Archive
Volunteer advocates meet with state senators’ staffs in start of effort to preserve Wrentham and Hogan centers
The fight to preserve the Wrentham and Hogan care centers in Massachusetts began this past Friday with a visit to the State House of a dozen advocates and family members of persons with intellectual and developmental disabilities.
Our group, which included several COFAR members, held meetings with legislative aides to State Senators Paul Feeney and Rebecca Rausch. Rausch’s district includes the Wrentham Developmental Center.
Jim Durkin, legislative director for AFSCME Council 93, a state-employee union in Boston, spoke to us prior to the Friday meetings, noting that AFSCME is currently deeply involved in fighting to save the Pappas Rehabilitation Hospital.
“AFSCME is fully behind your efforts to preserve Wrentham and Hogan, which are vital to the fabric of care in this state,” Durkin said. “Right now, we are fighting the battle for the Pappas Hospital, but we will be working with you to make sure that the ICFs are protected as well.”
The Healey administration’s move to close Pappas and allow Wrentham and Hogan to die by attrition are all part of the same effort to eliminate state-run care under what we have long argued is a faulty assumption that it will save the state money.
The first meeting we had on Friday was with Shane Correale, legislative director for Senator Feeney. We have asked Feeney to draft legislation that would open the doors at Wrentham and Hogan to new admissions and establish housing on the campuses of the facilities for elderly family members of the residents.

Wrentham and Hogan advocates at the State House — (Left to right) Mitchell Sikora (COFAR Board member), Marsha Hunt, Shiri Ronen-Attia, Laurie Noland, Ilene Tanzman, Ana Paula Meehan, Allan Tanzman, Mary Dias, Elaine Strug, Jim Durkin (AFSCME Council 93), and Kim Meehan. (Photo by David Kassel)
During that meeting, COFAR member Irene Tanzman stressed the importance of Intermediate Care Facility (ICF) settings, such as Wrentham and Hogan, which meet federal standards that are stricter than the state standards for group homes. “Not everyone thrives in the community,” Tanzman said, adding that the state is “denying us the opportunity” for ICF-level care.
“We want choice,” Tanzman added. “The community is a legal fiction. People coming in get nothing. They get so-called self-directed services with inadequate or no budgets.”
Kim Meehan, a COFAR member, talked about her successful effort last year to gain admission to Hogan for her legally blind and quadriplegic sister Kristen. But Kristen’s admission came only after a lengthy battle that included blog posts by COFAR in support, and coverage by Fox 25 news.
“There was no place for Kristen to go,” Kim said, explaining the situation her sister was facing while being kept for two months at Faulkner Hospital. “DDS kept using the verbiage that the community would be the ‘least restrictive’ setting for her. It didn’t matter to DDS that her doctor said she needed an ICF.”
Mitch Sikora, a COFAR Board member, recounted the landmark Ricci v. Okin litigation in the 1970s and 1980s that led to major improvements in state-run facilities that serve people with intellectual disabilities. Many aging people with intellectual disabilities, he noted, are in particular need ICF-level care because facilities such as Wrentham and Hogan are equipped and staffed to serve people with complex medical needs.
Sikora also discussed the comprehensive care his brother Stephen has received at Wrentham.
Both Shiri Ronen-Attia and Marsha Hunt pointed out that their sons are nonverbal, don’t socialize, and have no interest in group activities — characteristics that make them different from most people with developmental disabilities who are suitable candidates for community-based settings. “Group homes can’t meet their needs,” Ronen-Attia said. “They have no voice.”
Hunt said that her son “sits day after day with nothing to do.” He is not provided in his group home with the occupational, physical, or speech therapy that might enable him to make progress in those areas, she said.
As I noted, many group homes have become the new warehouses in which intellectually disabled people are now largely placed.
We also discussed the proposed legislation that Senator Feeney has agreed to draft. As Irene noted, the legislation was proposed some five months ago.
Correale said Feeney’s staff was still working on our legislative proposals, and was “trying to bring them to the Senate as an institution.” He said Feeney’s office has begun discussing the legislation with the co-chairs of the Children, Families, and Persons with Disabilities Committee.
COFAR has specifically asked Feeney’s office to draft language to be added to the ICF line item in the state budget, stating that persons who qualify for community-based care from DDS have a right to ICF care.
In sum, Friday’s meetings convinced us that if state-run ICF care is to be preserved in Massachusetts, advocacy efforts must continue, and should be combined, if possible, with the ongoing effort to save the Pappas Hospital. We recognize that this will be an uphill battle.
But the good news is that we got what seemed to be a sympathetic hearing on Friday from the staff members of the two legislators. What is needed going forward is for the lawmakers themselves to attend the advocacy sessions, and to publicly support the preservation of state-run care.
Our priorities for the 2025-2026 legislative session
The 2025-2026 session of the Massachusetts Legislature began on January 1 of this year. So we are taking this opportunity to announce our priorities for this 194th legislative session.
Admissions should be opened to the ICFs and state-operated group homes
We are seeking the filing and passage of legislation that would require the Department of Developmental Services (DDS) to offer the Wrentham Developmental Center, the Hogan Regional Center and state-operated group homes as options for persons with intellectual and developmental disabilities (I/DD) who are seeking residential placements in Massachusetts.
Unless the administration agrees to open those facilities to new admissions, they will eventually close. DDS data show the number of residents or the census at both the Wrentham Developmental Center and Hogan Regional Center continued to drop from Fiscal Years 2019 through 2024.
The census at Wrentham dropped from 323 in Fiscal 2015 to 159 in Fiscal 2024 – a 50% drop. The census at Hogan dropped from 159 in Fiscal 2011 to 88 in Fiscal 2024 – a 45% drop.

Source: DDS
From Fiscal 2008 to 2021, the census in the state-run group home system dropped from 1,059 to 1,023 – a 3.4% decrease.
Meanwhile, the census in the state’s much larger network of privatized group homes continued to climb during that same period, rising from 6,677 to 8,290 — a 24% increase.
Currently, the privatized group home system in Massachusetts is providing substandard care even as thousands of individuals continue to wait for residential placements.
Even the Arc of Massachusetts, which has pushed for the closures of all remaining ICFs, has acknowledged a “systemic failure” in the largely privatized DDS system in which thousands of persons with I/DD are unable to get services.
State-run residential facilities, which have better trained and higher paid staff, are vital to the fabric of care in the DDS system. As Olmstead v. L.C., the landmark 1999 U.S. Supreme Court decision, recognized, there is a segment of the population with I/DD that cannot benefit from and does not desire community-based care. ICFs, in particular, must meet stringent federal standards for care that make them uniquely appropriate settings for persons with the most profound levels of disability and medical issues.
Yet, DDS does not inform individuals and families seeking residential placements that these state-run facilities even exist. During the past two years, we have reported on two admissions to ICFs in Massachusetts (here and here), but those admissions have been the exceptions. In at least two instances in the past two years, families have been unsuccessful in efforts to win placements for their loved ones at the Wrentham Center.
That policy decision by DDS to discourage or block new admissions guarantees that the number of residents in state-run residential care will continue to drop, and that the ICFs, in particular, will eventually be closed.
Right to ICF care
Despite DDS’s policy, the federal Medicaid law and its regulations confer a right to ICF care to individuals and their families and guardians.
