Archive
The burdens of Supported Decision Making will fall primarily on women
Guest post by Lara Dionne
As one of the parent-guardians of a young lady who is 18 years old and has Level 2 autism and moderate intellectual disability, I am very concerned about bills pending in the state Legislature to authorize Supported Decision Making (SDM) in Massachusetts (S.109 and H.201).
SDM would enable persons with developmental disabilities to sign agreements with informal teams of supporters, who would “help” them make decisions about all aspects of their care.
SDM is billed as a voluntary alternative to guardianships of those individuals, who are referred to as the “decision makers” in SDM arrangements. In reality, many proponents of SDM want to eliminate guardianships altogether.
The problem is that decision-making capacity (i.e., legal competency) should be included somewhere in S.109/H.201, and it is not. The bills need to recognize those whose disabilities render them unable to make informed, reasonable decisions in their best interest due to deficits in cognition related to developmental disability, intellectual disability, or a mental health condition which impairs sound judgement.
The legal competency issue is obvious and a blatant oversight. The bills’ proponents can’t have failed to recognize that there are some people for whom the SDM process would be entirely inappropriate. Those individuals need guardians, and in most cases, those guardians are their mothers, sisters, and daughters.
SDM will further destabilize families that are already under stress and take additional agency away from the very people the state is relying on to fill the gaping holes in their disability services infrastructure: primarily women.
SDM is a means to the end that the state appears to be seeking. In most cases, the “decision-maker” will choose the course recommended by his or her SDM “team.” That team is likely to consist of providers and Department of Developmental Services (DDS) personnel, in addition to family members.
As a result, it is likely that few “decision-makers” will choose congregate care facilities, and many may choose the lowest-cost option — their family home. Even now, well over half of adults with autism live with family caregivers, according to the Children’s Hospital of Philadelphia’s Center for Autism Research.
In case the obvious needs to be stated: It is still overwhelmingly women who take on the burden of caregiving for the disabled in the family home.
Women comprise just over 80% of stay-at-home parents. The Institute on Aging reports that 75% of all caregivers are women, and that female caregivers may spend as much as 50% more time providing care than men. Further, research completed at Drexel University found that 30% of families with a child with autism had to reduce working hours to care for their child.
Given the first two statistics, what do you suppose the likelihood is that those leaving work to provide care for autistic family members are women? Pretty darn high, I would say.
I would also love to know how many of these disabled individuals are cared for by their grandmothers because the state already burned through their parents with the weaponized incompetence that passes for disability services for this population. However, I suspect this is a set of statistics the state does not want to gather for many reasons.
My concern is that S.109/H.201 is yet another bit of health and human services legislation that claims to give autonomy to one oppressed class of individuals by taking away the autonomy of another oppressed class whose members will be expected to suffer the financial fallout and complete any labor associated with it: women.
It is worth considering the following: Is the state entitled to rely on the free labor primarily of women to fill in their programming gaps while they dismantle state-run services and outsource them to unstable private vendors? Is the state entitled to the free labor of women to care for legal adult citizens? I do not think it is.
When most children grow to adulthood, their parents can then focus on their career and build financial security with the goal of retiring someday. Why does the state think that parents ― again, mostly mothers ― of adult children with disabilities are not entitled to that?
I was shocked to learn that, in Massachusetts, parents and guardians cannot be paid caregivers under most MassHealth programs, including adult foster care and personal care attendant services. There is currently a crisis-level shortage of professional caregivers for our disabled and elderly. Yet Massachusetts will not pay families to do the work.
Massachusetts expects that families work for free, and they are getting it. That doesn’t really give the state much incentive to fix the direct care workforce shortage, does it? They are balancing their budgets on the backs of women.
There is proposed legislation this session — S. 775/H. 1232, An Act Relative to Family Members Serving as Caregivers — to undo this overtly exploitative practice of relying on unpaid, mostly female, caregivers in adult long-term care. The bill would allow legally liable individuals, parents and guardians, to be paid caregivers for their adult children under MassHealth programs.
According to Massachusetts regulation (101 CMR 420.00), which governs reimbursement for Adult Long-term Residential (ALTR) Services, the state pays a group home provider over $200,000 a year on average for adult residential services for an individual with autism and intellectual disability. It would seem humane to allow mothers (or other family members) providing the same care to receive a fraction of that $200,000, equal to a living wage.
To elaborate further on the lack of basic human decency extended to unpaid female caregivers of children with disabilities, employees in a group home setting have their employment governed by U.S. labor laws. Depending on the number of employees in their parent company, they may receive health insurance and family medical leave. They may get work credit toward future social security benefits. Many companies that provide group home services give their employees paid time off and overtime pay.
Most importantly, group home employees are able to go home and rest at the end of a shift, away from the demands of their charges. Mom gets none of those things. Her shift never ends. Where was the Department of Labor when mothers were being written out of these MassHealth caregiving programs? Why is the caregiving labor of family members ― again, primarily women ― not seen as labor while someone else does it for pay?
Women who have children with significant disabilities have often been out of the paid full-time workforce for years by the time their child reaches adulthood. It seems that keeping individuals with disabilities and their caregivers in poverty is an intentional feature of most government programs. The poor have no voice. The poor are too busy surviving to object to the violation of their civil rights. The poor become invisible.
When we closed the doors of many institutions, the level of support needed by disabled individuals with more profound disabilities did not decrease or cease to exist. Yet the state assumes that the mystical powers of motherhood will somehow miraculously accomplish what it used to take teams of paid professionals to do.
I urge you all to find and read the excellent article in The Boston Globe last month on abuse and neglect occurring in residential schools for children with autism and intellectual disability. Some people who are being paid, albeit inadequately, to do this labor are resorting to abusing clients.
When an excuse is offered for such egregious violations, it usually mentions the stresses of the job, staff turnover, and chronic understaffing. Still, these employees do have the supports and protections mentioned earlier.
