Archive
Guardians and two group-home providers say no to day program re-openings due to COVID-19 risk
While Governor Baker has given the go-ahead to the reopening of day programs for persons with intellectual and developmental disabilities in Massachusetts, at least two group home providers are either declining to send residents to the programs or recommending that they not go until a COVID-19 vaccine is found.
Two guardians also told us they won’t sign a form that day programs have been issuing at the administration’s direction that would absolve the providers of liability should any of the clients become infected.
The release form has been issued by the Executive Office of Health and Human Services (EOHHS), according to a residential and day program provider to the Department of Developmental Services (DDS).
Neither DDS Commissioner Jane Ryder nor DDS Ombudsman Chris Klaskin responded to a query from COFAR last week about both the release form and the safety of reopening the day programs.
Thrive and NRS both recommending not to send residents to reopened day programs
In a July 23 email to guardians and family members, an executive officer with Thrive Support & Advocacy, a DDS residential provider, stated that they had concluded that “the day program environment poses too much of a health risk to our Thrivers and staff at this time.”
The email from Denise Vojackova-Karami, vice president of developmental services, added that the planned August 3 day program re-openings would “negate the precautions we have taken thus far. This decision was not made lightly, and we will revisit it if Massachusetts virus numbers continue to decline.”
Meanwhile, Scott Kluge, director of Northeast Residential Services (NRS), a regional DDS manager of state-run group homes, stated in a July 20 message to guardians that “it is our preference that our residents do not immediately rush back to their day programs.” Kluge said NRS “would feel more comfortable …if there is a universally accepted vaccine in place” first.
Kluge maintained that NRS has an additional concern about safely transporting residents to their day programs “as there is really no way to maintain social distance while in a van.” He added that “several families have already reached out to us expressing the same concerns.”
The release form, which was reportedly drafted by a provider trade association at the direction of EOHHS, asks that guardians:
…acknowledge the contagious nature of COVID-19 and voluntarily assume the risk that you or your loved one may be exposed to or infected by COVID-19 by attending a (provider-run day) Program, and that such exposure or infection may result in personal injury, illness, permanent disability, and possibly even death. You understand that this risk may result from the actions, omissions or negligence by you or your loved one, any employee, and/or other clients at the program.
Ryder has not commented
In a July 23 email to DDS Commissioner Ryder and Ombudsman Klaskin, COFAR posed a series of questions about the safety of the day programs and the need for the release form. Among our questions were the following:
- Do you agree that in attending day programs, DDS clients face an increased risk of contracting COVID-19?
- What is your understanding of the meaning of “voluntarily assuming the risk” of being exposed to or contracting the virus?
- Is this agreement intended to hold day program providers harmless from lawsuits and to shift responsibility to a third party?
- What happens if a guardian or family member declines to sign the agreement?
- Is the agreement a de facto admission that day programs are unsafe right now?
- Will all day provider staff be tested weekly?
- What specific transportation plans will be implemented to protect the clients?
- Will masks be mandatory in day programs? The agreement states only that masks are recommended.
- How will clients without guardianship or representatives be responsible for signing a legal document?
- Why is there an apparent rush to open day programs when clients are still largely being quarantined in their group homes?
As noted, neither Ryder nor Klaskin have responded to the July 23 query. Ryder and Klaskin have also not responded to previous questions from us about the scope of the DDS COVID-19 testing program in the DDS system.
Guardian says release form presents a false and dangerous choice
Neil Ferris, whose brother Eugene is a resident of a Thrive group home, said his brother had been attending a day program in Northborough operated by the Justice Resource Institute (JRI) for more than seven years. Ferris termed it a “well run program with good staff and a full-time nurse.”
He added that the day program provided “a very important outing each day for socializing, having relationship with others and enjoying some fun activities..” But he is concerned that the program opens up interactions with clients from many other Metro West locations, and “raises the concern of virus transmittal.”
Without a mask requirement, Ferris maintained, the day program arrangement “places all at risk. If a client cannot wear a mask for a number of reasons, that client should not attend the program.”
Ferris said that while his 66-year-old brother needs the day program to stay active mentally and enjoy a life outside of his room at his house, “JRI places us in a terrible position. If I don’t sign (the release form), I deprive my brother of a good life. If I do sign it, I place my brother at serious risk with his many underlying health issues as almost all other clients have.”
