Archive
The federal government’s cruel pursuit of deinstitutionalization
When is the federal government — particularly the Department of Justice — going to recognize or admit that deinstitutionalization of the developmentally disabled hasn’t worked as planned?
The DOJ seems to have closed its eyes to the realities on the ground in continuing to file lawsuits around the country to close state-run care facilities. This has caused “human harm, including death and financial and emotional hardship,” according to information compiled by the VOR, a national advocacy organization for the developmentally disabled and a COFAR affiliate.
While the DOJ has not filed such a suit against the State of Massachusetts, that may be because the state has closed, or is in the process of closing, four out of six developmental centers that were in operation as of 2008. But with two developmental centers remaining as well as other programs that the DOJ considers to be institutional, such as sheltered workshops, Massachusetts could well become a target for a lawsuit at any time.
The VOR filed testimony last month, urging a congressional subcommittee to adopt legislative language that would require the DOJ to do two very commonsense things before filing more lawsuits to close state-run facilities:
- First consult with the residents or their legal guardians “to determine residents’ needs and choices with regard to residential services and supports,” and,
- Second, do not “impose community-based treatment on patients who do not desire it.” This second requirement is consistent with the 1999 U.S. Supreme Court decision in Olmstead v. L.C.
The DOJ’s continued pursuit of class-action litigation to close developmental centers and other facilities has led to the irony that those lawsuits are generally opposed by the families of the residents on whose behalf the suits are ostensibly filed. As U.S. District Court Judge J. Leon Holmes wrote in 2011 in dismissing a lawsuit brought by the DOJ against the State of Arkansas to close the Conway Human Development Center center there:
…the United States is in the odd position of asserting that certain persons’ rights have been and are being violated while those persons – through their parents and guardians – disagree. (U.S. v. Arkansas, June 8, 2011, dismissal order).
Judge Holmes’ decision noted that evidence in the case showed that the parents and guardians of residents of the Conway Center “are overwhelmingly satisfied with the services there and believe that the Center is the least restrictive, most integrated placement appropriate for their children and wards.” Moreover, the judge’s decision stated that the weight of the evidence in the case failed to support the DOJ’s contention that care at the Conway Center was substandard.
The VOR notes that the DOJ’s Civil Rights Division has filed more than 45 legal enforcement actions in 25 states since 2009 to limit or shut down state care. On a website listing all the litigation it has filed, the DOJ includes the heading “Olmstead: Community Integration for Everyone.”
It’s not true, though, that Olmstead requires community-based care for everyone. The Supreme Court decision established a right to community-based housing and care only when:
1. The state’s treatment professionals have determined that community placement is appropriate,
2. Transfer is not opposed by the affected individual, and
3. The placement can be reasonably accommodated, taking into account the resources available to the state and the needs of others with mental disabilities.
Despite those clear conditions, the DOJ has plowed ahead with its community-integration lawsuits under the explicit assumption that all institutional care should be ended and everyone should be sent into community-based care, whether they want to go or not.
This viewpoint by the DOJ is a misinterpretation of the Olmstead decision, and it has had tragic consequences, according to the VOR. The organization pointed out in its testimony that higher mortality rates have been documented in Virginia, Nebraska, Tennessee, and Georgia in the wake of the DOJ’s deinstitutionalization settlements.
Those problems have occurred because so many of the privatized group homes to which the people formerly in the state facilities have been transferred are poorly monitored and are afflicted by high turnover and poor training of staff. Yet, that reality does not appear to have been recognized by the DOJ.
In Virginia, a state sued by the DOJ to close its state-run developmental centers, the risk of mortality for those individuals who left those centers was double that of those who stayed.
In Tennessee, DOJ lawsuits resulted in the closure of one developmental center in 2010 and the downsizing of two others. In that state, deaths among people released from institutions nearly doubled between 2009 and 2013. In addition, according to The Tennessean, a 2013 State Comptroller’s audit reported a lack of access to adequate medical and dental care, incarcerations, and hundreds of reports of abuse, and neglect and exploitation among the transferred developmental center residents.
In Nebraska, a 2014 monitoring team report found that of 47 persons considered to be “medically fragile,” who were transferred from a developmental center in 2009 as a result of a DOJ settlement, 20 (or 43 percent of them) subsequently died.
In Georgia, a 2010 a DOJ settlement agreement required the closure of all state-operated developmental centers and the transfer of 1,000 persons with developmental disabilities as well as 9,000 persons with mental illness from facility-based care. In March, The Augusta Chronicle reported that of 499 individuals with profound developmental disabilities, who had been transferred from the state developmental centers under the DOJ settlement, 62 (or 12%) died unexpectedly.
The Augusta Chronicle article discussed the case of Christen Shermaine Hope Gordon, a 12-year-old girl who died in community-care after being transferred from the Central State Hospital in Milledgeville, GA. The article recounted a litany of poor decisions and poor care that appear to have led to Christen’s death.