As Medicaid.gov, the federal government’s official Medicaid website, explains, “States may not limit access to ICF/IID service, or make it subject to waiting lists, as they may for Home and Community Based Services (HCBS)” (our emphasis).
Open ICF campuses to family housing
In addition to our proposal for legislation to open the ICFs to new admissions, we are calling for legislation that would establish housing on the Wrentham and Hogan campuses for elderly family members of the residents of the facilities.
Such housing would allow families to live in proximity to their loved ones in DDS care and to establish caring communities. It would provide peace of mind to ageing parents and siblings who may find it increasingly difficult to make long trips to visit their loved ones in the facilities.
Adequate funding needed for state-run facilities in the Fiscal Year 2026 budget
In order to preserve ICFs and state-operated group homes, state funding for these settings must be adequate. We are calling for the following increases in the state budget for the coming fiscal year:
- DDS ICF line item (5930-1000). Based on the federal Bureau of Labor Statistics inflation rate of 3.1% in the Boston Metropolitan Area as of November 2024, we are requesting a $3.9 million increase in this line item, from $124,809,632 in the current fiscal year, to $128,678,731 in Fiscal Year 2026.
The ICF line item decreased by 40% between Fiscal 2012 and 2025 when adjusted for inflation.*
- DDS state-operated group home line item (5920-2010). We are requesting a $10.3 million increase in this line item, from $330,698,351 to $340,950,000 in Fiscal 2026.
The state-operated group home line item increased by 47.6% between Fiscal 2012 and 2025 when adjusted for inflation. However, that compares with an increase during that period of 65% in the corporate-provider residential line item (5920-2000). The corporate community-residential line item was $1.7 billion in Fiscal 2025.
ICF budget language should be changed
We are seeking two modifications to the language that is included every year in the ICF line item in the state budget (5930-1000). In one instance, the language mistakenly implies that the U.S. Supreme Court ordered the closures of institutions for persons with developmental disabilities.
In the second instance, the annual budget language lists three conditions for discharging clients from ICFs to the community, but leaves out one of the key conditions in Olmstead, which is that the client or their guardian does not oppose the discharge. We will request that that condition be added to the language in the line item.
Regarding the first instance, the budget language refers to Olmstead v. L.C., the Supreme Court’s landmark 1999 decision, which considered a petition by two residents of an institution in Georgia to be moved to community-based care.
The budget language states that DDS must report yearly to the House and Senate Ways and Means Committees on “all efforts to comply with …Olmstead…and… the steps taken to consolidate or close an ICF…” (our emphasis)
However, as noted above, closing institutions was not the intent of the Olmstead decision. The decision explicitly states that federal law — specifically the Americans with Disabilities Act (ADA) — does not require deinstitutionalization for those who don’t desire it.
We believe the annual state budget language should be changed to state: “…the steps taken to consolidate or close an ICF and the steps taken to inform families of the choices available for residential care including ICF care.”
We are concerned that the current line item language could allow the administration to justify continuing to underfund the line item, and possibly to seek the eventual closures of the Wrentham and Hogan Centers.
Regarding the second instance in which we are seeking a language change, the three conditions listed in the annual state budget for discharging clients to the community are:
- The client is deemed clinically suited for a more integrated setting;
- Community residential service capacity and resources available are sufficient to provide each client with an equal or improved level of service; and
- The cost to the commonwealth of serving the client in the community is less than or equal to the cost of serving the client in an ICF/IID…”
The first two of those conditions do match conditions listed in the Olmstead decision for allowing the discharge of clients to the community. However, there is a further condition in Olmstead, which is that such a discharge is “not opposed” by the client or their guardian. That condition is not included in the budget language, and we will request that it be included.
Choice needed in residential services
DDS holds considerable authority regarding residential placements. Families cannot change residential providers without DDS approval. We would support legislation creating a voucher system, which would allow family choice, create competition, and improve the quality of care. This would also help families who need to move to other parts of the state for work or family reasons.
Guardianship reform needed
Reform is needed of the guardianship system in probate court, which traps many families into losing disputes with DDS.
We would support a guardianship reform bill that would provide for free legal representation for family members and that would presume that parents or siblings would be suitable guardians in petitioning for guardianships.
We have long supported proposed legislation that would presume that parents, in particular, would be suitable guardians of their adult children with I/DD. This legislation was first proposed by the late Stan McDonald, who had sought unsuccessfully to regain guardianship of his intellectually disabled son.
Stan’s bill, which was most recently filed in the previous legislative session, has never gotten out of the Judiciary Committee, however.
Independent DDS appeals process
The appeals process that persons must follow regarding Individual Support Plans (ISPs) contains a serious conflict of interest in that DDS controls the entire process.
When a family member or guardian of a DDS client appeals the client’s ISP, the DDS commissioner appoints a hearing officer of its choice to decide the case. After the hearing officer decides the appeal, the commissioner can reverse the decision. We have reported on at least two instances in the past year and a half in which this appeals process has been marred by apparent bias on the part of the DDS-selected hearing officer against the appellants.
We would support a bill, which would place the entire ISP appeals process under the control of the independent state Division of Administrative Law Appeals (DALA).
DPPC Abuser Registry reform
Last year, we reported that in only a minority of the cases in which the Disabled Persons Protection Commission (DPPC) affirmed initial substantiations of abuse allegations against care providers did the agency conclude that those persons’ names should be placed in the DPPC’s Abuser Registry.
An individual whose name is listed in the Registry can no longer work in any DDS-funded care setting.
Following our report, state Senator Patrick O’Connor, the original sponsor of the legislation that created the Registry, said he was worried by our findings and that it “may be time to fine-tune” the law.
We are calling for changes in the law that include requiring the DPPC to consider several factors listed in the regulations for determining whether a care provider against whom abuse has been substantiated is really fit to continue to provide services. Right now, the regulations say only that the DPPC “may” consider factors such as previous incidents of abuse and the provider’s previous work history.
Also, we believe the regulations should explicitly require that the DPPC place care providers in the Registry in all cases in which the agency has affirmed allegations of intentional physical or sexual abuse.
Funding to corporate providers must result in higher wages for direct-care workers
Increases in state funding to the providers over the past decade have resulted in continuing increases in the pay of the provider executives. The increased state funding, however, hasn’t been passed through by the providers to their direct care employees.
We are calling for legislation that would raise the pay of direct-care workers employed by DDS corporate providers to $25 per hour.
Work opportunities needed in congregate care settings
In the wake of the closures of all sheltered workshop programs in Massachusetts as of 2016, we are calling for legislation authorizing the introduction of work opportunities for individuals in community-based day programs.
The last time such legislation was proposed appears to have been in 2019 in the form of then H.88. That legislation, however, did not make it out of committee.
Safeguards and corrections needed in Supported Decision Making legislation
During the last legislative session, identical Supported Decision Making (SDM) bills came close to final enactment, but the bills died in the House Rules and House Ways and Means Committees respectively at the end of the session. We had raised numerous concerns about the bills with those and a number of other legislative committees.
We expect the same SDM legislation will be refiled in the current session. We intend to raise similar objections to the bills unless they are redrafted to correct serious flaws.
SDM reflects a growing movement to restrict guardianships of persons with I/DD and replace those guardians with “networks” of more informal advisors. While SDM can hold promise for some high-functioning individuals, and we would support its adoption only with adequate safeguards, particularly safeguards against the potential marginalization of family members.