While Andy Pond, JRI’s pesident and CEO, told COFAR that JRI would provide remote activities for clients if guardians declined to sign the release form, Ferris doesn’t believe that will be the case. “JRI cannot and will not provide any ‘at-home’ resources for those who do not sign,” he wrote in an email to us.
Ferris said he believes that JRI and other day program providers are placing their financial concerns ahead of their clients’ safety. “They should not open day programs until such time as they can safely protect their clients, and they should eliminate the legal release absolving them of any responsibility.”
Ferris said he believes Thrive has determined that their clients should not attend day programs “because it is way to soon, safety protocols at JRI are insufficient, and some clients lack the capability to follow safety guidelines.”
Pond maintained that “our (day program reopening) process has been careful and deliberative, and we have proceeded according to the best information we have access to.”
Mother says daughter would be at risk
The mother of an NRS group home resident said she agrees with NRS that it will only be safe for her daughter to go back to her day program after a vaccine is developed. She said she is not only concerned about safe distancing at the day program and on the transportation van, but her daughter could not tolerate a mask for that amount of time.
“I think asking parents and guardians to sign a waiver is ridiculous,” the client’s mother said. “That waiver would absolve them of any responsibility.”
We fully support the positions of those residential providers and guardians who think it would be best to wait for the development of a vaccine before opening day programs for DDS clients. And we support those guardians who are refusing to sign a form absolving the day program providers of liability.
What does DDS think about all of this? We don’t know. As far as we can tell, Commissioner Ryder has not even put any information for guardians and family members about the day program situation on the Department’s website.
What families and guardians need right now is information and leadership from DDS and the administration in general, and it doesn’t appear they’re getting it.
Release form sent to guardians to protect DDS day program providers from COVID-19 liability
As day programs for persons with intellectual and developmental disabilities open as scheduled in coming weeks, guardians are being asked to sign a release form that would absolve day program providers of legal liability if a client contracts COVID-19.
The release form has been issued by the Executive Office of Health and Human Services (EOHHS), according to the Justice Resource Institute (JRI), a provider contacted by COFAR.
COFAR reviewed the form, which was provided by a guardian of a JRI client, and contacted Department of Developmental Services Commissioner Jane Ryder with questions about the form on Thursday. Ryder has not responded to our query.
According to Andy Pond, JRI president and CEO, guardians can opt not to sign the form. In that case, day program services will be provided remotely, Pond said. He said that while the form was issued by EOHHS, it was actually drafted by a provider trade association.
COFAR President Thomas J. Frain, an attorney, said he would advise guardians not to sign the form. He also maintained that he does not believe on-site day program services can be denied even if a guardian declines to sign the form.
The release form appears to be part of a trend among government agencies and providers of all types to gain immunity from lawsuits stemming from the pandemic.
But as one advocate put it, “How can we give all providers an incentive to oversee staff and provide adequate staffing when there is no potential liability for simple negligence or even gross negligence? Some will do the right thing regardless, and some may not.”
And as one guardian stated, the form is “a legal protection document for the providers, not the clients. It forces clients and families to take unneeded risks for services.” The guardian added that he knows of no services “that can be performed remotely, as they are all group centered.”
Among other things, the release form states that:
(The day program provider) cannot guarantee that an Individual will not be exposed to, contract, or spread COVID-19. Further, attending a Program for in-person services increases an Individual’s risk of contracting COVID-19.
In addition, guardians or clients are asked to sign the form and to assert that they:
…acknowledge the contagious nature of COVID-19 and voluntarily assume the risk that you or your loved one may be exposed to or infected by COVID-19 by attending a (provider-run day) Program, and that such exposure or infection may result in personal injury, illness, permanent disability, and possibly even death. You understand that this risk may result from the actions, omissions or negligence by you or your loved one, any employee, and/or other clients at the program.
Finally, in signing the form, the guardian or client states that they “…freely and knowingly assume the risk as described above.”
The following are some of the answers to COFAR’s questions that were provided by Pond, the CEO of JRI. We asked these same questions of DDS Commissioner Ryder, who, as noted, hasn’t responded:
Is the release form a de facto admission that day programs are unsafe right now?
JRI is following all requirements to minimize the risk of COVID transmission at the program, although it is of course true that until there is widespread access to a vaccine, no environment (other than isolation) is 100% “safe.”