In a letter to the DOJ in January of this year, Margaret Huss, president of Intellectual Disabilities Advocates of Nebraska, urged the DOJ to ask critical questions about the mortality figures and other data regarding the transfer to community-based care prior to filing further lawsuits to close state facilities. “An increased risk of death should not be the unintended consequences of the worthy goal of community integration,” Huss’s letter stated. As of May 1, the DOJ had not responded to her letter.
That an increased risk of abuse, neglect, and death exists in community-based care has long been recognized, but few policy makers or people elected to office have been willing to stem the tide of deinstitutionalization. In March 2013, U.S. Senator Chris Murphy of Connecticut did call for an investigation of abuse and neglect in privatized group homes around the country, in response to a series by The Hartford Courant detailing those problems in that state.
In a letter to the Office of the Inspector General in the U.S. Department of Health and Human Services, Murphy termed the level of abuse and neglect in group homes “alarming.” Murphy asked the IG “to focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.”
But more than two years after Murphy’s request, it is not clear that the HHS Inspector General ever did undertake such an investigation. The IG’s office has so far not released a report and did not respond to an email query from us on April 30, seeking information on whether an investigation has been undertaken and what its status might be.
Senator Murphy’s office also did not respond to repeated inquiries from us last week as to whether Murphy ever received a response from the IG to his call for an investigation or whether he ever followed up with the IG after his original request in 2013.
Unfortunately, lawmakers in the U.S. Senate, in particular, have also not been supportive of VOR’s proposed legislative language to require the DOJ to consult with families before filing further lawsuits against state care. While language was inserted in a House appropriations bill for the DOJ last year at VOR’s request that protections for institutional care be considered by the DOJ as appropriate for those who desire it, that language was later watered down.
We can only hope that folks begin to wake up in Washington and elsewhere to overwhelming evidence that deinstitutionalization accompanied by privatization is not working, and that someone finally steps forward to slow both of those trends.
Compensation of provider executives in MA reaches $100 million
More than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation, according to our updated survey of the providers’ nonprofit federal tax forms.
By our calculations, state taxpayers are on the hook each year for up to $85 million of that total compensation.
We reviewed the federal tax forms for some 300 state-funded, corporate providers, most of which provide residential and day services to persons with developmental disabilities.
The following is a summary chart of our latest survey results (click on the chart to enlarge):

For the complete survey chart, click here.
We first released our survey about a year ago, when we found that more than 550 executives working for some 250 state-funded corporate providers of services to people with developmental disabilities in Massachusetts received a total of $80.5 million in annual compensation.
COFAR has also previously raised concerns that increasing amounts of money going to provider executives have not translated into higher pay for direct-care workers in Massachusetts.
The latest survey reports on 635 executives who received total annual compensation of $102.4 million and average annual compensation per employee of $161,231. The survey was based on provider tax forms filed in either the 2011 or 2012 tax years. Those tax forms are available online at www.guidestar.org.
The survey sample included 100 CEO’s and presidents, making an average of $210,227 in salaries and benefits; and 107 executive directors receiving an average of $130,835 in compensation. As the chart above shows, the survey also included 67 chief financial officers, 31 chief operating officers, 100 vice presidents, 110 directors, and 120 other officers, all earning, on average, over $100,000 a year.
A state regulation limits state payments to provider executives to $158,101, as of fiscal year 2013. Money earned by executives above the state cap is supposed to come from sources other than state funds.
Based on this regulation, we calculated that provider executives are eligible for up to $85 million a year in state funding to cover those total salary and benefits costs. Our calculation was based on identifying the companies paying executives at or above the state threshold of $158,101, and assuming that amount as the maximum state payment for each of those companies’ executives.
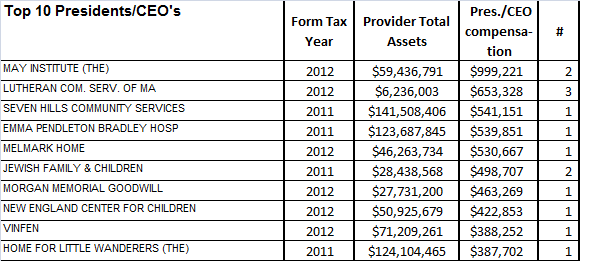
Among the top-paying providers in our latest survey was the May Institute, which paid two employees a total of $999,221 in the 2012 tax year. Both employees were listed as president and CEO of the provider. The May Institute’s federal tax form shows that one of the two employees, Walter Christian, worked for the company until December 2012 and received a total of $725,674 in salary and benefits in that tax year, which started on July 1, 2012. Christian was replaced as president and CEO by Lauren Solotar, who received a total of $273,547 in that same tax year, which ended on June 30, 2013.
Despite the regulation capping compensation payments by the state, the state auditor reported in May 2013 that the state had improperly reimbursed the May Institute, a corporate provider to the Department of Developmental Services, for hundreds of thousands of dollars paid to company executives in excess of that cap. COFAR had previously reported in 2011 that the state may have paid Christian and other executives of the May Institute more than the state’s regulatory limit on individual executive salaries.