*From the Massachusetts Budget & Policy Center’s online Budge Browser at https://massbudget.org/budget-browser/.
An overlooked but vitally important book on the history of institutional care in Massachusetts
Among the books that anyone interested in the continuum of care for persons with intellectual and developmental disabilities (I/DD) should not miss is Ingrid Grenon’s meticulously researched “From One Century to the Next: A history of Wrentham State School and the Institutional Model in Massachusetts.”
I hope the controversial Special Commission on State Institutions, which is due to release a report on the history of institutional care in Massachusetts next June, has a copy of this book. While the book can be purchased online, it is also available in libraries.
I have to confess to having missed this book, which was published in 2015, until Grenon contacted me a few weeks ago. Having now read it, I realize it makes a powerful case that institutions, in themselves, are neither good nor bad. It is how they are run that counts, just as is the case in any care setting.

As this book documents, the high point of the care and services at Wrentham — prior to the advent of the modern Intermediate Care Facility (ICF) model in the 1980s — was during the 1920s.
The 1920s, exactly a century ago, was a period when the then Wrentham State School, under the direction of its first superintendent, George Wallace, had a caring staff and administration, and offered a multitude of services and activities for the residents. Wallace displayed a genuine interest in helping them lead meaningful and productive lives.
But, as the book shows, Wrentham, like other similar institutions that sprang up in this state and around the country, entered a long decline, starting in the 1930s as it became more and more overcrowded and understaffed. By 1960, Wrentham, which was intended to house no more than 1,500 residents, had a residential population of 2,400. Today, less than 160 residents remain there.
Wrentham and other state schools in Massachusetts were finally brought back to excellence as a result of the Ricci v. Okin class action litigation in the 1970s and the intervention of the late U.S. District Court Judge Joseph L. Tauro.
A refutation of the ideology behind deinstitutionalization
Based on that historical arc, I think the book offers a compelling refutation of the longstanding and dominant ideology used to support deinstitutionalization. That ideology is based on the premise that all institutional care is bad and outdated, and that that characteristic never changes and can never change.
The book, however, shows, on a year-by-year basis, how one institution – Wrentham — progressed from very good to very bad, and back again. Wrentham did change, and it changed dramatically. It is clear that if an institution is well run and has sufficient resources, it can be a positive and even necessary option for residential care.
Grenon’s book also shows how the ongoing debate over institutional versus community-based care was central to the thinking even of Walter Fernald and Wallace way back in the late 19th and early 20th centuries.
What was later to become the Fernald Developmental Center was established in 1848 as the first institution in the United States for persons with intellectual and developmental disabilities. It was later named for Walter Fernald, who became its first superintendent. The then Wrentham State School was officially opened in 1910.
Grenon’s book demonstrates that it’s not a simple proposition that the Fernald and Wrentham schools were meant to be segregated facilities, intended to keep people with intellectual disabilities out of the view of the general public. Even for Walter Fernald and George Wallace, there were two ways of looking at their facilities.
The centers could be seen from the perspective of the now discredited science of eugenics, as places to separate people with I//DD from the general population. Or they could be seen, as Wallace viewed them and Fernald later came to view them, as places where people with I/DD could be helped to lead meaningful and fulfilling lives. Unfortunately, the prevailing view today is that that former perspective regarding institutions is the only valid one.
Bellotti and Dukakis changed the game
Grenon documents Wrentham’s history virtually year by year from the early 1900s until 1993 when Judge Tauro officially disengaged from the Ricci litigation. It includes many photos from throughout that period.
In addition to consulting numerous primary sources, Grenon interviewed many key figures in the history of Wrentham and of institutional care in Massachusetts. Among those were former Governor Michael Dukakis and his then Attorney General Francis Bellotti.
Bellotti, who died yesterday (December 17) at the age of 101, took the unusual and courageous step in response to the Ricci lawsuit of refusing to defend the conditions at Wrentham, Fernald, Belchertown and the other state schools in the 1970s.
As Grenon explains, Bellotti’s refusal as attorney general to defend the administration – a position that Dukakis fully supported – meant the state would cooperate with the plaintiffs in the case. Those plaintiffs included Ben Ricci, who had brought the original lawsuit on behalf of his son, who was a resident of the then Belchertown State School.
Founding of COFAR
Grenon also interviewed John Sullivan, one of the founders of COFAR, whose daughter, Colleen Lutkevich, continues to work with this organization.
Sullivan, who died in 2017, told Grenon in 2012 that he had helped start COFAR in 1984 as a counter to the Massachusetts Arc and to Rhode Island Senator John Chaffee, both of whom were pushing to close all of the state schools and transfer all of the residents to privately run, community-based group homes.
Sullivan and other like-minded advocates, including Ricci, Charles Hart, Richard Krant, and Louise Johnson, believed that the improvements brought about by the Ricci litigation had transformed Wrentham and the other state schools into the best possible settings for their loved ones by the mid-1980s.
Personal experiences
But Grenon’s book is based on more than historical research and even interviews. She also recounts her own experiences at Wrentham, having worked there for 34 years in a variety of capacities, starting in 1981. Her personal descriptions draw the reader into the day-to-day life and drama of the institution during her time, and add to the context and richness of the center’s history.
Grenon started working at Wrentham after graduating from college with a degree in psychology. Her first job was as a direct care worker, a position referred to at the time as a “Mental Retardation Assistant.” She spent most of the next four years with the “heavy hitters” — women in the D Building who were given that appellation because they had behavioral problems.
In 1982, Grenon was promoted to ward supervisor, and then became building manager, and later back-up shift supervisor and crisis responder.
In 1985, because of her separate degree in equestrian science, she became director of a new therapeutic horseback riding program at Wrentham. And from 1992 until 2014, she served as a coordinator in public relations at Wrentham and as a community liaison.
In 2016, Grenon discussed her book and emerging therapies and models of care for people with I/DD in a series of interviews, including this one.
Opposition from DDS
But as Grenon explained to me, the Department of Developmental Services (DDS) was not happy with her book. She said that when top DDS administrators learned she was writing it, they wanted her to emphasize only “the most egregious” aspects of Wrentham’s history.
The reason for DDS’s position is clear. Since the 1990s, a succession of administrations in Massachusetts has been intent on shutting down state-run residential care and privatizing the services. But Grenon told the Department officials she wanted to tell the whole history of Wrentham, both good and bad.
The result, she said, was that she was repeatedly threatened by DDS with termination in the last few years of her employment, and was later even banned from visiting the campus.
Grenon said that at a meeting with the DDS administrators in 2013, “They all wanted to know why I wanted to present the facility in a positive light, and I told them something like, ‘up until now, everything that has ever been written about facilities has been very negative. I’ve found some surprising evidence to the contrary and I want to present it. I don’t just want to regurgitate egregious conditions, I want to present facts.’”
Grenon said, though, that the reply from one of the administrators at the meeting was, “’We would really rather that you present the egregious conditions. . .’” She said she was also told “not to make the facility look good.”
As we’ve argued before, it is vitally important to study the history of the care of persons with I/DD in Massachusetts and elsewhere, if only to avoid repeating the mistakes of the past. It is just as important to recount the entire history, and, as Grenon said, to present the facts.
It is only in recounting the full and complete history of any person, event, trend or institution that valid conclusions can be drawn as to the meaning of the past and how to plan for the future. That is what Grenon sought to do in writing her book; and, in our view, she fully succeeded.