Will all provider staff be tested weekly?
Staff will receive temperature and symptom checks prior to the start of each shift. Staff will be tested if they have symptoms or if they have reason to believe that they may have been exposed. As an agency, we recently hired a full time “covid nurse” who helps coordinate testing and consults on contact tracing, etc.
We understand that EOHHS is currently considering policies which may require periodic (sometimes called “survelliance”) testing of staff.
Will JRI report all infections to clients and representatives?
Yes.
What specific transportation plans will be implemented to protect the clients?
Transportation to and from dayhab services is not provided by JRI. We understand that transportation vendors will be following EOHHS Guidance when they resume services, including: screening and hand-washing for drivers and passengers before and after each trip ; distancing rules on vehicles; use of masks by drivers and preferably also by riders; and cleaning and sanitizing procedures.
We expect JRI to offer very limited transportation as part of dayhab services, such as community outings, but will be following that same Guidance. We have procedures to screen drivers and riders, for hand-washing, for mask wearing, and for enhanced cleaning and sanitizing.
The capacity of each van is limited, with a protective barrier in place between the driver and passengers, and passenger seats limited to one person in every other row.
Will masks be mandatory in day programs? The agreement states only that masks are recommended.
Masks will be mandatory for staff and recommended for clients. Some clients are not able to wear masks because of health conditions not related to COVID.
How will clients without guardianship or representatives be responsible for signing a legal document?
Under the EOHHS Guidance, they are required to sign or verbally acknowledge their acceptance.
Why is there an apparent rush to open day programs when clients are still largely being quarantined in their group homes?
Our process has been careful and deliberative, and we have proceeded according to the best information we have access to. EOHHS permitted opening sites in early July. We will be reopening in August at reduced capacity and all clients have the option to continue to receive services remotely.
Pond added that he wanted family members with questions to “reach out to the program directly.”
The fact that the Baker administration is issuing this form to guardians says some good and bad things about the administration’s continuing response to the pandemic. It’s a good thing that the administration recognizes the continuing threat that the virus poses in the DDS system even as they assert that infection levels are falling.
It continues to be troubling, however, that the administration is not taking basic precautions such as requiring mandatory testing of staff in day programs and group homes. Instead, the strategy appears to be to protect providers from liability even if infected staff are negligently admitted into DDS facilities where they then infect clients.
As usual, the process lacks accountability and transparency. The administration wants to protect itself and its providers from responsibility if clients get sick, and the administration continues to ignore basic questions from advocates and families about their policies.
Administration keeping records hidden and declining comment on COVID-19 in DDS system
The Baker administration seems to be going out of its way to avoid providing information to us regarding the impact COVID-19 has had on persons with intellectual and developmental disabilities in Massachusetts.
We have four outstanding Public Records Requests with three state agencies – the Executive Office of Health and Human Services (EOHHS), the Department of Developmental Services (DDS), and the Department of Public Health (DPH). In none of the cases have we received responsive documents.
Administration officials also don’t appear even to want to talk about their response to the pandemic. Neither HHS Secretary Marylou Sudders nor DDS Commissioner Jane Ryder have responded to our repeated questions over the past several months about the lack of mandatory testing of staff in the DDS system for COVID-19.
A key state lawmaker also declined to clarify her apparently erroneous remarks recently made to a COFAR member about why mandatory testing of staff isn’t being done. (More about that below.)
Ryder also has refused to respond to our questions about the administration’s apparently haphazard policy on retesting of persons in the system or the slow pace of testing of both residents and staff.
For instance, one parent of a resident in a state-operated group home said his daughter has been tested four times in her group home since April, and has been negative each time. Meanwhile, approximately 1,400 residents in the DDS system haven’t even been tested once.
We are concerned that if a second wave of the virus hits Massachusetts, DDS’s lack of a coherent policy on retesting could be tragic.
No mandatory testing records provided
Our longest-running Public Records request to the administration is for internal emails and other documents relating to the topic of mandatory testing of staff in the DDS system. As we have reported, DDS does not require staff to be tested even though it is likely that much of the spread of the virus in group homes has been caused by asymptomatic staff.
I first asked EOHHS, DDS, and DPH on May 26, more than a month and a half ago, for emails and other records regarding mandatory testing, and so far none have been provided. The stories keep changing from EOHHS as to whether they have any such records.