The following charts show the top earning presidents/CEO’s and executive directors in our latest survey and the number of those executives holding each title in each company:

Most of the providers surveyed are under contract to the Department of Developmental Services, which manages or provides services to people with intellectual disabilities who are over the age of 22. The providers operate group homes and provide day programs, transportation and other services to tens of thousands of intellectually disabled persons in the DDS system.
As we have noted, the state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue.
Funding to DDS corporate residential providers rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in fiscal 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
More financial information about nonprofit corporate providers, including compensation of executives, can be found at www.guidestar.org.
Why the Fernald land deal should include a plan for the developmentally disabled
The history of what is now known as the Fernald Developmental Center hasn’t been free of some serious blemishes or controversy. But from 1889 to the present time, Fernald’s 200-acre campus in Waltham has been the site of a facility providing residential care for persons with intellectual disabilities.
That’s all about to change permanently.
Under legislation negotiated among representatives of the Patrick administration, the City of Waltham, and local legislators, the state will sell the campus to the city for $3.7 million, which comes to 18,500 per acre — a price that has been described as “dirt cheap.” It appears there is also a requirement that the city pay the state up to half the proceeds from the re-sale of any of that land to developers.
There is just one group of people that seems to have been left out of the plans and negotiations. That group is the developmentally disabled — the very persons who had been living at Fernald all along. Other than keeping the therapeutic swimming pool open at Fernald and maintaining a 29-bed nursing home on the campus, there appear to be no plans to continue to provide care or services at the Fernald site for persons with disabilities who live in the surrounding community.
This is an unfortunate oversight, not only for the residents who have been forced to leave Fernald, but for developmentally disabled people in the community. As I’ll explain, the lack of a plan for integrated, community-based care at the Fernald site has been, and will continue to be, both a missed opportunity to help those waiting for services and a potential waste of taxpayer money.
First, I would note that the Fernald Working Group, a coalition of local organizations, had recommended that a portion of the campus remain the site of residential care and services for the intellectually disabled. Similar proposals have been made over the years by the former Fernald League and COFAR. Both of those latter groups suggested a “postage-stamp” arrangement under which existing residents would live in housing situated in a small area of the campus while the rest of the campus was converted to other uses. And Waltham Mayor Jeannette McCarthy, the chair of a Fernald Reuse Committee, also publicly supported the continued use of part of the campus for institutional, residential and health care.
But the then Romney and subsequent Patrick administrations were interested only in one thing — closing Fernald and three other developmental centers in the state, contending the state would save tens of millions of dollars a year in doing so. They never considered any of the proposed alternatives to the closures, and have never done what administrations in other states have done, which is to propose the integration of congregate care facilities for the developmentally disabled with their surrounding communities.
The result is that since 2008, two of six remaining developmental centers in Massachusetts have been closed; a third center is being converted to state-run group homes, and just two residents of the Fernald Center remain on the campus out of a total of 160 who were there at that time. Most of the residents living in the four facilities targeted for closure were dispersed around the state, with the majority going either to state-operated group homes or to the Wrentham Developmental Center. Why has all of this been a missed opportunity and a potential waste of taxpayer money?
First, with regard to the cost to taxpayers, the administration projected that Fernald would be closed by July 2010, but the closure was blocked for four years by administrative and court appeals filed by guardians on behalf of some 20 remaining residents there. The administration elected to keep Fernald open only for the remaining residents there, pending resolution of their administrative and court appeals. This turned out to be an extremely inefficient way to proceed.
Not only has there been an undisclosed cost to the state in fighting the legal battle to close Fernald over the past decade, but as the population dwindled in all four targeted facilities, the cost per resident of care there shot up due to fixed costs such as heating and other utilities in larger buildings. This was particularly true for Fernald, which has remained open for more than four years with 20 or fewer residents.
The administration could have saved millions of dollars a year since 2010 had it been willing to consider and negotiate an alternative to outright closures of the facilities. The legal battle over Fernald would have ended immediately, and instead of continuing to house the remaining residents in several locations on campus, the state could have built small, cost-efficient housing in one location for the residents. That proposed alternative to closure has rarely if ever been reported on by the media, which has instead adopted the position of the administration and its corporate providers that the high cost of continuing to operate Fernald has been solely the fault of the residents remaining there.
Moreover, dozens of the Former Fernald residents were sent, as noted, to the Wrentham Center, which amounted to transferring residents from one developmental center to another. Not only was there no real savings in doing this, but the administration was forced to undertake renovations at Wrentham in order to accommodate the former Fernald residents — a project that cost taxpayers at least $3.2 million.
There is a second, and potentially greater, cost to taxpayers in closing Fernald and the other developmental centers without planning for any continuation of care at those sites that could be integrated with their surrounding communities. As we have noted, an undisclosed number of developmentally disabled people throughout the state have been unable to access services or care from DDS due to a lack of resources. The state has tried to address this problem by expanding the provider-run residential system, which has involved building more than 150 group homes spread around the state since 2008 and substantially increasing rates paid to the providers.