Yet the burden on family caregivers ― primarily mothers ― is inordinately higher and there is no compensation involved. Mothers are expected to endure all that the inadequately compensated direct care workforce endures, and they are expected to do it alone, or while impoverishing themselves to qualify for any state support for their child.
Why is it not expected that this is going to result in domestic violence and child abuse? That would seem logical given what is happening in the paid disability services workforce. It is that mystical power of motherhood again, isn’t it?
The assumption of the right to the free labor of women doing work they cannot possibly do alone, given the lack of available state resources and, in many cases, the level of their child’s disability, is not only misogynistic, it is ableist. Yet SDM is designed to further support the push toward privatization and reliance on “natural supports” when this system can clearly be seen to be failing those with more profound disabilities.
SDM will place additional labor burdens on female caregivers, as well. The guardianship process is onerous enough, as it should be, given its gravity. However, once guardianship is approved, a legal guardian can provide caregiving services without needing to consult a team of people who may be difficult to assemble. It is hard enough for women to take time away from primary caregiving and a job and household demands to perform necessary legal and financial tasks for their adult children with disabilities.
Many of these tasks involve multiple calls, meetings, paperwork, and errands. For example: Has anyone had to apply for SSI on behalf of their adult child? Acquiring a state I.D. for documentation purposes, applying to be their representative payee (because guardianship isn’t enough to represent them with the Social Security Administration), and opening a representative payee bank account are quite a bit of work. Now imagine doing it in committee.
The adult child is not going to be able to perform this labor themselves. I also tend to doubt that their SDM team is going to do much of this work, if the disabled adult lives with family. It will be Mom or Grandma doing it with everyone on the team getting to tell them how to do their job.
Poor, working, and middle-class women will be unable to buy their way out of the caregiving responsibilities that will continue to be forced on them by SDM. The unpaid labor expectations and the micromanagement by a team of individuals, who will have interests and agendas that conflict with the health of the entire family unit, will push many female caregivers beyond their breaking point.
The state knows this, but the state also knows it has mothers over a barrel. At every stage in the life journey of your disabled child, mothers are expected to make a choice: Choose to sacrifice yourself or choose to potentially sacrifice your child’s health and future.
There is never a choice that considers the inherent worth and civil rights of both individuals. It is never mother AND child in disability law. It is solely focused on the child, but it depends upon ― it assumes the right to enlist― the mother’s labor in a manner that sacrifices her health, her career, and her financial independence.
Disability law creates dependency in female caregivers that leaves them vulnerable to poverty and abuse. It removes their agency. The SDM legislation (S.109/H.201) is merely the latest incarnation of disability law continuing that pattern.
It is morally wrong to rely on the lifelong free labor of a particular class of people — based on their sex — to save money and shirk social responsibility. This assumption of the right to the free labor of women bars many women from equal access to educational advancement, civic involvement, and financial security and independence.
Disempowering women further disempowers adults with profound autism and intellectual disability. Many of these adults cannot advocate for themselves. Women ― mothers ― are their voices. If the mothers of the profoundly disabled have no access to the power structure in our society, their children have no voice within that power structure. Their children’s needs go unanswered.
The desire to be able to earn a living wage, to prepare for a somewhat secure retirement, and to protect our physical and mental health does not mean that we women do not love our children and grandchildren. It means that we are people with rights to be considered too.
You can’t give freedoms to one class of people that rely on the continued oppression of another.
___________________________________________________________________
 Lara Dionne is a COFAR member and is currently attending Salem State University, working on a Certificate in Data Analytics, with the long-term goal of getting back into the workforce after many years of caregiving for both her daughter and elderly relatives. She looks forward to being paid for her labors, again.
Lara Dionne is a COFAR member and is currently attending Salem State University, working on a Certificate in Data Analytics, with the long-term goal of getting back into the workforce after many years of caregiving for both her daughter and elderly relatives. She looks forward to being paid for her labors, again.
DDS: We’re ‘not required to answer questions’ about the number of state-run group homes or of residents
As we have reported, the census or number of residents living in state-operated residential group homes and Intermediate Care Facilities (ICFs) in Massachusetts appears to be steadily declining.
But in response to Public Records requests filed by COFAR, first in January and then last month, the Department of Developmental Services (DDS) said it no longer has information on the actual number of people living in state-operated group homes during the past five years.
If it is true that DDS has no such records, it would indicate that the Department is unaware of the status of one of its most important operational programs.
DDS has also declined to clarify an apparent discrepancy in its claims concerning the number of state-operated group homes that have been closed since 2021.
We have appealed to the state’s public records supervisor in an effort to get clarification on those matters. In a response filed on Friday to our appeal, a DDS attorney said that under the Public Records Law, “an agency is not required to answer questions…”
Denial of group home information
Prior to this year, DDS did provide us with information on the declining census in state-operated group homes. That data showed a steady decline from a high of 1,206 residents in Fiscal Year 2015, to 1,097 in 2021. During that same time, the census in the much larger network of corporate, provider run group homes, also funded by DDS, rose from 7,793 to 8,290.
But as of January of this year, as noted, that information on the census in the state-operated group home system is apparently no longer available. What DDS said in January and again in September is that while it can provide information on the total available beds in, or capacity of, state-run group homes over the past five years, it now has no records on the census.
In September, DDS stated that the total capacity of the homes had declined from 1,173 beds to 1,131 beds between Fiscal 2019 and 2023.
But capacity numbers don’t tell the full story, particularly if DDS has not been allowing admissions to the group homes, and there consequently are vacancies in them. In fact, DDS acknowledged last month that there were 91 vacancies in the state-run group home system as of June of this year. That would imply that the actual census in the homes is lower than the capacity.
But DDS also said that while there were 91 vacancies as of June 30, it has no records on the number of vacancies each year since Fiscal Year 2019.
We calculated the apparent drop in the census as of Fiscal Year 2023
Based on the Department’s partial records, we did our own calculation of the census in the state-run group home network as of Fiscal Year 2023. That year, it appears the census would have dropped to 1,040.