First, EOHHS said in early June that they had so many records that the cost could potentially be prohibitive to provide them to us. But after I narrowed down my request at their suggestion, they said earlier this month that they have no responsive records. I filed an appeal with the state Public Records Division on July 14.
EOHHS has also failed to provide us records I requested on June 16 relating to a contract with Fallon Ambulance Service, which is carrying out the testing in the DDS system.
Among the records I asked for were records showing how much Fallon had been paid since they started the testing work on April 10, and copies of daily reports, which the contract requires Fallon to submit to EOHHS.
We have also have not yet received any records, which I asked for on June 25, concerning the online reporting system used by DPH regarding COVID test results in the DDS system. We want to know why the reporting system has been changed from cumulative data to current data, and why the site shows only currently positive cases.
DDS itself has provided cumulative COVID testing data to us, but the Department refuses to display the data on its website where the public could access it on a daily basis.
No indication whether administration has discussed mandatory testing
To date, no one in the administration has given us a reason for the decision not to make testing of staff mandatory in the DDS system.
On May 26, I asked EOHHS, DDS, and DPH for internal emails, memos and other records relating to internal discussions of the topic.
To date, I have received zero documents in response to my request. As a result, on July 14, I filed an appeal with the state’s Public Records Supervisor.
It’s hard to believe that there have been no such internal discussions at the highest levels in EOHHS.
EOHHS story keeps changing on the records it has
On June 9, when a response was legally due under the Public Records Law to my May 26 request for documents, an EOHHS records officer told me initial searches of emails of all EOHHS personnel using the term “mandatory testing” resulted in such a voluminous number of documents that the cost of reviewing and reproducing them would be potentially prohibitive.
As a result, I agreed to the records officer’s suggestion that I narrow the requested communications to Secretary Sudders and her executive team, and narrow the time frame to a period between April 1 and June 1, 2020.
About a month went by, and I received no further word or documents from EOHHS or from DDS or DPH. On July 9, after I queried EOHHS, the records officer said he had a “responsive record” and would provide it by July 13. When no response was forthcoming by July 14, I appealed to the Public Records Division.
The next day, the EOHHS records official emailed me to say that he had been mistaken about the responsive record, and that EOHHS actually had no records that were responsive to my narrowed request.
So, in the month and a half since my original Public Records Request, EOHHS had gone from having a voluminous number of records in response to it, to having zero records after I narrowed the request according to their suggestions.
So, I asked on July 15 if EOHHS could redirect their search to the highest-level personnel in the agency whose emails did include references to mandatory testing in the agreed-upon time frame.
Secondly, I asked for an explanation as to why it had taken more than a month since our June 9 agreement on narrowing my records request to do a search of the emails of the secretary and her team, which then came up empty. To date, I have received no response to those follow-up questions.
DPH wanted to charge us for records … then did not respond to us
On June 17, DPH responded to my May 26 Public Records request regarding mandatory testing records with a letter stating that that agency had identified more than 2,700 emails that might be responsive to my request, and that providing all of them would cost us more than $1,600.
In a June 18 email to the DPH records officer, I offered to similarly narrow my request to communications involving DPH Commissioner Monica Bharel and her executive team and to a time period from April 1 through June 1. To date, I have not received a response from DPH to my offer, nor have I received any records.
State lawmaker declines to support claim that mandatory COVID testing is prohibited by statute
In a July 7 email to a COFAR member in response to a question about mandatory testing of staff, state Representative Kay Khan stated that she has been advocating for increased testing in the DDS system.
Khan, who is House chair of the Children, Families, and Persons with Disabilities Committee, said it was her understanding, however, that requiring mandatory testing of staff is not allowed by statute and that the Massachusetts General Laws would need to be changed through legislation for this to become policy.
We at COFAR are not aware of any such statute that would prevent mandatory testing. In an email to Khan on July 8, I asked if she could provide a citation of the statute she was referring to. Khan has not responded to my query.
No new records provided regarding Fallon COVID testing contract
On June 16, I asked EOHHS for documents relating to a contract with Fallon Ambulance Service to test residents and staff in the DDS system. We had previously received the contract itself from EOHHS.