But there is no centralized system of care in the provider-run system. People have to be transported to day programs and for medical and other types of care — a process that is potentially much more expensive than if all of this care were available in centralized locations. Continuing to provide centralized care at developmental center sites could both allow more people in the surrounding community to receive services and provide those services more cost-effectively than is the case in a system consisting almost entirely of disbursed group homes.
We have also pointed out the potentially high cost of privatized care in Massachusetts and elsewhere due to the thick layer of highly paid corporate executives in that system.
That there isn’t necessarily a long-term savings in transferring people from developmental centers to decentralized, provider-based care has been acknowledged even by one of the leading proponents of deinstitutionalization in the Obama administration. I’ve blogged about a law journal article written by Samuel Bagenstos, a former top litigator in the Justice Department’s Civil Rights Division, in which Bagenstos stated that any cost savings in closing developmental centers “will shrink as people in the community receive more services.” He added that a significant part of the cost difference between institutional and provider-based care “reflects differences in the wages paid to workers in institutional and community settings — differences…that states will face increasing pressures to narrow.”
All of this is why we supported the vision of the Fernald Working Group, which described “a progressive site at Fernald where open space and greenways can be matched with an equal vision of integration for individuals with disabilities.” That vision encompassed both existing residents and disabled persons in the surrounding community. The Working Group specified that this vision included new housing and the preservation of the therapeutic pool and gym at Fernald as well as the chapel and programs for physical therapy, dental and medical services. As the vision statement noted, “all of these services could become part of the community and economic life of the Fernald redevelopment.”
But as far as we can tell, the Working Group’s vision has not been adopted by either the administration or the Legislature. While the newly signed legislation to sell the Fernald land to the city provides incentives for adopting “smart growth principles” and affordable housing in the development of the site, it makes no mention of continued services or care for persons with developmental disabilities.
Last week, I emailed Senator Michael Barrett and Representatives Tom Stanley and John Lawn, the key sponsors of the land sale legislation, to ask whether the continued use of a portion of the Fernald campus for individuals with disabilities was considered in the negotiations over the bill and whether any provisions for that might be made in the future.
A staffer in Barrett’s office said that no proposals to serve the developmentally disabled at Fernald were made at a public hearing on the land sale bill that was held in July by the Legislature’s State Administration Committee, and the idea was therefore not considered. But while the Village at Fernald concept for the disabled may not have been raised at a public hearing earlier this summer, most, if not all, of the negotiating parties to the legislation have long been aware of that concept. It should have been a part of the legislation from the beginning.
Does the administration have a double standard in the care of the disabled?
As The Boston Globe reported last week, Governor Patrick has “unveiled an ambitious and potentially costly plan” to reform the way the state’s criminal justice system handles mentally ill people.
The governor has proposed both a major increase in staff at Bridgewater State Hospital and a new facility there where potentially violent patients could receive care, according to the Globe.
We support the administration’s commitment to expanding care at Bridgewater State. But we wonder whether this is yet more evidence of what appears to be a double standard on the part of the administration with regard to care of the mentally ill versus persons with developmental disabilities.
The administration appears to believe that congregate settings are necessary and appropriate for the mentally ill, but not appropriate for the developmentally disabled. In fact, we think Governor Patrick will be known as a builder of major institutional facilities for the mentally ill, yet as a closer of facilities for the developmentally disabled. This appears to us to reflect the absence of a comprehensive plan by this administration for care of all disabled people in the commonwealth.
Why are we building new state facilities and expanding state-run care for one group, yet tearing facilities down, eliminating an intensive care model, and privatizing most services for another group?
In addition to the plans for expansion of Bridgewater State for the mentally ill, the administration has taken major credit for the construction of the new Worcester Recovery Center and Hospital. That facility, which opened in August 2012 at a cost of $302 million, has 320 beds for persons with mental illness. The administration has billed it as “the largest non-transportation construction project (the state has) undertaken in more than 50 years.”
The administration has also apparently realized that intensive treatment models are necessary for the mentally ill. According to the Globe, the administration has declared that mentally ill people “should receive the appropriate care in the appropriate setting.” The Bridgewater proposal includes a plan for spending $10 million for an additional 130 full-time mental health clinicians at the complex. Patrick administration officials told the paper that if the Legislature approves this funding promptly, the additional staff could be working at Bridgewater by September.
The Bridgewater proposal further calls for $500,000 to study the possibility of retrofitting an existing state facility such as Taunton State Hospital or building yet another a new facility to treat and evaluate potentially violent people accused of committing crimes, according to the Globe. The plan gives no cost estimate for the new facility.
At the same time, the administration is closing or has closed four of six developmental centers for people with profound levels of intellectual disability and severe medical conditions, contending these centers are too institutional. Developmental centers provide an intensive level of care that must meet federal Intermediate Care Facility (ICF) standards. ICF rules specify more staffing and monitoring than do federal and state requirements for privatized, community-based care in group homes.
Even sheltered workshops are considered by the administration to be too institutional for the intellectually disabled, and the administration has announced plans to shut those down by June of next year. The administration is, at the same time, pouring additional funding into privatized group homes for the intellectually disabled, scattered in communities throughout the state.