Legally blind and quadriplegic woman ‘thriving’ at Hogan Center
After initially being denied a placement at the Wrentham Developmental Center, Kristen Robinson has been living and “thriving” since June at the Hogan Regional Center, her sister, Kim Meehan, said last week.
Kim said the family is now ready to talk about the happy outcome of their months-long struggle to get Kristen, who is 51 years old, into an Intermediate Care Facility (ICF) in Massachusetts.
“She (Kristen) is so happy,” Kim said. “ She’s joyful, cared for, loved. They love her at Hogan. She’s treated the way she should be treated.”
Hogan, which is in Danvers, and the Wrentham Developmental Center are the state’s two remaining ICF-level congregate care centers. But as we’ve noted many times, it is extremely difficult for people to get admitted to them.

Kristen and Kim on wheelchair swing at Hogan Center
As we reported in May, then Department of Developmental Services (DDS) Commissioner Jane Ryder initially promised Kristen’s family she would admit Kristen for evaluation and rehabilitation to Wrentham’s May Center medical unit.
But Ryder reneged on that promise just a few days later, saying she hadn’t been aware that only Wrentham Center residents are admitted to the May Center unit. This was despite the fact that Kristen is profoundly intellectually disabled, legally blind, and quadriplegic, and has seizure disorder and severe dysphagia, a medical condition that causes an inability to swallow.
DDS rarely admits individuals to either ICF because the Department maintains that so-called community-based residential settings are less “restrictive.” But DDS had been unable to find either a community-based group home or a nursing home that could meet Kristen’s needs.
Yet, while Ryder did go back her promise to admit Kristen to Wrentham, Kim said Ryder then gave the family some other options. One option was for an “evaluation” of Kristen at Hogan; and the other options were for short-term placements at either of two private rehab facilities or a state-operated group home.
Kim said the family visited all of those settings and selected Hogan even though it is a three-hour round trip from Kim’s home in Norfolk. “We felt she would be safe there,” she said.
Kristen was admitted to Hogan on June 17. It is not clear whether the placement is considered by DDS to be permanent, but Kim said she and Karen are prepared to fight to ensure that she remains there.
Hogan offers full range of services and activities
Kim maintained that all of Kristen’s needs are being met at Hogan, particularly her need for 24/7 nursing care.
Prior to her placement at Hogan, Kristen had been confined for weeks at Faulkner Hospital in Boston following a choking incident in her mother’s home.
Kristen had lived her entire life under her mother’s care in Walpole. But when their mother died a year ago this month, Kim and her sister, Karen Brady, and their husbands began to take turns caring for Kristen and staying overnight with her.

Given Kristen’s medical complexities – particularly those related to swallowing and choking – it is safest for her to be at a facility like Hogan where medical care is available on site, Kim said. At Hogan, Kristen doesn’t need to be taken off campus for medical care or for her day program.
Kim said Kristen has been receiving physical and occupational therapy at Hogan, and is attended by doctors, nurse practitioners, and many other care givers. She is also regularly taken outside for recreational activities, including the use of a swing set built for people in wheelchairs. And she attends arts and crafts, music nights, communal dinners, and enjoys visits from school bands.
Kim said she is looking forward to having Kristen attend Hogan’s greenhouse this winter to work on making wreaths. “She always enjoyed planting flowers with our mother,” she said.
“Normally, at age 22, the educational system falls off,” Kim noted. “Here they work with her daily. This is a community like no other. When we looked at the group homes DDS showed us, people were just sitting around watching TV.”
Cleanliness highlighted
Kim said she would also like to “highlight the cleanliness at Hogan. You could eat off the floors there.” Kristen is also very clean now, she said. When she was at the hospital, the staff were not able to shower her, she said.
Kristen’s potential still being assessed
Kim said that since she has been at Hogan, Kristen “is doing things we never knew she could do, and they’re still in the early stages of determining her capacity.”
For instance, physical therapists are working with her on standing up. “She hasn’t stood up since she was a little kid. She is now feeding herself with assistance,” Kim said.
Kim added that clinicians at Hogan think Kristen may be able to understand more than her family had previously thought. Early on, they found that Kristen could identify six colors. “She was never able to do that before.”
The Hogan clinicians also think Kristen may be able to communicate with a communication board. “They’re doing assessments to see what she can comprehend. They are learning things about her that we didn’t know. It could take years to find out what’s going on in her mind,” Kim said.
Similar assessment from mother of man admitted to Wrentham in 2022
Kim’s assessment of Hogan is similar to Janice Marinella’s assessment of the Wrentham Center. Janice’s son Jeremy was admitted to Wrentham in 2022 after years of poor care in the community-based system.
Janice told us at that time that, “I no longer see it (Wrentham) as institutional. I now see the love and devotion the staff gives my son.” She added that even though the buildings are old, her son’s unit is “immaculate.”
It is unfortunate that the Healey administration continues to subscribe to a long-held ideology that care in Massachusetts’ two remaining congregate-care centers is unduly restrictive, and that better and more appropriate care can be found in the community-based and largely privatized group home system.
The evidence clearly shows this ideology is wrong. It doesn’t matter how many people are served by a care setting as long as the ratio of staff to residents is adequate and the staff are caring, well trained, and motivated. The testimony of Kim Meehan, Janice Marinella, and others we have spoken with over the years shows that is certainly the case at the Wrentham and Hogan Centers.
Is RFK Jr. open to reversing the longtime federal policy of phasing out state-run and ICF care?
Late last month, we sent a message to Robert F. Kennedy Jr. via his Make America Healthy Again (MAHA) website, asking whether he would support the preservation of state-run, congregate and group home care for persons with intellectual and developmental disabilities (I/DD).
RFK, who has been nominated by President-elect Donald Trump to head the U.S. Department of Health and Human Services (HHS), has spoken out about what he refers to as the capture of governmental agencies and regulators by the pharmaceutical, agricultural and other industries. He has cited the undue influence of corporate interests in healthcare, in particular.
While there are many people who are skeptical of Kennedy, primarily due to his controversial statements about COVID and other vaccines, our main concerns center around the future of residential care for people with I/DD. Would Kennedy’s efforts to rein in corporate interests in healthcare include reining in corporate providers that contract with states to run group homes for people with I/DD?
In our message to Kennedy, we asked whether he would be “committed to changing the direction in which HHS and the U.S. Department of Justice (DoJ) have long been headed in furthering the runaway privatization of human services and the closures of state-run services for people with I/DD, including Intermediate Care Facilities (ICFs).”
We understand that there are many people competing for Kennedy’s attention right now, and that it might be some time before we hear back. We hope we do hear back.
Privatization proponents acknowledge problems, but oppose the use of institutional resources
As we noted in our message to Kennedy, the privatized system of care in Massachusetts and elsewhere in the nation for people with I/DD is broken.
In Massachusetts, the state Department of Developmental Services (DDS) is funding the privatized group home system at close to $1.7 billion in the current fiscal year — an increase of more than 60% from a decade previously. Yet, thousands of people are waiting for residential placements in group homes that are rife with abuse and neglect and underpay their direct-care staff. The executives who run those corporate providers make exorbitant salaries.
Massachusetts has just two remaining state-run ICFs, which serve as a critical backstop for residential care, and meet strict federal standards for staffing and treatment. They are the Wrentham Developmental Center and the Hogan Regional Center. Yet a succession of administrations has let these facilities die slowly by attrition, and has steadily increased funding to corporate group-home providers.