That census or number of residents is based on DDS’s statement that the capacity of the state-run group homes was 1,131 in Fiscal 2023, and that there were 91 vacancies in the group homes as of June 30, the last day of that fiscal year. Subtracting the number of vacancies from the census that year equals 1,040. (1,131 minus 91).
If that is the case, it would indicate that the census in the state-run group homes dropped from 1,206 in Fiscal 2015 to 1,040 in Fiscal 2023, a 14% drop. See our chart below.
 (Source: DDS. Note: We were not able to calculate the census in the state-run group homes in Fiscal Year 2022 because DDS did not provide a figure on the number of vacancies in that fiscal year.)
(Source: DDS. Note: We were not able to calculate the census in the state-run group homes in Fiscal Year 2022 because DDS did not provide a figure on the number of vacancies in that fiscal year.)
DDS will not clarify number of homes closed
As noted, DDS is not willing to clarify seemingly contradictory information on the number of group homes that have been closed and subsequently reopened since August 2021, during the height of the COVID crisis.
In September, DDS indicated that a net of nine state-run homes were closed between August 2021 and September 2023, leaving 251 homes remaining. However, eight months earlier – in January — DDS indicated that a net of six state-run homes were closed between August 2021 and January 2023, leaving 250 homes remaining as of January.
The implication of the January data was that 256 homes existed as of August 2021, whereas the implication of the September data was that 260 homes existed as of August 2021. The discrepancy might also mean that the number of homes that DDS said were closed may have been inaccurate.
However, as noted, when I asked that DDS provide clarification regarding that apparent discrepancy, a DDS attorney stated that, “Under the PRL (Public Records Law), an agency is not required to answer questions…”
The Public Records Law does require clarity
As part of our appeal, we stated to the public records supervisor that we believe DDS is, in fact, obligated to clarify information it provides under the Public Records Law.
The Massachusetts Guide to the Public Records Law, updated in March 2020, states that, “(State agencies) must help the requestor to determine the precise record or records responsive to a request…”
Also, the Public Records Law [M.G. L. c. 66, § 6A(b)] states that:
(The state agency) shall: …(i) assist persons seeking public records to identify the records sought;… and (iii) prepare guidelines that enable a person seeking access to public records in the custody of the agency or municipality to make informed requests regarding the availability of such public records electronically or otherwise…Each agency and municipality that maintains a website shall post the guidelines on its website.
In asking for clarification regarding the number of homes that existed as of August 2021 and have subsequently been closed, we were seeking the Department’s help in determining the precise record or records that might be responsive to our Public Records requests.
In sum, DDS’s response to our latest records requests seems to be part of the Department’s usual pattern of providing as little information as it feels it can get away with under the Public Records Law. The only other explanation is that the Department doesn’t have basic information about the programs it runs. We’re not sure which explanation is more troubling.
DDS confirms 91 vacancies in state-operated group homes even after several homes are shut
The Department of Developmental Services has confirmed for the first time that there are dozens of vacant beds in its state-operated group home network, even though the Department also says it has closed a net of nine homes since August 2021.
That information was provided to us in response to a Public Records Request, which we filed earlier this month with the Department.
In a response on September 26 to our request, DDS stated that as of June 30, there were 91 vacancies in the state-operated group home system.
COFAR has long contended that there are vacancies in state-operated homes because DDS generally does not inform individuals seeking residential placements of the existence of that system. Instead, DDS seeks to place virtually all persons in its much larger network of corporate provider-run group homes.
We are frequently told by families seeking placements for their loved ones in the state-run system that there are no vacancies in state-operated homes.
DDS also does not inform or generally admit persons to either of its two remaining Intermediate Care Facilities (ICFs) in the state – the Wrentham Developmental Center or the Hogan Regional Center. As a result, the number of residents living in state-run residential facilities has continued to decline, while the number in corporate run group homes has been steadily increasing.
COFAR has periodically filed Public Records requests with DDS to track the declining census in both the state-operated group home system and the Wrentham and Hogan Centers. The Wrentham and Hogan centers are the last remaining, congregate ICFs in the state.
DDS has continued to maintain that the corporate provider system is less restrictive and better integrated into the community than is the state-run residential system. However, as a Spotlight investigation by The Boston Globe showed on September 27, the corporate group home system is beset by abuse and neglect.
The data provided by DDS on September 26 show the following:
- There were 91 empty beds in state-operated group homes as of June 30. The Department, however, said it “does not have any responsive records” pertaining to COFAR’s request for the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.
- The census, or total number of residents, at the Wrentham Center dropped by 48%, from 323 residents in Fiscal 2013, to 167 in Fiscal 2023.
- The census at Hogan dropped from 159 in Fiscal 2011, to 95 in Fiscal 2023, a 40% drop.
- The total census in the state-run group home system dropped by nearly 10% between Fiscal 2015 and 2021, according to previous DDS data. However, DDS has not provided information on the census in the state-run homes since 2021. We have appealed that apparent information denial to the state supervisor of public records.
- The total capacity, or number of beds, in the state-run group home system declined by 3.6% from Fiscal Year 2019 to Fiscal 2023.
- DDS says it closed a net of nine state-operated homes between August 2021 and September of this year. As noted below, the numbers don’t appear to add up, however. We’ve appealed for clarification.
Declining capacity and census in state-operated group homes
As the chart we created below based on the DDS data shows, the total capacity or number of beds has continued to decline in state-run group homes. That capacity declined from 1,173 beds to 1,131 beds, or by 3.6%, between Fiscal 2019 and 2023.