The argument could be made that the administration views institutional care as appropriate for people with mental illness who are violent, and that’s why it is expanding facilities such as Bridgewater State. But that doesn’t explain the construction of the Worcester hospital center; and it doesn’t explain why the administration is eliminating the ICF care model at facilities for the developmentally disabled such as the Templeton Developmental Center, where many people with behavioral problems live.
The alleged assault by a Templeton resident that caused the death last year of Dennis Perry shows that even that facility may not be fully equipped to meet the needs of all the people who live there, and keep them safe. And yet, the administration is closing Templeton as an ICF and converting the facility to group homes, which will only reduce the level of staffing and supervision there. Also, the attempted rape of a woman by a resident of a group home in Chelmsford in 2011 shows that there are intellectually disabled persons with potentially violent impulses who live in the DDS community system.
It has been argued that another difference between facilities for the mentally ill, such as the Worcester hospital center, and developmental centers for the developmentally disabled is that the Worcester facility is meant to help people make a transition to independent living in the community, whereas developmental centers are not intended to do so. Therefore, according to this argument, the developmental centers should be closed, and the remaining system will be devoted either to serving all disabled people in the community or helping them get there.
Our response to that argument is that we have consistently stated that residents of developmental centers who want to benefit, or can benefit from community-based care should be encouraged to do so. As far as we know, there has never been any rule or policy that prevented anyone who wanted to leave a developmental center from doing so and moving into the community system.
As we argued in connection with the Chelmsford group home incident, the real issue is the care model. The administration wants to eliminate the intensive, ICF care model for people with developmental disabilities. The administration does acknowledge that people with mental illness should receive the appropriate care in the appropriate setting. And they appear to understand that the community system is not the appropriate setting for all mentally ill people. But for some reason, the administration hasn’t yet figured out that the community system isn’t the appropriate setting for all people with intellectual and developmental disabilities either.
We do believe that one day, the state will come to realize that institutional care for a certain segment of the developmentally disabled is needed, and there will be an effort to reconstruct our institutional facilities for them. Unfortunately, we’re making that future job much more difficult and expensive by tearing down the system that we have had in place and which we spent so much money to upgrade from the 1970’s onward.
State-funded provider execs paid more than $80m a year
More than 550 executives working for some 250 state-funded corporate providers of services to people with developmental disabilities in Massachusetts received a total of $80.5 million in annual compensation as of Fiscal Year 2012, based on nonprofit federal tax reports surveyed by COFAR.
The average compensation among all 559 executives surveyed was $143,969 per year. Among CEOs, the average compensation was $185,809, while executive directors were paid an average of $127,164 in salary and benefits.
According to the COFAR survey, provider executives making over $100,000 a year on average included 97 executive directors, 92 CEOs, 71 chief financial officers, 31 chief operating officers, and 83 vice presidents. CEOs or presidents of 14 providers made over $300,000 each.
“I think few people realize what the real cost of privatized care is in Massachusetts,” COFAR President Thomas Frain said. “Do Massachusetts taxpayers really need to be paying hundreds of corporate executives millions of dollars for grossly duplicative duties? This makes no sense at all.”
COFAR has long been critical of efforts by the Patrick administration and the Romney administration before it to outsource residential and other services to providers without adequate oversight of the growing privatized system. The system appears to have become top-heavy with corporate executives who do not provide direct-care services, but who nevertheless draw large salary and benefits packages.
Most of the providers surveyed are under contract to the Department of Developmental Services, which manages or provides services to people with intellectual disabilities who are over the age of 22. Frain noted that DDS pays more than $1 billion a year in contracts to service providers, which operate group homes and provide day programs, transportation and other services to tens of thousands of intellectually disabled persons in the DDS system.
State regulations capped state payments to provider executives at approximately $149,000, as of Fiscal Year 2011. The average compensation among the surveyed executives was slightly less than that amount. Money earned by executives above the state cap is supposed to come from sources other than state funds.
But while the state cap on executive salaries is intended to limit the total amount of state funds going into the pockets of provider executives, COFAR has reported that the state may not receive complete information on the total compensation paid to provider executives and may not have the capacity to oversee their finances adequately. Also, COFAR has raised concerns that increasing amounts of money going to provider executives has not translated into higher pay for direct-care workers in Massachusetts.
The state auditor reported last year that in one case involving the May Institute, a DDS provider, hundreds of thousands of dollars in state funds had been paid to company executives in excess of the regulatory cap. COFAR’s executive compensation survey found that the May Institute CEO received $404,900 in compensation in FY 2011 and that a total of 12 company executives were paid a total of $2.5 million that year.
At $404,900, the May Institute CEO was the fifth highest paid CEO on COFAR’s list. Community Systems, Inc. topped the COFAR list of the highest paid CEOs, with two employees listed on the company’s federal tax filing as serving as company CEOs in FY 2011 and drawing combined compensation of $526,755. Second on the list was Morgan Memorial Goodwill, whose CEO was listed as making $464,572 in FY 2012.