Also being phased out in this state is a smaller network of state-run group homes, which provide care from well-trained staff. Families and guardians seeking residential placements for their loved ones with I/DD are not informed of these state-run options, and, when they do seek those placements, are routinely denied.
Federal government has pushed for ICF closures
As we noted to Kennedy, this same anti-congregate care trend has long been encouraged at the federal level. The federal Centers for Medicaid and Medicare Services (CMS) and the Civil Rights Division of the DoJ have pursued a relentless policy for years of deinstitutionalization and privatization of services. This policy has been promoted under the guise of civil rights, with the misleading argument that congregate care segregates people with I/DD.
Not only has the DoJ filed unnecessary and unwanted lawsuits around the country to close ICFs, but the federal government has encouraged the closures of important and highly successful programs such as sheltered workshops for people with I/DD. This has been done under the mistaken ideology that all people, no matter how severe their disabilities, can compete and succeed in the community-based system.
However, the U.S. Supreme Court in Olmstead v. L.C. recognized that institutional care is valid and appropriate for those who desire it and who can’t cope in the community.
Yet the single-minded focus of the federal government and other proponents of privatization on eliminating institutional care has caused the proponents to ignore the serious problems with community-based care.
Biden administration increased funding for community-based care, but not state-run ICFs
Over the past four years, the Biden administration increased Medicaid funding to states for home and community-based services. But as COFAR and a key state employee union, AFSCME Council 93, noted in a joint letter to Massachusetts Senator Elizabeth Warren in 2021, the Biden administration was not similarly proposing any additional funding for state-run ICFs.
Many advocates for the disabled are worried today that the incoming Trump administration will reverse the Medicaid gains that the home and community-based system has received under the Biden administration. They are particularly concerned that under the leadership of Kennedy and Mehmet Oz, who has been nominated to head the CMS, Medicaid funding to the states will be replaced by block grants, and individual recipients will be subject to work work requirements.
While we understand these concerns, we would also note that pumping more Medicaid dollars into a flawed, privatized system won’t solve the problems that continue to plague that system.
As we stated in our message to Kennedy, we believe that the states need to reopen the doors of their state-run ICFs and group homes before it is too late. If we lose these critical residential options, we foresee a race to the bottom in the quality of care for thousands of our most vulnerable residents.
However, the Healey administration in Massachusetts, like several before it, takes its cue from the federal government, and is pushing us ever closer to the demise of state-run and ICF-level care.
DDS hearing officer’s denials of appeals for placements at Wrentham Center appear to show bias against families and guardians
It’s becoming clear that the legal division and even the internal appeals division of the Department of Developmental Services (DDS) have a bias against families and guardians seeking residential placements for their loved ones at state-run congregate care centers in Massachusetts.
A decision by a DDS hearing officer last summer marks at least the second time in the course of a year that the Department shot down appeals by families to transfer intellectually disabled persons from corporate, provider-run group homes to the Wrentham Developmental Center.
Concerns downplayed
In both cases, the same DDS hearing officer, William O’Connell, denied the appeals in rulings that used the same language in many instances. And O’Connell appeared to downplay or even ignore concerns raised by the families about a lack of adequate care and meaningful activities in the “community-based” group homes and day programs.
In his decisions, O’Connell stated either that he did not give “substantial weight” to testimony of the families, or that they had not provided “substantial and probative evidence” that their adult children were receiving inadequate services or that Wrentham had more services and less turnover among staff. At the same time, he found to be “credible” every argument raised against the families by DDS in its closing briefs.
In particular, O’Connell didn’t explain why he didn’t give substantial weight to what is arguably easily verifiable and true assessments about the Wrentham Center regarding services and staff turnover. This is clearly due to the fact that O’Connell fully subscribes to the administration’s ideology that all congregate residential care is institutional and therefore bad.
Also, as explained below, O’Connell’s decisions appear to be internally contradictory with regard to whether clients in the DDS system have a right to placements at the Wrentham Center and the Hogan Regional Center in Danvers, which are known as Intermediate Care Facilities for individuals with intellectual disabilities (ICFs).
As we previously reported, O’Connell denied an appeal in July 2023 filed by a father and mother who had been trying to get their son into the Wrentham Center. Last summer, O’Connell denied a second appeal by another mother to gain admission to Wrentham for her son. Then DDS Commissioner Jane Ryder upheld both of O’Connell’s decisions.
We have frequently noted that both ICFs are critical backstops for care in the DDS system. Yet these facilities are being targeted for eventual closure by the administration. Families and guardians of persons needing residential placements are not informed that the two ICFs exist; and, if they do ask for placements there, are almost always denied.
Conclusion stated at outset of decisions
The DDS bias was evident at the start of each of O’Connell’s decisions in which he stated that care in the community in each case had been “successful.”
In both cases, O’Connell stated that one of the “issues presented” was, “Does (the) appeal … entitle (the individual) to a change in residential placement, specifically admission to a specific ICF, after…years of successfully being supported in a less-restrictive community-based residence.” (my emphasis)
It appears from this language in both appeal decisions that O’Connell had already made up his mind before even hearing testimony. He listed, as an “issue presented” (meaning the case had yet to be heard), that the individual’s supports in the community had been successful.
However, in each case, the family had appealed based on an argument that the community-based supports had not been successful.
Also, a guardian in at least one of the cases claimed that her son was leading a highly restricted life in his community-based group home. And both families noted that they found that the Wrentham Center is highly interactive with its surrounding community, and offers many services and activities that are normally not available in their sons’ group homes.
So, the hearing officer’s presumption from the start in these cases that ICFs are automatically more restrictive than are community-based group homes indicates an unwillingness to consider evidence in individual cases that the opposite may be true.
Also, his presumption that care in the community-based system is uniformly successful ignores years of evidence that the community-based system has become highly dysfunctional and is rife with abuse and neglect.
Claims of inadequate services not given weight
As noted, O’Connell actually acknowledged that he didn’t give “substantial weight” to allegations by each family about a lack of specific activities or supports in the community-based system. Instead, he accepted DDS’s assertions that the individuals in each case were “well supported” or “successfully supported” in that system.
In fact, O’Connell used the exact same language in stating in each decision that:
I find credible (DDS’s) testimony that admission to (Wrentham) is not appropriate for (the individual) because there was no immediate risk to (the individual’s) health or safety and no indication that (the individual’s) needs cannot continue to be met in the community.”
O’Connell just updated the name from the first to the second decision.
In both decisions, O’Connell also stated that DDS was “continuing to work” or “willing to accommodate” some of the specific services and supports requested by the parents. But those promises, in the parents’ view, are vague and ultimately empty. If DDS were really committed to doing these things, they would have been done years ago, and the parents would not be appealing for placements at Wrentham.
Hearing officer’s decisions and DDS policy are internally contradictory regarding ICF admissions
In each decision, O’Connell accepted the DDS argument that the federal Medicaid law “does not entitle (the individual) admission to an Intermediate Care Facility at the Wrentham Center… “
O’Connell, as noted, also accepted DDS’s uniform position that each individual “is not entitled to admission because (Wrentham) is not the least restrictive environment available to serve (the individual.” And in each decision, O’Connell added that, “the Medicaid Act choice provision does not entitle (the individual) to choose between ICF or in a community home on an annual basis.”
