out in the data was the significantly higher number of deaths in the community residential system in 2013 than in 2008. There were 196 deaths in the community residential category in 2008, and that number rose to 254 deaths in that category in 2013. That was an increase of 58 deaths per year, or about 30 percent.
The number of deaths in the community system rose in three of the five years between 2008 and 2013. There was a slight drop in the number of deaths in the community system in 2010, and a somewhat larger drop in 2013, the latest year for which the mortality reports are available. Nevertheless, the increase in the number of annual deaths between 2008 and 2013 is statistically significant.
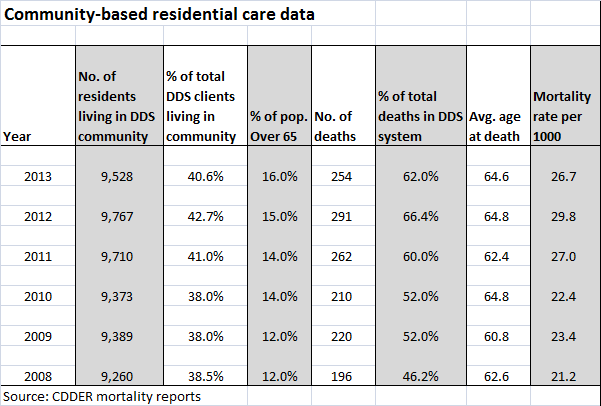
We looked at the mortality report data for two other residential categories within the DDS system — people living at home and people in the remaining developmental centers. We did not review report data for two other categories of residential care — nursing homes, which had a relatively small number of DDS clients living in them during the 2008-2013 period, or for settings listed as “non-DDS facilities.”
In contrast to the community residential system, the numbers of deaths in the developmental centers and living-at-home categories decreased fairly steadily between 2008 and 2013.
The percentages of all deaths in the DDS system rose in the community residential category from 46.2 percent in 2008 to 62 percent in 2013, while the percentages of all deaths dropped in that time in the developmental centers and among people living at home. During that time, the percentage of DDS clients living in the community system increased only slightly — by 2.1 percent.
The data raises some questions. Did the closures of the Fernald, Monson, and Glavin developmental centers, starting in 2008, contribute to the increase in the overall death rate in the community system? Were there people living in those centers who died as a result of having been moved into the community system?
The mortality reports, which were done by the Center for Developmental Disabilities Evaluation and Research (CDDER) within UMass Medical School, do not offer any speculation or answers to that question.
CDDER’s 2010-2011 mortality report does offer some speculation about a statistically significant increase in deaths in the community system between those two years. The report states that the increase may have been due to people with “high medical needs” having been moved into the community at that time from nursing homes. But we found no discussion in any of the reports about the potential impact of moving people into the community from the developmental centers.
The CDDER reports also do not appear to differentiate between corporate-provider-run and commonwealth-operated group homes. The community residential category examined in the reports appears to lump both of those types of residential care together. This allows no comparisons to be made between the state-run and privatized group home systems with regard to the mortality rate.
The CDDER reports do provide the average ages of people in each residential setting. But the reports do not compare average levels of intellectual disability or medical conditions in each category. (Some of the reports did compare the medical causes of death in some of the residential settings, but the data didn’t indicate the percentages of residents in each setting with specific medical conditions such as cancer and heart disease.)
There is a lot of important research contained in the CDDER reports, but the omissions are concerning, though perhaps not surprising. CDDER is under contract to DDS to produce the reports, and they are not going to produce or analyze any data that DDS doesn’t want them to produce or analyze.
For years, we have been critical of the ongoing privatization of DDS services. We have raised concerns about the Patrick and now Baker administrations’ policies of under-funding state-operated care, closing existing state-operated group homes, and preventing people from choosing state-operated care as a residential option.
We have also expressed concern that care in the privatized system is not as well overseen as it should be; that staff in provider-run group homes is often underpaid and inadequately trained, and that provider executives are continuing to make huge salaries nonetheless.
We have also been critical of the closures of the developmental centers, which took place in many cases over the objections of the families of the residents in them.
One would think the DDS-sponsored mortality reports would examine the impact of both the developmental center closures and privatization of services on client deaths among other variables. That is, unless DDS would rather not get into those matters. Based on the reports, it would seem that DDS does not want CDDER looking into the impact of increasing privatization, at least on client deaths.
As a result, we can only glean some hints from the CDDER data about those issues.
According to the reports, the community residential system appears to have grown by about 2.9 percent during 2008-2013 period, which makes sense since people were being moved there from nursing homes and from developmental centers.
The data show that the number of residents of the developmental centers dropped from 925 in 2008 to 550 in 2013 — a 44 percent decrease. Given that the number of residents in the centers was dropping so rapidly, the number of deaths among that population was bound to drop as well. There were 49 deaths in the centers in 2008, and 24 deaths in 2013 — a 55 percent decrease.
Among people living at home, the number of deaths also dropped between 2008 and 2013. There were 69 deaths among people living at home in 2013 — a drop of 18.8 percent from the 85 deaths listed in 2008. The total number of people living at home dropped only by 4.3 percent during that period.
Nursing homes and developmental centers had the highest mortality rates per 1,000 clients among the residential settings, according to the 2012-2013 CDDER report. The report explained that the high mortality numbers in those two settings were due to the relatively advanced age of the residents and their relatively serious health conditions.
As noted, however, the mortality reports don’t appear to have compared medical data among residents living in the various settings. The data do show that an average of more than 30 percent of the residents of the developmental centers were over the age of 65 between 2008 and 2013, compared with about 14 percent of residents in the community and 5 percent of DDS clients living at home.
As of 2013, 550 or 2.3 percent of all DDS adult clients were still living the developmental centers. That year, there were 9,528 clients living in the community system, or 40.6 percent of all DDS clients; and there were 11,822 clients living at home, or 50.4 percent of all DDS clients.
In sum, there doesn’t seem to be too much that is surprising in the data, other than the apparent increase in deaths in the community system between 2008 and 2013.
We think it’s possible that those transfers from the developmental centers may have contributed to that increase in deaths in the community system. But given that CDDER does not appear to have collected data concerning deaths of former developmental center residents, we may never know the real impact on mortality of the closures of the centers.
And unless CDDER begins differentiating between provider-run and state-operated group homes, we may never know the impact of increasing privatization on mortality rates in residential care.