Community Systems federal tax filing states that the company, which is based in Forestdale, MA, took in $14.4 million in revenues in Fiscal Year 2011. Of that amount, the company received $11.6 million from DDS, according to a 2011 financial report filed with the state’s Operational Services Division.
(The Community Systems OSD report lists only compensation in FY 2011 for two executive directors and does not list the company CEOs. As a result, OSD appears to have disallowed only $21,000 in funding to the company as having been earned above the regulatory compensation cap. This appears to confirm COFAR’s finding that the OSD receives incomplete information from providers on executive compensation.)
In addition to the CEOs listed on the Community Systems federal tax report, two employees were listed as executive directors of the company that year and made a combined total of $276,538. The OSD report lists the two executive directors of the company as having made only $154,473.
The following chart, based on COFAR’s survey of some 250 providers, shows 30 of the providers with the top earning CEOs (click on it to enlarge).

Where’s the beef in Community First?
We’ve long maintained that the Patrick administration’s agenda of phasing down and closing state developmental centers would ultimately fail to free up additional funding for the community based system.
It’s been nearly three years since the administration announced its plan to close the Fernald, Templeton, Monson, and Glavin Centers and reportedly plow back as much as $45 million a year in the “savings” into beefing up the largely privatized community-based system of care. That $45 million savings projection was a cornerstone of the administration’s “Community First” initiative.
So far, the administration has succeeded in moving hundreds of residents out of developmental centers, starting with Fernald, which is now emptied of all but 14 of its residents, who have filed appeals of their transfers. But nothing remotely close to the $45 million in savings has materialized. In fact, the opposite has been the case — the administration has continued to cut community-based line items in the Department of Developmental Services budget.
In a November 20 email to members and other advocates, the Association of Developmental Disabilities Providers, which has wholeheartedly supported the closures of the developmental centers, stated the following :
For the last four fiscal years, in order to cope with the effects of the economic collapse of 2008, the Commonwealth’s budget has:
- deeply cut Family Support programs, leaving 10,000 families without service,
- inadequately addressed Chapter 257 rate reform by not introducing sufficient funding to rate making but instead forcing existing programs to redistribute already inadequate funding
- failed to address historically low salary needs of the community workforce (though the Legislature has recently added the first salary reserve dollars in four years)
- continued to require community programs to implement state mandates without sufficient funding, including closing sheltered workshops without funding to replace this model in favor of a more inclusive and empowering model.
- not backed it’s professed interest in Community First and Employment First with funding to make these efforts successful. (my emphasis)
Not exactly a ringing endorsement of the success of the administration’s community-based care delivery model and its promised use of of the savings from the developmental center closures. We hope the ADDP and the Arc of Massachusetts will reach the next logical step in their argument and urge the administration to cease and desist from closing the centers.
Unfortunately, the ADDP and the Arc of Massachusetts are supporting H.984, known as “The Real Lives Bill,” which appears to continue to rely on the premise that DDS clients should not be given the choice of living in developmental centers.
The bill, sponsored by Rep. Tom Sannicandro, is intended to provide for more choice for persons with intellectual disabilities. But it appears to specifically deny consumers the choice of “congregate services.” In other words, everyone should have a choice, as long as they choose only small, community-based settings. We believe, however, that the congregate services provided by developmental centers are appropriate for certain people who are unable to benefit from community based care. And now we’re seeing that closing the congregate care centers is not freeing up community-based funding.
Sannicandro’s bill does appear to recognize that the community-based system has not thus far benefitted from the developmental center phase-downs. The bill’s text reads:
Too many people are not receiving the assistance they need. The public Medicaid system is reeling from cost pressures. The time has come for individuals with disabilities, families, advocates and providers to work together with policy makers in the administration and legislature in crafting a support system that both increases quality and on average reduces costs whenever possible.
We agree with the language in Sannicandro’s bill on that last point. We just disagree that closing the developmental centers is the right way to go about it.
Update on our requests for cost records
After a month and a half, it’s troubling that the Patrick administration is apparently still unable to locate cost records we requested pertaining to a single community-based group home contract.
I just received a letter from the Department of Developmental Services, dated September 14, that they are in the process of searching for the documents, which I had requested on July 29. Meanwhile, the MassHealth Privacy Office in the Executive Office of Health and Human Services has been searching for these same records since August 9.
To recap, we’ve been trying to find out the sources of state funding for medical, nursing, clinical, and therapeutic services in a single DDS group home program run by the May Institute, a private provider. We have a copy of a $1.2 million contract with the May Institute, which provides for 24-hour residential services under the program for 14 individuals in four residences in the DDS Central Middlesex Area.
The FY 2009 contract, however, only provides for direct care and limited nursing services for the 14 residents. It does not mention medical, extended nursing, clinical or therapeutic services.
From what we’ve been able to determine, the administration has been basing its $20 million annual cost savings estimate in closing the Templeton, Monson, and Glavin Developmental Centers on a comparison of their budgets with the cost of community-based group contracts such as the May Institute contract. But here’s the rub. Our understanding is that the Templeton, Monson, and Glavin budgets do provide for medical, extended nursing, clinical, and therapeutic services.