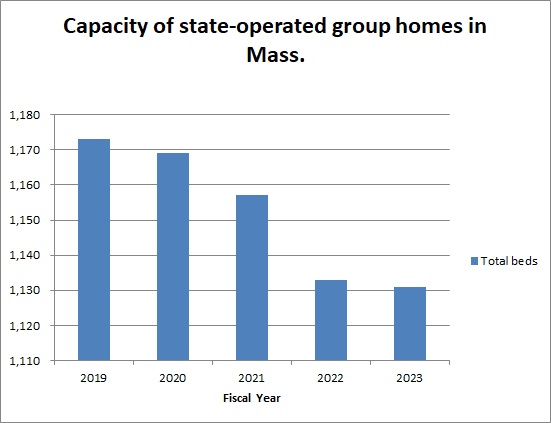
Previous data from DDS showed that the total census in the state-operated group homes declined from a high of 1,206 in Fiscal 2015, to 1,097 in 2021 — a 9% drop.
DDS numbers don’t add up
In addition to appealing the lack of census information regarding the state-run group home system subsequent to 2021, we are appealing to the public records supervisor to seek clarification from DDS regarding an apparent discrepancy in the numbers the Department has given of homes that have been closed since 2021.
The September 2023 DDS response to our Public Records request indicated that a net of 9 state-run homes were closed between August 2021 and September 2023, leaving 251 homes remaining.
However, data previously provided in January indicated that a net of 6 state-run homes were closed between August 2021 and January 2023, leaving 250 homes remaining as of January.
The implication of the January data was that 256 homes existed as of August 2021, whereas the implication of the September data was that 260 homes existed as of August 2021.
We have asked the public records supervisor to require DDS to account for the apparent difference between the two responses in the number of homes that existed as of August 2021.
DDS consistently maintains it has no records regarding the future of state-operated care
Despite the continuing downward trend in the census at Wrentham and Hogan, DDS said in January and again in September that they have no records concerning projections of the future census of those facilities or concerning plans to close them. Nevertheless, we maintain that unless DDS opens the doors at those settings to new residents, they will eventually close.
Violation of federal law not to offer state-run facilities
In a June 5 legal brief, DDS argued that federal law does not give persons with intellectual or developmental disabilities the right to placement at either the Wrentham or Hogan Centers. We think the Department’s argument in the brief misrepresents federal law, and reflects an unfounded bias among policy makers in Massachusetts against ICFs.
As Medicaid.gov, the federal government’s official Medicaid website, explains, “States may not limit access to ICF/IID service, or make it subject to waiting lists, as they may for Home and Community Based Services (HCBS)” (my emphasis). In our view, the federal Medicaid law and its regulations confer the right to the choice of ICF care to individuals and their families and guardians.
Meetings with state and federal lawmakers to bring these concerns to their attention
Last week, we met online with state Representative Jay Livingstone, the new House chair of the state Legislature’s Children, Families, and Persons with Disabilities Committee, to raise our concern about the declining census in state-run facilities and to discuss their vital contribution to adequate care in the system. We are similarly seeking a meeting with Senator Robyn Kennedy, the new Senate chair of the committee.
So far, we have also met online with legislative staffs of U.S. Senators Elizabeth Warren and Ed Markey, and of U.S. Representatives James McGovern, Lori Trahan, Catherine Clark, Seth Moulton, and Stephen Lynch, and have imparted that message. We still have four additional members to meet with in the Massachusetts congressional delegation.
In our meetings with the staff members of the congressional delegation, we are urging that the lawmakers oppose pending bills that would expand funding to the largely privatized, community-based system, but would not direct similar funding to either Wrentham or Hogan.
In sum, the data we have gotten from DDS have shown a consistent pattern by multiple administrations of building up the privatized DDS group home system while letting state-run residential facilities wither and ultimately die. As we’ve said before, we think that will result in a race to the bottom in the quality of care in the DDS system.
In our experience, state-run residential facilities in Massachusetts, as in most other states, meet higher standards for care than do privatized settings, and tend to have higher paid, better trained, and more caring staff. We want to bring that message to our state and federal legislators before it’s too late.
Latest Supported Decision Making bill offers no improvements over previous versions
We first pointed out problems seven years ago with a bill in the state Legislature that would authorize Supported Decision Making (SDM) in Massachusetts.
SDM involves written agreements to replace guardians of persons with developmental disabilities with informal teams of “supporters” or advisors.
Each year, SDM legislation has gotten closer and closer to final passage in the Legislature; and yet, as far as we can see, the proponents of the bill have not made what we argue are needed changes or improvements to the versions of the bill that they have continued to file.
This year’s version of the bill, S. 109, is no exception. In our view, it has the same problems as the previous versions.
Last year’s version of the bill (S. 3132) passed the Senate in November and died in the House Ways and Means Committee, just one step away from final passage in the full House. At the time, we had urged the Ways and Means Committee not to send the bill to the House for final passage.
As we noted in a previous post about that bill, it lacked provisions to protect the rights of persons with intellectual and developmental disabilities, and their families and guardians.
S.109, this year’s version, is now before the Children, Families, and Persons with Disabilities Committee. We are similarly asking the Committee this year not to advance the bill in the legislative process without making needed changes to it.
Under the bill, an SDM “supporter” or “supporters” would help an individual with an intellectual disability, known as the “decision-maker,” make key life decisions, including decisions about their care and finances. Most people with developmental disabilities currently have guardians, most of whom are family members of those individuals. But SDM proponents maintain that guardianship, even when guardians are family members, unduly restricts an individual’s right to make those decisions.
But persons with severe and profound levels of intellectual disability have greatly diminished decision-making capacities. We think many of those people are likely to be vulnerable to coercion and financial exploitation from persons on their SDM teams who may “help” them make financial decisions that don’t reflect their wishes.
In these situations, family members of persons with developmental disabilities, whom we have found to be likely to act in the best interest of their loved ones, may find themselves outvoted on the support teams by other team members who may stand to benefit financially from the clients’ “decisions.”
Legislation still does not provide a standard for judging the decision-making capacity of the individual
In our view, a key piece missing from the SDM legislation so far has been a standard for the level of intellectual disability above which an individual can reasonably be considered to be capable of making decisions with “support” from clinicians, paid caregivers, and other SDM team members.