But DDS, in fact, does offer such a “choice.” It’s just that DDS, not the Medicaid Act, insists the “choice” must always be a community-based home.
DDS requires families and guardians to sign a waiver of ICF care in order to receive DDS services. In what is referred to as a “Choice Statement” on the form, the applicant for DDS services is required to sign the following:
CHOICE STATEMENT:
I ____________________________________(Applicant or guardian) choose to apply for the Home and Community-Based Services Adult Waiver Programs and live and receive my services in the community rather than in an ICF/ID. (my emphasis)
DDS essentially admits here that a choice of ICF care exists in that the Department requires families and guardians to waive that choice in order to receive DDS services.
In fact, O’Connell explicitly stated in each appeal decision that the family applied for enrollment of their child “in the HCBS (Home and Community Based Services) Waiver …, exercising their choice for community rather than ICF services in so doing.” (my emphasis)
Despite that apparent choice, O’Connell stated in both decisions, as noted, that the individuals in question did not have a right under federal law to placement in an ICF. DDS, in fact, asserted in each case that:
DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.
This, in our view, appears to violate federal law, which does confer a right to institutional care for those who desire it. The U.S. Supreme Court, in Olmstead v. L.C., also held that a right to institutional care exists.
Not only does federal law specify that there people who are found to eligible for ICF-level care are entitled to choose it, but DDS and O’Connell both acknowledge that such a choice exists. It is not a real choice, though, if DDS requires families and guardians to waive their right to one of the available options.
It is moreover, disingenuous of DDS and the hearing officer to tie families and guardians forever to community-based care by falsely claiming that those persons had freely chosen it years before in many cases.
What is ultimately so frustrating about this situation is that DDS and the administration as a whole continue to cling to an ideological position against congregate care that ignores reality. They continue to maintain that ICF care is more restrictive than care in the community, no matter what evidence may be presented to the contrary.
And DDS and the administration continue to ignore evidence that community-based care is beset by serious problems. As a result, when families and guardians appeal the inevitable denials by DDS of a full continuum of choice in residential care, the official adjudication process they encounter is anything but fair and impartial.
A compelling new book chronicles a girl’s life at the Belchertown State School
Edward Orzechowski has done it again. He has written a second gripping, as-told-to account of life within the notorious and now long-closed Belchertown State School in western Massachusetts.
The launch of his new book, “Becoming Darlene,” is scheduled for November 23 at 1 p.m. at the Florence Civic Center in Florence, MA.
“Becoming Darlene” is about the life of Darlene Rameau, a former Belchertown resident, as related in a series of interviews with Orzechowski. It follows a similar pattern to that of Donald Vitkus, whose experience before, during, and after Belchertown, was the subject of Orzechowski’s first book, “You’ll like it Here.”

In each case, Orzechowski, a former COFAR Board member, has written the life story of a person who spent most of their childhood at the Belchertown school. When Donald was first sent there in the 1950s, and Darlene in the 1960s, that institution, like a number of others in Massachusetts, was a literal warehouse of abuse and neglect.
It is important to understand that the type of institution that Orzechowski describes in both of his books no longer exists today. Starting in the mid-1970s, while Darlene was still at Belchertown but Donald had long since left it, major upgrades in care and conditions began to be implemented at that and other similar institutions in Massachusetts. These changes were the result of a class action lawsuit first brought by Benjamin Ricci, the father of a former Belchertown resident.
The upgrades were overseen by U.S. District Court Judge Joseph L. Tauro. By the time Tauro disengaged from his oversight of the case in 1993, he wrote that the improvements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
As Orzechowski notes, Darlene became aware while she was still at Belchertown of the impact of Tauro’s involvement. Suddenly, and seemingly in one day, new, kinder staff appeared. Restrictions and beatings ended, Darlene says. But those changes still took many years to be fully implemented.
In 1996, Belchertown was closed for good. Today, only two large congregate care facilities remain in Massachusetts — the Wrentham Developmental Center and the Hogan Regional Center. Both centers must meet strict federal standards for care and staffing that were made possible by the federal litigation in Massachusetts and in other states starting in the 1970s.
At Belchertown, Darlene was a keen observer of nonstop human suffering, of wards filled with naked, neglected children, and reeking of urine and feces and infested with insects.
As was the case with Donald Vitkus’s story, much of the story about Darlene is about her attempts to cope in the “real world,” after having been discharged from Belchertown. For both Donald and Darlene, the transition was filled with trials and setbacks. Belchertown continued to affect both of their lives in sometimes tragic ways.
“Becoming Darlene” is a true story, but it reads like a novel. It is a page turner. It is at turns disturbing and heart breaking. But as with Orzechowski’s first book, one finishes this second book with a feeling of gratitude for Darlene and for the triumph of her spirit.
Federal IG report finds safety deficiencies at the Wrentham and Hogan Centers, but misses the big issue – What about the group homes?
A federal investigative agency has reported deficiencies in safety and emergency preparedness in Massachusetts’ two developmental centers for persons with intellectual and developmental disabilities.
The October 2024 report by the Inspector General with the U.S. Department of Health and Human Services alleged 44 deficiencies related to life safety and emergency preparedness at the Wrentham Developmental Center and the Hogan Regional Center.
The IG’s report, however, raises a number of questions, in our view. First, will the IG similarly examine safety policies in the much larger, corporate-run group home network in Massachusetts?
The number of privatized, yet state-funded group homes has grown exponentially as developmental centers, also known as Intermediate Care Facilities (ICFs), have been closed over the past decade.
Secondly, why did the IG not address the quality of care in the ICFs and the group homes? It is in the group home system today that the most serious problems of abuse and neglect are endemic.
Thirdly, why not investigate the lack of access to ICFs for people needing residential care, and the misguided efforts to close them?
Finally, how serious were the safety deficiencies at Wrentham and Hogan that the IG’s report identified? The report did not appear to provide sufficient detail to answer that question.
No discussion of seriousness of deficiencies
The IG report stated that as a result of the deficiencies, “the health and safety of residents, staff, and visitors at the two ICFs are at an increased risk of injury or death during a fire or other emergency.” The question is how much of an increased risk?
The deficiencies included such things as fire extinguishers that had not been inspected on a monthly basis; placement of oxygen cylinders in hazardous storage areas; exits in some buildings that were obstructed, sprinkler heads that were “blocked or obstructed” in some instances; portable space heaters that were improperly placed in residential areas; and holes in some ceilings and walls.
While some of those things sound potentially serious, a problem with the report was that it gave few if any details about them. For instance, what else was contained in the hazardous storage areas? How were the sprinkler heads blocked, and how many were blocked?
Strangely, the report never named either of the two Massachusetts ICFs, so it never specified which of the deficiencies were found in which of the two facilities.
The report noted that the portable fire extinguishers that had not been inspected monthly were found in one of the ICFs, although, as noted neither of the ICFs was named in the report. The report also didn’t say how many fire extinguishers in that facility had not been inspected, or how many months had gone by without inspections.
The report didn’t explain what it meant by blocked or obstructed sprinkler heads. In a photograph that was included in the report, it didn’t appear that the sprinkler in the photo was broken, but rather that the sprinkler had been installed in the ceiling of a closet, and that it was partially blocked by objects placed underneath it.