Among the documents I asked for on June 16 were records showing how much Fallon had been paid since they started the testing work on April 10, and copies of daily reports, which the contract specifically required Fallon to submit to EOHHS.
In its response on July 16, a month later, EOHHS provided only the same contract it had provided earlier. The EOHHS response stated that the agency had no daily reports from Fallon, but that we should ask DPH for those.
As far as payment to Fallon, the EOHHS response stated that I should go to the Comptroller’s online database at https://www.macomptroller.org/cthru. This database, however, does not make it clear how to determine payments made to contractors.
For instance, when I did a search for Fallon Ambulance, the Comptroller’s site appeared to indicate that the last time Fallon Ambulance was paid was in Fiscal Year 2018. When I checked it, the site listed $0 paid to the company in the previous and current fiscal years.
I emailed the EOHHS records officer about the problem with his agency’s response to my Public Records request yesterday (July 20.) I have not received a reply.
DPH ignores Public Records Request regarding its reporting system
On June 25, I asked EOHHS, DDS, and DPH for documents concerning the weekly online data reporting system used by DPH for testing results in the DDS system. We wanted to know why the reporting system had been changed from cumulative data to current data, which shows only currently positive cases.
Both DDS and EOHHS stated they would provide a response by July 17. To date, however, I haven’t received that response from either agency. I have received no communication from DPH since filing my June 25 Public Records request.
As a result, I appealed to the state Public Records Supervisor on July 16, specifically regarding the lack of response from DPH.
It’s not clear to me what, if anything, the Public Records supervisor is going to do about any of these matters.
In any event, maybe it’s just us, but is anyone else sensing a pattern here? After initially seeming responsive to our information and records requests when the viral pandemic first appeared in March, the administration has become increasingly secretive.
We are at a loss to explain this apparent lack of transparency. Overall, the administration has been getting high marks for its response to the pandemic. Massachusetts is one of the few states in the nation in which the rates of infection have been declining.
But when it comes to the DDS system, the administration just doesn’t want to answer any questions.
ACLU and SEIU surprisingly and confusingly gang up on congregate care for the developmentally disabled during COVID crisis
The American Civil Liberties Union (ACLU) and the Service Employees International Union (SEIU) are usually strong advocates of accountability and transparency in government.
That’s why it is surprising that both of those organizations appear to be using the coronavirus pandemic to further a longstanding agenda, which we never knew they shared, to privatize services to people with intellectual and developmental disabilities.
It’s particularly surprising that the SEIU, a human services employee union that represents caregivers in the state’s two remaining developmental centers, would be on board with closing down state-run care facilities.
In a petition filed June 23 with the U.S. Department of Health and Human Services (HHS), the ACLU, SEIU, and a number of other advocacy organizations appear to start off on the right track in criticizing the federal government for its mismanaged response to the pandemic.
The petition identifies nursing homes, Intermediate Care Facilities for the developmentally disabled (ICFs), and group homes as sites of large numbers of COVID-19 infections and deaths that could have been prevented with better guidance for infection control, more testing, and better patient and worker protections.
But the petition then goes on to make a number of, at times, poorly conceived and even confusing claims and recommendations that ultimately appear intended to support a privatized care agenda.
At least some of the confusion centers around group homes, which the petition lumps together with ICFs as sources of “congregate care.”
The petition suggests that among the causes of the infections and deaths is the federal government’s failure “to divert people from entering nursing homes or other congregate settings” or to increase discharges from those settings “to the community.”
The argument the petition makes is that reducing the population in all of those facilities would “make social distancing possible.”
The petition defines congregate settings as including ICFs, psychiatric facilities, and group homes. Yet, group homes are considered part of the community-based system of care in Massachusetts and other states. As a result, it isn’t clear what the ACLU and SEIU mean in stating that people living in group homes would be among those in congregate settings who should move “to the community.”
The petition, moreover, calls for reducing the population of nursing homes and congregate settings by 50 percent. Should HHS neglect to act within three weeks to enact that and other suggested measures, the groups will sue, the petition states.
It is unclear whether the ACLU and SEIU mean that nursing homes, ICFs, and group homes should all be emptied of 50 percent of their residents, or where those residents would then go.