As was the case with previous versions of the bill, S.109 defines the “decision-maker” as “an adult who seeks to execute, or has executed, a supported decision making agreement with one or more supporters…”
There is no further specification about the decision maker in the bill. There is no differentiation in the definition between individuals with greater or lesser degrees of intellectual disability, and no consideration whether persons with low levels of cognitive functioning are really capable of making and appreciating life-altering decisions.
As a 2013 article on SDM in the Penn State Law Review stated,
…there is a potentially unavoidable paradox in acknowledging that a person has diminished decision-making capacity but maintaining that he or she is nevertheless capable of meaningfully contributing to decision-making discussions and that the decisions that result from such discussions reflect his or her wishes. (my emphasis)
Also, “Supported decision-making” is defined in S.109 as:
…the process of supporting and accommodating the decision-maker, without impeding the self-determination of the decision-maker, in making life decisions, including, but not limited to: (i) decisions related to where the decision-maker wants to live; (ii) the services, supports, financial decisions and medical care the decision-maker wants to receive; (iii) whom the decision-maker wants to live with; and (iv) where the decision-maker wants to work.
There is no specification as to whether the “supporter(s)” would be family members. In other words, family members could be frozen out of the decision-making process if they were consistently outvoted by other supporters.
Bill doesn’t require court approval of an SDM arrangement
Currently, a person applying for guardianship must state in probate court the reason why a guardianship is necessary; and if they are applying for a full guardianship, the reason why a limited guardianship is inappropriate.
There is no requirement in S. 109, however, that the probate court approve an application for an SDM arrangement. However, S.109 would impose an additional burden in probate court on family members who continue to seek guardianship of their loved ones.
Under S. 109, an applicant for guardianship would now have to state in court, “whether alternatives to guardianship … including a supported decision-making agreement, were considered, (and) why such alternatives to guardianship and supports and services are not feasible or would not prevent the need for guardianship” (my emphasis).
Given that applying for guardianship requires probate court approval, it isn’t clear to us why that shouldn’t also be the case with an SDM agreement, which would entail making the same types of life decisions involving an incapacitated individual. Moreover, it isn’t clear why applicants for guardianships should have an additional burden placed on them in court to show why an SDM arrangement, rather than the requested guardianship, isn’t needed.
No clear protection against financial or other exploitation
S.109 states that, “Evidence of undue influence or coercion in the creation or signing of a supported decision-making agreement shall render the supported decision-making agreement invalid.”
This statement in the bill appears to recognize the possibility that a developmentally disabled individual can be influenced or coerced into signing a SDM agreement. The problem with the bill in this regard is there is no description of the type or level of coercion that would invalidate an SDM agreement. Also, the bill doesn’t specify who would invalidate the agreement in that case.
The legislation states that if a person suspects that a disabled individual is being abused or exploited under an SDM arrangement, they can take their complaint to the Disabled Persons Protection Commission (DPPC). But while the DPPC’s enabling statute authorizes the agency to investigate allegations of abuse and neglect, the DPPC is not specifically charged with investigating cases of alleged coercion in signing agreements.
S. 109 also states that the DPPC and the Department of Developmental Services (DDS) may petition the probate court to revoke or suspend a SDM agreement on the grounds of abuse, neglect or exploitation by supporters. But the bill doesn’t say that either the DPPC or DDS will or must petition the court to revoke the SDM agreement even if they do find abuse or neglect. It says only that they “may” petition the court to do so.
No protection against conflicts of interest, and no funding
Members of an individual’s SDM team who are also service providers to that person face a potential conflict of interest when they advise the “decision maker” about making use of the services they provide.
A Syracuse Law Review article published last year about SDM pilot projects in Massachusetts identified, or at least implied, a number of problems or difficulties associated with SDM, including conflicts of interest involving providers.
The Syracuse Law Review article stated that in the Massachusetts pilot project:
…project staff had frank discussions with the Decision Maker and supporters about any potential conflict of interest and how to draft an agreement to minimize the potential conflict, such as having paid supporters not assist with decision-making support for issues that concern services from the agency paying the supporter (my emphasis).
But like bills that have come before it, S.109 does not require any separation between provider employees and individuals on the SDM team. They can serve in both capacities.
The Syracuse Law Review article also stated that one of the lessons of the Massachusetts and other pilot projects was that “without dedicated funding, ample cash reserves or an extraordinary commitment to Supported Decision Making, it is very difficult for organizations to introduce, implement and help to support Supported Decision Making for a large number of individuals.”
There is no reference in S.109, however, to a potential funding mechanism for SDM in Massachusetts.
No dispute resolution process
The Syracuse Law Review article also recognizes that there are likely to be disputes within SDM networks or teams, and noted that a pilot program in New York State created a “Mediation Module designed as a two-day training for mediators.”
While S.109 and previous versions of the bill would require the Executive Office of Health and Human Services in Massachusetts to establish an SDM training program, none of the bills specify or specified either a dispute resolution process for SDM arrangements or training in dispute resolution.
Families may not fully understand the guardianship rights they will be forgoing
SDM advocates argue that the process is entirely voluntary on the part of the intellectually disabled individual, and that family members can still opt to go to court to apply for guardianship.
But it may be wrong in all cases to assume that someone who has a severe or profound level of intellectual disability has not been coerced into making what may look on the surface like a voluntary decision. Also, while a family member may still go to court to become a guardian, the SDM legislation, as noted, would increase the burden on them to make the case for guardianship.
And while family members might be persuaded to willingly enter into SDM agreements rather than to seek guardianship of their loved ones, we think many family members may not realize the amount of authority they would be ceding in doing so. Under an SDM arrangement, a family member would become just one member of the SDM team.
It has been our experience, that in many disputes over care, family members find themselves pitted against a united front of provider and DDS personnel. This would seem to be a highly likely dynamic in an SDM arrangement.
Unless and until the proponents of this legislation finally agree to address these issues and improve the bill, we can’t support it.