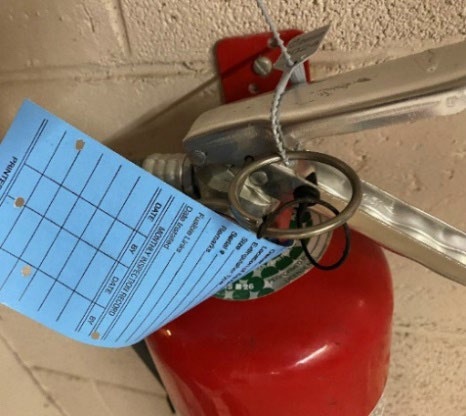
Fire extinguisher with the monthly inspection tag not filled out. From IG report.
Also, many of the deficiencies involved failures to provide documentation. It’s hard to judge the seriousness of some of those findings, particularly because some of them seemed ambiguous. For instance, the report stated that, “Both ICFs did not have a formal communications plan that was updated at least every 2 years.”
What is a “formal” plan versus an informal plan, and does this mean the facilities had no plan at all? There was no explanation or details provided about that.
The report also stated that “one ICF did not have policies and procedures that address the facility’s emergency preparedness plan and identified hazards within the facility’s risk assessment.”
What exactly does that mean? Did it mean that that particular ICF did have an emergency preparedness plan, but didn’t have “policies and procedures that address” the plan? Don’t plans refer to policies and procedures?
Robert Goldstein, commissioner of the Massachusetts Department of Health, which inspects the ICFs annually, responded to the IG report, stating that the majority of the audit findings were “immediately corrected” by the staff of each of the facilities.

Deficiency identified as “obstructed sprinkler head.” From IG report.
It’s also not clear to us why the federal IG singled out the Wrentham and Hogan Centers for this inspection report. We understand that the IG conducts investigations when it is requested to do so by an elected official. Who would have wanted such an investigation done just about the Wrentham and Hogan Centers, and why?
The report itself noted that there are approximately 5,400 Medicaid-certified ICFs in the U.S., and that Massachusetts has just two of them. Four others were closed in this state between 2012 and 2015.
The IG noted that its report on the Massachusetts ICFs is the first in a planned series of audits that will similarly assess compliance with federal “life safety, emergency preparedness, and infection control requirements for ICFs.” So, it does appear that the IG will be conducting similar searches for fire extinguishers without inspection tags and blocked exits in ICFs in other states.
Hopefully, those coming reports will provide more explanatory details about the deficiencies that will surely be found. It would also be nice if the IG were to expand the scope of its investigations to include the broader questions why ICFs around the country are being closed, and what the quality of care is in the group home systems.
We are not holding our breath in anticipation of those broader investigations.
DDS provides heavily redacted documents concerning one-time calculation of vacancies in state-operated group homes
The Department of Developmental Services has provided us with almost completely redacted documents concerning a calculation it made that there were approximately 91 vacancies in its state-operated group homes as of June of 2023.
That month in 2023 was apparently the one and only time that DDS ever attempted to determine the number of vacancies in the homes. The Department, however, is either unable or does not want to explain how or even why the vacancy rate was calculated on that one occasion.
In July of this year, we reported that DDS had finally clarified, after we had filed an appeal for records from the Department, that it doesn’t track the number of vacancies in its state-operated group home network.
However, in September 2023, the Department stated that it could, in fact, provide us with the number of vacancies as of that one date. The vacancies were within a network of group homes that then had close to 1,000 residents. (As of this past June, the total number of residents had dropped to 986.)
About two months later in 2023, DDS stated that the number of 91 vacancies was only “an approximation” that had been determined in a one-time “exercise” that DDS employees had participated in. Since then, “no similar exercises have been conducted,” a DDS attorney stated.
That explanation, however, only appeared to raise the question why DDS attempted on one occasion, but never again, to determine the number of vacancies in its group-home network.
Even though thousands of people with intellectual and developmental disabilities are waiting for residential placements and other services from DDS, why would the Department not have a continuing interest in knowing whether its state-run network has available beds for them?
Based on those questions, we filed a new Public Records Request with DDS on July 12 of this year, seeking all documents relating to the Department’s exercise, which had resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.
We hoped some of those documents might shed light on why the exercise had been conducted.
In a response on August 9, DDS provided records that it described as “documents that DDS employees relied upon to identify the approximate number of state-operated group home vacancies as of June 30, 2023.”
However, the documents appeared to provide no information regarding the nature or scope of the exercise or the reasons for conducting it.
One of the documents provided, labeled “Southeastern Residential Services — 6/15/23 — Temporary Moves,” was filled with text boxes containing information that had been entirely blacked out. There was no readable information in the document other than the words “Medical Respite” below one of the redacted text boxes. I’ve reproduced that document here:
DDS document provided to us concerning group home vacancy calculation
Another heavily redacted document, labeled “Metro Residential Services Caseload List July 2023,” appeared to contain only the names and positions of DDS employees.
Another document, referred to as ‘Central West Region Vacancy Tracker,’ appeared to be an undated spreadsheet with columns containing the names and phone numbers of DDS employees.
There were approximately 70 listings of the word “vacancy” in a separate column in the spreadsheet that appeared to contain the redacted names of residents of group homes in that region. There was no apparent summary information in that or any of the other documents.
In particular, there was no reference in any of the documents to the total of 91 vacancies that the exercise reportedly identified. None of the documents contained any identifiable connection to the exercise or the subject of the exercise — the number of vacancies in the group homes.
As a result, we appealed on August 26 to the state supervisor of public records, asking that DDS be ordered to clarify whether it did or did not possess records that specifically described the nature or scope of the one-time, vacancy-determination exercise.
On September 6, the supervisor of public records stated that in a phone call between a staff attorney of the Public Records Division and an attorney for DDS that same day, “the Department confirmed that it provided all records responsive to (our) request.”
The public records supervisor added that, “The Department further confirmed that the exercise in question was an informal exercise that provided an estimate for vacancies, and that the records provided to (COFAR) were used in determining the approximate numbers.”
The supervisor, in other words, was satisfied with the Department’s response. Because the exercise was “informal,” whatever that means, DDS was apparently not required to maintain or provide any documents that might shed any light on it. Our appeal was denied.
As we’ve said before, the fact that the administration does not even track the vacancy rate in state-operated group homes is evidence, in our view, that the administration does not view state-run residential services as a viable option for waiting clients. DDS, in fact, is letting the state-run system die by attrition.
In light of all of that, we think it would be helpful to know why the Department decided at one point a few years ago to conduct an informal exercise to determine the approximate vacancy rate as of one particular date.
Was it because a number of DDS officials have been telling families, as we have heard, that there are no vacancies in state-operated group homes, and the Department had no idea if that information was correct? If so, the exercise showed that there were, in fact, vacancies in the residences.
Unfortunately, it doesn’t appear that the fact that the exercise indicated the existence of an approximately 10 percent vacancy rate in the state-run homes has persuaded the Department to admit more people to those residences.
So why did DDS conduct that one-time exercise? It appears we may never know the answer to that question.
DDS finally acknowledges it doesn’t keep track of whether there are vacancies in state-operated group homes
For almost a year, we had been trying to clarify with the Department of Developmental Services (DDS) whether there are – and we suspect there are – continuing vacancies in the Department’s network of state-operated group homes.
Finally, in a clarification issued earlier this month in an appeal we filed with the state public records supervisor, a DDS attorney stated flatly that, “DDS does not track state-operated group home vacancies.”