VOR, COFAR’s national affiliate, issued a statement sharply critical of the petition, maintaining that:
…the ACLU has cast its net too wide, and falsely claimed to represent the interests of everyone receiving federally funded services who is classified as elderly or who has intellectual and developmental disabilities. In doing so, it apparently assumes that all such persons look and feel alike and need the same supports and level of care.
Further confusion over the HCBS waiver
Adding to the confusion over group homes is language in the ACLU/SEIU petition calling on HHS to “provide incentives to states to redesign their Medicaid programs to expand Home and Community Based Services (HCBS) and other community-based services and supports” with the goal of the 50 percent reduction in the population in congregate settings.
Once again, that language is confusing in that group homes in Massachusetts and other states have long been recipients of federal funding under an HCBS waiver of Medicaid regulations governing ICFs. In asking for an expansion of Medicaid funding under the HCBS waiver, is the petition suggesting that the money go toward care in a setting other than group homes?
ACLU/SEIU petition misreads the Olmstead Supreme Court decision
The ACLU/SEIU petition further misreads the landmark Olmstead v. L.C. U.S. Supreme Court decision, which paved the way for expansion of privatized care. Although the 1999 decision held that community-based care should be made available for those who desire it, it nevertheless recognized the role played by institutional care for those who can’t function under community-based care.
The Olmstead ruling stated that the Americans with Disabilities Act (ADA) “does not condone or require removing individuals from institutional settings when they are unable to benefit from, or do not desire, a community-based setting.”
We have asked the SEIU’s Massachusetts affiliate, Local 509, whether it is in support of the ACLU/SEIU petition. We have not heard back yet, but we hope they are in a position to disavow it.
There is a lot to be concerned about regarding the efforts of both the federal government and the state government here in Massachusetts to protect persons with intellectual and developmental disabilities from the virus. We’ve raised a lot of those concerns over the past few months.
At the same time, and for that reason, we don’t think it is appropriate for any organization to use the pandemic to support an anti-institutional agenda.
Baker administration now relying on provider claims, not tests, to measure COVID-19 rate in DDS group home system
Since early April, the coronavirus has been found in group homes run by more than 80% of the providers to the Department of Developmental Services (DDS), and in more than 3,400 residents and staff in the Department’s system.
Yet, according to the state’s online Weekly State Facility Reporting site, only between 7 and 12 residents are currently COVID-19 positive in the entire DDS group home system. That report stated that its data was current as of June 30.
How is it possible that the virus could have infected so many people in the system on such a widespread basis since April, and yet so few people are currently infected?
Have more than 1,300 residents alone recovered from the virus, as the weekly report claims, or is the low number of residents listed as currently positive wildly inaccurate?
It may be impossible to answer that question, given what appear to be:
- a significant slowdown since May in actual testing for the virus in the DDS system,
- an apparent reliance by DDS on reporting by the providers themselves of the number of COVID-positive residents and staff in their group homes, and the number who recovered, and
- major gaps in the data reported by both DDS and the Department of Public Health (DPH) on the incidence of COVID-19 among persons in Massachusetts with intellectual and developmental disabilities.
First, there appears to have been only a minimal level of testing done in the DDS system over the past month and a half, and virtually no on-site monitoring by DDS of the group home system. As I’ll discuss below, the downturn in testing since late May appears to correlate strongly with reporting by DDS of continuously lower numbers of new positive cases during that period.
Secondly, without the testing to determine the ongoing level of infection, DDS has apparently been relying on the providers to report accurately to it. It is unclear, however, how the providers are able to determine whether residents or staff are COVID-positive if they are not being tested.
It would seem that the most the providers can report with any degree of confidence is whether residents and staff are displaying symptoms. But as has been widely reported, asymptomatic or pre-symptomatic people can still be COVID-positive and are able to transmit the virus to others.
Thirdly, with regard to gaps in the data, the weekly state facility reports do not include the number of currently positive staff in provider-run group homes, so we have no idea what the total number of positive people in the system is right now.
The latest weekly state facility report states that as of June 30, a total of seven residents in provider-run group homes and less than five residents in state-run group homes are currently positive with COVID-19. The report also states that a total of 1,346 residents in all group homes in the DDS system had recovered from the virus. No information is given of the number of staff in provider-run group homes who are positive or the number of recovered staff.
“Recovered” individuals are defined in the reports as those who “have tested negative or have met symptom and time-based recovery guidelines issued by the the state DPH and the federal CDC.” (my emphasis).