Why we are asking federal and state lawmakers to help save the Wrentham and Hogan Intermediate Care Facilities
We believe individuals with intellectual and developmental disabilities in Massachusetts have a right under federal law to care at the Wrentham and Hogan Intermediate Care Facilities (ICFs).
They also have a right to work opportunities in their day programs and other congregate care settings.
Those rights are under continued assault. (See here and here.)
As a result, we are contacting members of the Massachusetts delegation in Congress and key members of the state Legislature, and are asking them to relay information about those rights to policymakers at the federal and state levels.
It seems to us that most lawmakers and policymakers do not recognize the wide range of functioning and needs among people with intellectual and developmental disabilities, or the importance of giving this population a full continuum of choice. One size does not fit all.
DDS phasing out state-run residential care
The Massachusetts Department of Developmental Services (DDS) is allowing the state’s two remaining ICFs — the Wrentham Developmental Center and the Hogan Regional Center — to slowly die by attrition. We believe the eventual closures of these essential backstops for care of the state’s most profoundly disabled residents will be disastrous.
So far, we have met online with legislative staff of U.S. Senators Elizabeth Warren and Ed Markey, and of Representatives James McGovern, Seth Moulton, and Catherine Clark, and imparted that message. We still have six additional members to meet with in the congressional delegation.
Next week, we will also meet online with staff of state Senator Robyn Kennedy, the new Senate chair of the Legislature’s Children, Families, and Persons with Disabilities Committee. We hope to discuss these issues with Senator Kennedy herself, at some point, and will try to schedule a meeting soon with state Representative Jay Livingstone, House chair of the Committee, and his staff.
We want these legislators to know that DDS has failed to inform families and guardians of individuals in the DDS system of the existence of the Wrentham and Hogan Centers, and, with few exceptions, has denied their requests to place their loved ones in those facilities. The Department is also failing to inform people of the existence of its network of state-operated group homes.
What DDS has done has been to attempt to place virtually all persons waiting for residential services in the much larger network of corporate provider-run group homes that the Department funds.
That policy was explicitly confirmed in a decision earlier this month in which DDS Commissioner Jane Ryder upheld the denial of an appeal by the parents of an intellectually disabled man to place their son at Wrentham.
In that case, the parents presented evidence that their son has received inadequate services in his provider-run group home. He is also facing eviction from the residence, and had been abused by staff employed by his group home and day program provider. But a DDS-appointed hearing officer adopted the Department’s position that “federal law does not entitle the (son) to admission to an Intermediate Care Facility at WDC (the Wrentham Center).”
DDS policy runs counter to federal rules
As Medicaid.gov, the federal government’s official Medicaid website, explains, “States may not limit access to ICF/IID service, or make it subject to waiting lists, as they may for Home and Community Based Services (HCBS)” (my emphasis). The son’s group home in the appeal case is run by a corporate DDS provider that is partly federally funded under the HCBS program.
Unfortunately, in his decision, the hearing officer confirmed that DDS’s policy is the opposite of the federally prescribed policy that states may not limit access to ICFs. The hearing officer stated that he agreed with the testimony of a DDS regional director in the appeal hearing that, “DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.”
In our view, however, the federal Medicaid law and its regulations confer the right to the choice of ICF care to individuals and their families and guardians.
DDS, like many advocates of deinstitutionalization of care for people with intellectual and developmental disabilities, has also regularly misinterpreted the landmark Olmstead v. L.C. Supreme Court decision, which also implies a right to ICF care for those who desire it.
Federal ICF legislation that we support and oppose
In our meetings, we are urging lawmakers in Congress to oppose pending bills that would expand funding to largely privatized HCBS system, but would not direct similar funding to ICFs.
We oppose:
The Latonya Reeves Freedom Act of 2023
- H.R. 2708 (Steve Cohen, D-TN) https://www.congress.gov/bill/118th-congress/house-bill/2708
- S.1193 (Michael Bennett, D-CO) https://www.congress.gov/bill/118th-congress/senate-bill/1193
As Hugo Dwyer, executive director of the VOR, our national affiliate explained, this legislation was proposed by ADAPT, an organization that has “repeatedly called for the elimination of the ICF model.” Dwyer stated that VOR supports “keeping all services available and allowing individuals and their families to choose what is right for them.”
- H.R.547 (Debbie Dingell, D-MI) https://www.congress.gov/bill/118th-congress/house-bill/547
- S.100 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/100
- H.R.1493 (Debbie Dingell, D-MI) https://www.congress.gov/bill/118th-congress/house-bill/1493
- S.762 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/762
Dwyer noted that these latter bills would increase federal Medicaid funding for direct-care wages, which we and VOR support. But those wage increases would be in HCBS settings only, leaving out the ICFs.
We support:
Recognizing the Role of Direct Support Professionals Act
- H.R.2941 (Brian Fitzpatrick, R-PA) https://www.congress.gov/bill/118th-congress/house-bill/2941
- S. 1332 (Maggie Hassan, D-NH) https://www.congress.gov/bill/118th-congress/senate-bill/1332
Dwyer said these bills would help raise wages and training of direct-care staff in all settings, including ICFs.
Work opportunities legislation
With regard to work opportunities for people with intellectual and developmental disabilities, two pending bills in Congress would encourage such opportunities:
We support:
- H.R.1296 (Glenn Grothman, R-WI) https://www.congress.gov/bill/118th-congress/house-bill/1296
- H.R.553 (Glenn Grothman, R-WI) https://www.congress.gov/bill/118th-congress/house-bill/553
The Restoration of Employment Act would give an individual a choice whether to accept employment at a subminimum wage. (This blog post explains why the subminimum wage is needed by people who are unable to compete in the mainstream workforce.)
The Workplace Choice Act states that a program setting in which an intellectually disabled individual is able to interact with “colleagues, vendors, customers, and superiors…” would be considered a “competitive, integrated employment” setting. This would allow people who can’t compete in the mainstream workforce to be provided with work activities in their day programs.