Naturally, the community system will appear to be less expensive than the developmental centers if certain community-based costs are not taken into account. That’s why we want to find out exactly how much is being paid to fund those additional services to which the May Institute residents are reportedly entitled, and where that money is coming from.
By the way, we originally asked DDS on July 7 for the budgets of the Monson, Templeton, and Glavin Centers. A month later, we received a one-page document from the department with single, line-item amounts representing the total annual spending for each facility. There was no budgetary breakdown whatsoever for the facilities.
We appealed to the state’s Public Records Division for help, explaining that a budget of a state facility involves more than just a single line item. As a result, I received a second letter from DDS, also dated September 14, stating that the department was in the process of searching for the “additional (budgetary breakdown) information” I had requested.
I guess DDS considers a budget and a “budgetary breakdown” to be entirely separate concepts. Stay tuned.
Once again, we’re waiting for the administration’s cost records
It has been more than a month since we asked Secretary of Health and Human Services JudyAnn Bigby for public records detailing the costs of specified services in a particular group home program for intellectually disabled persons in Massachusetts.
It has been almost two months since we asked Commissioner of Developmental Services Elin Howe for the budgets of the Templeton, Monson, and Glavin developmental centers.
To date, we’ve received neither set of records.
As we’ve previously noted here, we’ve been attempting to compare the cost of an apparently typical vendor-run group home program with the three developmental centers. We wanted to see whether the Patrick administration was comparing apples to apples in claiming to the Legislature in the last two fiscal years that closing the Templeton, Monson, and Glavin centers will save tens of millions in state funds.
As we reported, a group home contract, which we did receive last May from DDS, specified a yearly cost per resident of $104,400. In its cost savings analysis, the administration compared a very similar residential cost based on group home contracts with an average calculated cost of care at Templeton, Monson, and Glavin.
The potential problem with the administration’s analysis that we found in examining the single group home contract was that it specified budgeted costs for only direct-care, supervisory, and minimal nursing staff. What about the extensive nursing, medical, clinical, and therapeutic staffing that exists at the developmental centers and to which the residents of DDS group homes are entitled?
The fact that those additional medical, clinical, and therapeutic costs were not in the group home contract we examined appeared to raise the question whether the administration’s savings analysis was accurate. One immediate question was: if those additional costs are not paid through DDS contracts, how are they paid? Secondly, what is the total amount of those community-based costs that the administration may have missed in its analysis?
Once we get the answers to those questions, we can determine for ourselves whether there would be a savings or not in closing the developmental centers.
On July 29, we sent Public Records requests to both Secretary Bigby and Commissioner Howe, asking for copies of any documents detailing funding for medical, nursing, clinical, and therapeutic services for individuals residing in the community-based group home program we had selected for review. About three weeks prior to that, we had asked DDS for the Templeton, Monson, and Glavin budgets for the same time periods as the group home contract.
On August 9, I received a letter from the records custodian at EOHHS, stating that the agency was in the process of identifying the records we had requested regarding the group home contract. Last week, I called the records custodian, and was told EOHHS was still working on our request. He wasn’t able to tell me when the records would be found.
We’ve appealed to the Public Records Division for the Templeton, Monson, and Glavin budget documents. We’re close to filing an appeal for the group home contract records.
But one piece of useful information may have emerged here. The fact that the August 9 response to our request came from EOHHS and not from DDS does appear to confirm that it is not DDS, but some other source at EOHHS, that funds medical, clinical, and therapeutic services in the DDS vendor-run group home system. We believe that other source of funding is MassHealth.
In any event, it’s getting clearer and clearer that the administration wasn’t counting all the community-based costs of care it incurs when it told the Legislature there would be major savings in closing the developmental centers.
Identifying the missing costs
The Patrick administration claims that the average per-person cost of Department of Developmental Services vendor-run group homes is less than the average per-person cost of state developmental centers for persons with intellectual disabilities.
But we’ve now identified some specific missing group home costs that we think the administration overlooked in its analysis.
An apparently typical DDS vendor contract, which we have reviewed, did not specify any psychological or therapeutic services, and only specified minimal nursing services. Developmental center budgets, on the other hand, do provide for all of those services.
This appears to be the first major confirmation we’ve been able to obtain, after months of Public Records Law requests from DDS, that the Patrick administration’s savings claims in closing four developmental centers in Massachusetts are based on an apples-to-oranges comparison. The administration has not fully responded to our follow-up questions about these costs.
I asked DDS Commissioner Elin Howe on June 16, after we had first reviewed the $1.2 million contract, whether medical, clincal, and therapeutic services were available to the residents of the program, and, if so, how those services were funded.
The email I received in response from DDS General Counsel Marianne Meacham, dated July 2, stated the following:
With regard to your questions regarding clinical services available to individuals in the particular…program site, as you know, a full array of clinical services (medical, physical therapy, speech therapy, occupational therapy, psychological, etc.) are available to the individuals in the program through community providers as needed and set forth in the individual’s individual support plan.