The definition of recovered individuals appears problematic because those symptom and time-based recovery guidelines state only that a staff worker can return to work if they have been symptom-free for a total of three days. The guidelines don’t ensure that the individual is not still COVID-positive or potentially capable of transmitting the virus to others.
Nevertheless, it appears DDS has been relying more and more on reports by providers of the number of people in group homes displaying symptoms, and is no longer relying on testing to determine the number who are currently positive.
DDS has never answered our repeated question as to whether and where retesting is being done throughout the group home system. The Department also stated that it keeps no records on the number of residents reported as symptomatic. And it has no records on the number of staff who have refused testing.
Positive test numbers have closely tracked the rate of testing
The level of mobile testing done in the DDS group home system by the state’s only contractor for that work, Fallon Ambulance Service, has slowed continuously since a peak of testing activity by the company in late April.
As of July 1, only 80 percent of the residents in the system appear to have been tested, leaving some 1,600 residents and an undetermined number of staff untested since Fallon began on April 10.
In addition, group home staff are not required to be tested and providers can refuse testing in their residences if they report that none of the residents are symptomatic.
All of those factors appear to raise questions whether the apparently declining level of positive COVID-19 cases in the group home system might not, in fact, be due to the lack of testing.
We used DDS data to show what appears to be a strong relationship between a sharply declining rate of testing for the virus since April and declining numbers reported by DDS of new positive cases among residents and staff in the system. In both cases, the numbers have trended downwards since a peak in late April or early May.
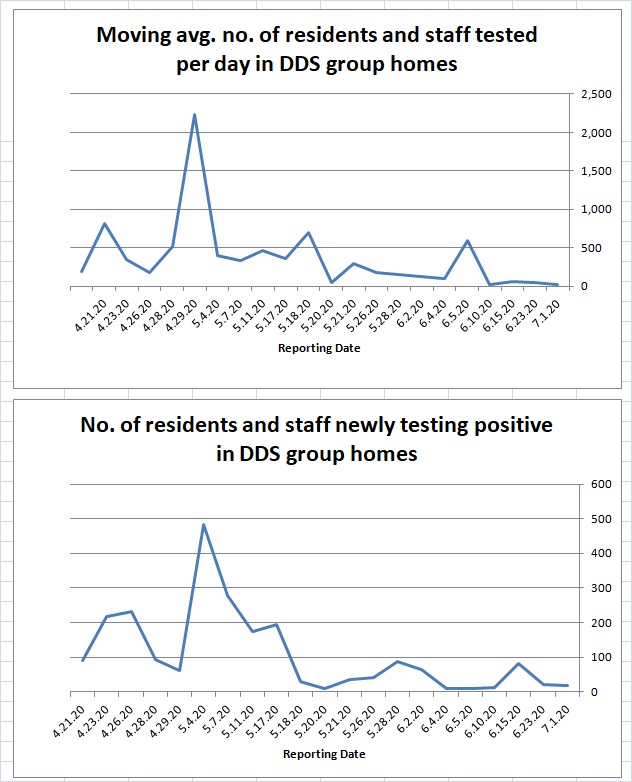
Source: DDS data reports
Both the daily rate of testing and the number of new positive cases show large spikes in late April-early May. The daily testing rate graph shows the spike occurring April 29. The positive cases graph shows the spike occurring on May 4, just five days later.
From late May onward, both graphs show lower numbers of average daily testing and positive COVID cases than had been the case in early May.
Prior to announcing a new, less restrictive policy on visitation last week, DDS Commissioner Jane Ryder stated in an email to COFAR that the number of new COVID cases “have been decreasing in DDS residential programs, much as they have across the state.” She added that DDS believed the reasons for that decline include “the visitation restrictions adopted in March…along with hand hygiene, testing, and mask use.”
Ryder didn’t note the decline in testing itself, and didn’t respond to our questions about the lower rate of testing and the possible impact it was having on the numbers of reported cases.
The administration appears to believe that if the providers are reporting fewer people showing symptoms, there isn’t a need for testing of either residents or staff. Perhaps their strategy is that if the numbers of symptomatic people start to rise, they will ramp the testing back up at that time.
In the meantime, let’s hope the providers are reporting the situation in the group homes correctly to DDS. We have no way of knowing for sure.