We oppose:
- H.R. 1263 (Bobby Scott, D-VA) https://www.congress.gov/bill/118th-congress/house-bill/1263
- S.533 (Bob Casey, D-PA) https://www.congress.gov/bill/118th-congress/senate-bill/533
- H.R. 4889 (Bobby Scott, D-VA) https://www.congress.gov/bill/118th-congress/house-bill/4889
- S.2488 (Bernie Sanders, I-VT) https://www.congress.gov/bill/118th-congress/senate-bill/2488
The legislation above would make work opportunities harder to find for people who can’t handle mainstream work environments. Those bills would remove the option of the subminimum wage.
A number of family members have joined us in our online meetings with legislators. If you are interested in attending upcoming meetings, let us know. Your stories are vitally important for lawmakers and policymakers to know.
In ruling criticized as biased, DDS denies family’s request to place son at the Wrentham Center
As had been expected, Department of Developmental Services (DDS) Commissioner Jane Ryder last week upheld the denial of a request by a couple to place their intellectually disabled son at the Wrentham Developmental Center.
Ryder upheld a recommended decision by DDS Hearing Officer William O’Connell, who had previously denied a request by the couple to submit a COFAR blog post in rebuttal to a DDS closing brief in the case.
The COFAR post claims, among other things, that federal law gives individuals a right to care in an Intermediate Care Facility (ICF) such as the Wrentham Center.
The couple, who have asked that their names not be used, have sought the Wrentham placement as part of an appeal of their son’s Individual Support Plan (ISP). They contend the DDS-funded corporate provider that operates their son’s group home and day habilitation program does not provide services their son needs, such as nursing, speech and occupational therapy; and they note that these services are provided at Wrentham.
O’Connell’s 24-page recommended decision denying the couple’s appeal was dated July 20. The couple maintain that the language and reasoning in O’Connell’s decision confirms that he held a bias against them and in favor of DDS.
Son had been abused at day hab program and is facing eviction from group home
The couple also stated in their appeal that their son had been sexually and physically abused in his day hab facility. They further stated that the provider sought last September to evict their son from the group home after he had a toileting accident on the group home’s outside deck.
The eviction is currently on hold based on the couple’s objection to it under DDS regulations.
The couple said they are considering an appeal of O’Connell’s decision in state Superior Court. They said their hope is that a win in court would establish a precedent for other families seeking to place their loved ones with intellectual and developmental disabilities at either Wrentham or the Hogan Regional Center, the two remaining congregate ICFs in Massachusetts.
In ruling against the couple, O’Connell cited the testimony of two DDS regional directors during a hearing on the couple’s appeal in April. O’Connell stated that based on that testimony, he concluded that “the assessments and/or goals used to develop (the son’s) ISP…form a more than adequate basis for service planning for (the son), including his needs and treatments.”
O’Connell also stated in his decision that the son’s current services are “the ‘least restrictive’ to meet (his) current needs.”
O’Connell’s decision, however, largely did not address the couple’s contention that the actual services their son has received in his group home are inadequate.
Also, as COFAR pointed out in the blog post, which O’Connell would not allow to be submitted, “a statement that a community-based setting is necessarily less restrictive than an ICF is an ideological position that ignores the evidence.”
Hearing officer appeared to have a bias against the family
The couple further noted to us that the regional directors whose testimony was cited by O’Connell are bureaucrats who are largely unfamiliar with the day-to-day care of the son. Yet, the couple said, O’Connell clearly placed all of his credence in the directors’ testimony and not in their own testimony.
In his final decision, O’Connell used the term “credible” or “credibly” to describe the testimony of the two DDS regional directors at least 14 times, while repeatedly stating that the couple had “not met the burden of proof” and had not provided “probative evidence” to support their request that their son be placed at Wrentham. He didn’t explain why their evidence wasn’t probative.
The mother also told us that during the April hearing, O’Connell had expressed repeated impatience with her, telling her to “get to the point…” She said he never interrupted the DDS attorney.
O’Connell had also stated in his previous ruling that the COFAR Blog post was “not probative” as a reason for refusing to consider COFAR’s rebuttal to the DDS closing brief. The blog post would have required him to address several points including:
- That the federal Medicaid statute does provide a right and choice to individuals and their families to ICF care.
- That care at Wrentham and Hogan is not necessarily more restrictive than in provider-run group homes.
- That the couple’s son’s care in the community-based system has not been successful for the past 13 years, as the DDS closing brief stated, and O’Connell repeated.
- That DDS’s policy for many years of blocking new admissions to both Wrentham and Hogan is likely to result in the eventual closure of both of these vitally important backstops of care for some of the state’s most vulnerable residents.
In his decision, O’Connell also repeatedly stated that the couple had rejected all providers of community-based residential services that DDS had identified for them. But he did not acknowledge that the couple said they did so because they believe the community-based system has failed their son and will continue to do so.
ISP hearing process inherently unfair
COFAR has additionally questioned the fairness of the ISP appeal process, under which both the hearing officer is appointed by the DDS commissioner, and the commissioner then makes the final decision whether to uphold the hearing officer’s ruling. COFAR has called for such appeals to be decided by the state’s independent Division of Administrative Law Appeals.
Hearing officer discounted the impact of sexual and physical abuse of couple’s son
In his decision, O’Connell played down the impact of two incidents of sexual and physical abuse of the couple’s son, which the couple said were part of the reason they don’t believe the community-based system is safe or adequate for him. Both incidents had occurred in the bathroom of the day hab facility.
In one case in 2017, a staff member at the day hab program slapped the son on the head, punched him in the back, grabbed his genitals, and was verbally abusive to him over the course of several days.
In a second case in 2015, the son arrived from the day hab facility with a belt tightened so tightly that the parents couldn’t get it off. They said the belt was used to keep their son from going to the bathroom and moving his bowels. Their son has Crohn’s disease and needs to use the bathroom frequently.