This carefully worded answer states only that medical, clinical, and therapeutic services “are available to individuals in the program,” but it doesn’t say how those services are funded — in other words, where the money comes from. Here’s why that is a key question:
In July 2010, the adminstration provided a cost analysis to the Legislature, which claimed a $20 million annual savings in closing the Templeton, Monson, and Glavin Developmental Centers and transferring most of their residents to vendor and state-operated group homes. In the cost analysis, the administration specified a “community residential” cost per client of $107,689. After adding an average “day services” (work and daily living skills programs) rate to that cost and an average transportation rate, the administration computed a total “community services cost” of $140,955 per client.
The administration then compared that $140,955 total community cost to an average per-person cost at the Templeton, Monson, and Glavin centers of $233,902. The administration’s conclusion was that serving a client in the community was $92,947 less expensive than in a developmental center.
After we asked DDS, starting last December, for all documents supporting its community residential cost figure, DDS provided, among other things, a spreadsheet listing total costs of close to 1,000 vendor contracts in FY 2009. We selected one of those contracts for closer review and asked DDS for a copy of it.
The Fiscal Year 2009 vendor contract with the May Institute, Inc. specified 24-hour staffing in a program serving 14 individuals. The contract further stipulated a rate per client of $286 per day, or $104,400 per year. This was quite close to the $107,689 community residential rate in the administration’s analysis.
However, as noted, the $104,400 community residential cost did not include clinical, therapeutic, or full medical costs of care available to community-based residents. The budgets of the Templeton, Monson, and Glavin centers do provide for those services.
On July 6, I emailed back to Meacham at DDS, asking once again how the medical, physical therapy, speech therapy, occupational therapy, psychological, etc. services available to residents of the May Institute program were funded for the residents of the May Institute program. To date, I’ve received no reply to my question.
This is why we need an independent study of the cost of closing the Templeton, Monson, and Glavin Centers.
Nonprofit vendor salaries drawing increased attention
Organizations such as the Massachusetts Providers Council may still be defensive about suggestions that scrutiny be applied to the sometimes excessive salaries drawn by executives of human service providers in Massachusetts and elsewhere.
But it’s becoming clear in the wake of the fallout over the recent $4.2 million severance package for a Blue Cross Blue Shield CEO and a number of other similar cases, that even in the nonprofit community, responsible voices are beginning to be raised urging serious consideration of the appropriateness of executive pay levels.
Here’s Ruth McCambridge, editor in chief of the influential Nonprofit Quarterly, discussing in an email to subscribers the Blue Cross severance package to former CEO Clive Killingsworth:
This case is a poster child for why the public does not trust our considerations of pay levels. While most of us are, of course, well within or below reasonable limits for pay, there are these high fliers among us, and in this case the money that Killingsworth walked away with came very directly from millions of families’ pockets, some of whom are legitimately concerned about such stuff as getting by from day to day.
Meanwhile, in an interview with the Nonprofit Quarterly last week, Paul Light of the Wagner School of Public Service at New York University, had this to say:
I think the nonprofit sector has an obligation to get the very best talent it can at the most reasonable cost appropriate to its role in the public service—more broadly defined. Yet you can’t simply say, “We’ve got to pay whatever the market demands, and that’s the only criteria we can use.”…
I don’t think you have to take that vow of poverty, but at the same time I wonder if the sector is obligated to set itself out there as being more a part of the community that it serves—obligated by basic issues of fairness to set reasonable market-sensitive pay, but also stay in touch with the world we serve.
Here in Massachusetts, State Senator Mark Montigny of New Bedford came closer this year than ever before in gaining passage of proposed legislation that would limit pay for both nonprofit executives and board members to $500,000 (a pretty generous threshold in our view, particularly for board members). Versons of Montigny’s measure passed the House and Senate in the form of budget amendments last month, but the measure was ultimately knocked out of the budget conference committee. However, the measure is still alive in the form of a bill before the Judiciary Committee, but has not yet been scheduled for a hearing.
Montigny’s bill is supported by Attorney General Martha Coakley, who has been investigating compensation of nonprofit board members, and found that several health insurers were paying tens of thousands of dollars to their trustees annually. Coakley’s spokesman, Brad Puffer, told The Globe last month that Coakley and her staff are concerned about situations in which “board members of any charity (nonprofit) are paid.”
Massachusetts already limits the amount of state funds that can be earmarked to pay for nonprofit salaries to $143,900. COFAR has reported that in a number of cases, state and federal records regarding salaries subject to that compensation limit don’t match each other.
Meanwhile, Coakley, along with Massachusetts State Auditor Suzanne Bump and Inspector General Gregory Sullivan have been investigating questionable financial practices, including high executive salaries, of nonprofit organizations involved in the state’s special education program. COFAR has called on Bump and Sullivan to expand their probe to examine the entire human services vendor system for persons with intellectual disabilities.
In sum, this is an issue that isn’t going away soon and can’t be ignored. Salaries and financial practices of human service vendors, insurers and other nonprofit organizations should be a major focus of state oversight. The other major focus should be on quality of care and services. To the extent that there are problems or a lack of state oversight in one of these two areas, we believe there are likely to be problems in the other.