While it’s helpful to know it would be a waste of time to continue to ask DDS for information it clearly says it doesn’t have, the Department’s clarification still raises a number of questions. First, why doesn’t DDS track what appears to be basic information about its state-operated group home network?
Secondly, even though thousands of people with intellectual and developmental disabilities are waiting for residential placements and other services from DDS, why would the Department not have any interest in knowing whether its state-run network has available beds for them?
One troubling answer to those questions is that the Healey administration does not view state-run residential services as a viable option for those thousands of waiting clients. This is borne out by evidence that DDS is letting the state-run system die by attrition.
DDS does not generally inform people seeking residential placements of the existence either of its network of state-run group homes or of its two remaining state-run congregate residential centers – the Wrentham Developmental Center and the Hogan Regional Center. Instead, the Department directs those people to its much larger network of state-funded group homes that are run by corporate providers.
In many cases, families have told us that when they have asked about placements in state-operated group homes, DDS has stated that there are no vacancies in such homes in their area. That is despite the now-apparent fact that DDS doesn’t actually know whether there are vacancies or not.
Ambiguous statements about information on vacancies
For close to a year, DDS provided ambiguous responses to requests we made under the Public Records Law for information on the number of vacancies in the state-operated group home network in recent years.
In September 2023, I first filed a Public Records request with DDS, asking for “the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.” I also asked for data on the census, or number of residents in the state-run group-home system, and the capacity, or total number of available beds in the system.
DDS responded that it did not have “any responsive records pertaining to the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.” However, the Department added in that same response that, “The Department can provide the number of vacancies in state-operated group homes as of June 30, 2023, which is 91.”
Given that the Department was both saying it didn’t have information on the number of vacancies each year, but did have that information with regard to a specific date, I appealed to the public records supervisor. The public records supervisor agreed that it was unclear whether DDS did or did not have information about those vacancies.
DDS then responded with a statement that only appeared to add to the confusion. The Department stated:
Vacancies are not tracked by the Department independently from the capacity and census data provided above. Vacancy numbers are more complicated as they are dependent on a number of real time factors, including but not limited to the temporary placement needs of individuals, staffing, and other group home demographics.
Finally, this past July 10, after I had requested information on the number of vacancies through April of this year, DDS issued the following clarification:
DDS does not have in its possession, custody, or control the state-operated group home vacancies on the specific dates requested because DDS does not track state-operated group home vacancies. (my emphasis)
One-time “exercise” to determine vacancy number
In its July 10 response, the Department also sought to explain how it had come up with the number of 91 vacancies as of June 30, 2023, despite not tracking vacancies.
DDS stated that prior to my original Public Records request in September 2023, “DDS employees participated in an exercise which resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.”
However, since then, “no similar exercises have been conducted,” the DDS response stated.
That explanation, however, only appears to raise further questions.
Why, for instance, did DDS attempt on one occasion, but never again, to determine the number of vacancies in its group-home network?
Based on questions like that, I filed a new Public Records Request with DDS on July 12, seeking all documents relating to the Department’s exercise, which resulted in identifying the approximate number of state-operated group home vacancies as of June 30, 2023.
DDS stated that it will provide a response to my request as of Friday of this week (August 2).
DDS data on census and capacity raise further questions about possible vacancies
Despite the lack of data about vacancies, the data DDS has provided about the census and capacity of the state-operated homes implies to us that vacancies do exist in the group-home network.
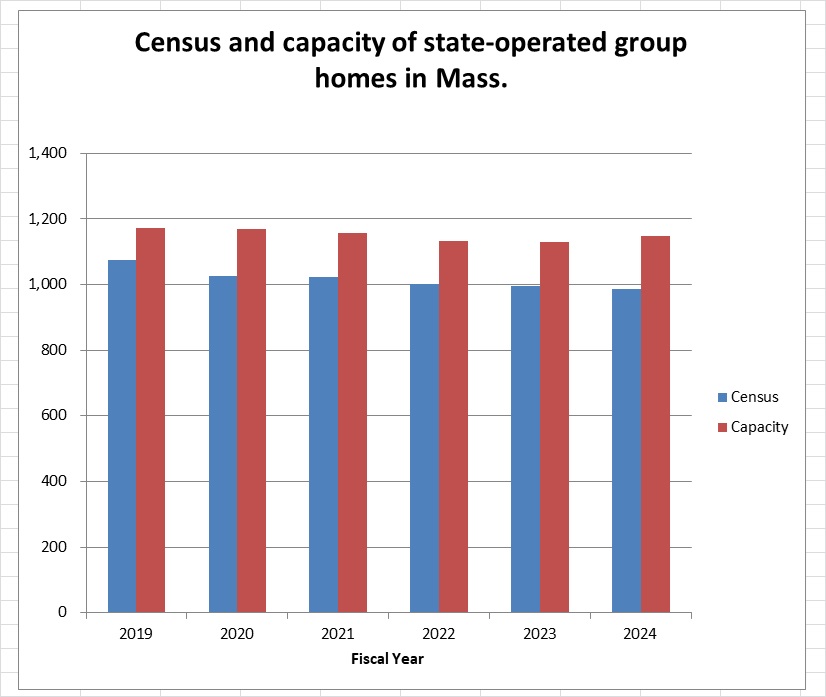
As the chart below shows, the capacity in the state-operated group home system was close to 1,150 in the just-ended Fiscal Year 2024 (as of June 30). But the total census was only 986.
Source: DDS
The capacity as of June 30 was 16.4% higher than the census, implying that there were as many as 162 vacant beds in the state-run group home system that year.
The chart further shows that while the census (depicted by the blue columns) has steadily declined in the homes since Fiscal 2019, the capacity (red columns) declined through Fiscal 2022, and then began to rise in 2023 and 2024.
The gap between the census and capacity of the homes since Fiscal 2019 can be seen in the differences in the heights of the blue (census) and red (capacity) columns in the chart. That data appear to imply that the number of vacancies in state-operated homes has been rising since Fiscal 2022.
DDS, however, states, as noted, that it cannot confirm the number of actual vacancies in the homes because it doesn’t track them. The Department also maintains that vacancy numbers are “more complicated” than the difference between a group home’s census and its capacity.
DDS stated that the number of vacancies in group homes is “complicated” because it is “dependent on a number of real time factors, including but not limited to the temporary placement needs of individuals, staffing, and other group home demographics.”
It’s not clear to us what DDS actually means by that statement. It is not clear why the number of vacancies, for instance, would depend on staffing in the homes. In that case, it would seem that capacity would also depend on staffing. Yet, DDS was able to provide us with data on that capacity.
DDS’s reference to the temporary placement needs of individuals would appear to imply that the total census in the homes also changes over the course of the year due to temporary placements of certain individuals. Yet in that case as well, DDS was able to provide us with data on the census in the group homes.
It is unclear why DDS is able to track both the census and capacity of the homes, yet can’t or doesn’t track the number of vacancies. All three of those variables – census, capacity, and vacancies – would appear to depend on either staffing or temporary placements. Why are vacancy numbers more complicated than either census or capacity numbers?
The DDS data on the state-operated group homes raise many questions, as we’ve said. Unfortunately, DDS has repeatedly declined to answer our questions about the data.
We hope that the additional records DDS is scheduled to provide us about the one-time exercise it conducted will shed a little more light on the important vacancy question.