According to the couple, their son cried and screamed when they tried to get the belt off. They said he had clear marks and indentations on his stomach which they photographed. In both cases, abuse was substantiated by the DDS investigations unit.
But O’Connell stated in his decision that:
I credit the (couple’s) concerns regarding (their son’s) well-being and safety given these terrible events, but find they were at day supports, not a residential placement, and thus do not have particular probative effect to the (couple’s) current appeal of the ISP and POC (Plan of Care).
O’Connell also stated, in line with the DDS closing brief, that the abuse happened five or more years ago.
But O’Connell didn’t mention that the same provider that runs the son’s day hab program also runs his group home. Also, there was no evidence presented by DDS or the hearing officer that abuse and neglect in the DDS provider system has become less prevalent in the past five years or that the abuse is unlikely to occur again.
Also, abuse in the provider system in general is not restricted to day programs, but occurs in residential settings. If the son were to be admitted to Wrentham, he would attend a day program there, where the abuse rate is likely to be lower than in the provider system.
We have found that abuse overall is lower in the ICFs than in provider run group homes.
Did not address specific services allegedly missing from the community
In a brief that they filed with their original appeal, the couple stated that there is no speech, occupational, recreational, or vocational therapy available to their son in his group home. The group home provider doesn’t provide those services, but Wrentham does.
The couple also stated that their son’s group home and day hab provider have not assigned a nurse to him or provided the name of a nurse to call in case a medical issue arises. They also said there is no nursing listed on his ISP or day hab service plan.
Also, the couple stated that no one at the group home “knows about (their son’s) health status at any given time.” For instance, they said, no member of the staff was aware their son was due for a colonoscopy in June.
The couple also maintained that in most doctors’ offices in the community, there are no accommodations for individuals like their son who have trouble waiting for long periods of time to be seen by the doctor.
O’Connell’s decision largely did not address these specific issues. However, O’Connell did respond to the couple’s contention that their son is not receiving the proper nursing care, writing that “DDS has indicated they will work with (the provider) and any subsequent residential agency to support (the son’s) specific nursing needs.”
The couple maintained to us, however, that saying DDS will “work with” the provider is a tacit admission that the service doesn’t currently exist, and is not an assurance that anything concrete will be done. Those nursing services, however, do exist at Wrentham.
O’Connell also stated that one of the DDS regional directors “credibly testified” that the couple had stated during an informal conference prior to the hearing that the son’s doctor is “excellent.” While that may be the case, the fact remains that the medical staff at Wrentham are highly trained to deal with people with intellectual disabilities, while medical staff in the community are not.
Also, O’Connell stated that the son’s difficulties in waiting at doctors’ officers “are common and easily managed by staff.” The parents disputed this, saying that if that behavior were easily managed, the problem would have been solved long ago.
Couple says son did not face discharge due to their actions
In his decision, O’Connell, once again adopting the DDS closing brief position, stated that the couple were notified last September that the son’s provider “was looking to discharge (him) from their residential placement services due to the (couple’s) actions, not due to any issue with (the son) or (the provider’s) ability to serve (the son).”
O’Connell did not say what those actions were that the parents allegedly committed. Moreover, the couple disputed O’Connell’s characterization of the matter. According to the couple’s original appeal brief, the incident that led to the discharge notice started when no staff were available in the residence to let their son inside to use the toilet.
The group home blamed the couple following the son’s accident on the group home deck, claiming they failed to clean up the area and failed to notify the staff about it. The couple dispute that charge, saying they used a sheet in their car to clean up the area and then emailed both provider and DDS officials about it.
The couple said there was one other incident that precipitated the discharge notice having to do with a Facebook post that the mother made that was critical of the staff of the group home. Neither of these incidents, in our view, are sufficient reasons to have issued a notice to evict the son. No details were provided in the hearing officer’s decision about either of those reasons for the discharge notice.
In sum, O’Connell’s decision in this case, in our view, shows exactly why the ISP appeal process is inherently unfair to families and guardians. His decision was entirely supportive of DDS’s position, and was entirely dismissive of the testimony and evidence put forth by the parents.
For the reasons the couple enumerated, we too hope they will win in court should they decide to appeal, and that this case would then set a precedent that might serve to save the Wrentham and Hogan Centers and other state-run residential programs and services from eventual extinction.
DDS finally agrees to allow client to stay with shared-living caregiver; but caregiver’s payment will be cut almost 50%
A year after having disenrolled Mercy Mezzanotti from her shared-living program, the Department of Developmental Services (DDS) finally agreed this past spring to allow Mercy to continue to receive shared-living services from her longtime caregiver, Karen Faiola.
But before doing so, the Department’s Worcester area office reassessed Mercy as a candidate for shared-living services, and increased her assessed level of functioning. That move, according to Karen, will cut her previous income for caring for Mercy by close to 50%.
A higher level of functioning implies a lower level of needed services. However, both Karen and Mercy contend that Mercy’s needs and level of functioning have not changed. Mercy was found by DDS in 2004 to qualify to receive Home and Community Based (HCBS) as well as institutional services from DDS.
“They are continuing to punish us,” said Karen, referring to the DDS area office. Karen and Mercy claim both DDS and Venture Community Services, Karen’s former shared-living contract agency, retaliated against them after they alleged that Venture employees abused Mercy emotionally last year.

Karen Faiola and Mercy Mezzanotti
As we argue below, it also appears that the DDS reassessment of Mercy did not comply with departmental regulations. The regulations require that such an assessment be done by a qualified eligibility team and that notice of the reassessment be provided to Mercy.
Income for caring for Mercy would decline from $38,000 a year to $20,000
Karen said she was told last month by Mercy’s new shared-living contract agency that as a result of the new assessment by DDS, her previous annual income for caring for Mercy will be reduced from $34,000, which she had earned under the Venture contract, to roughly $20,000. Also, she will no longer receive a $4,000 respite allocation for providing services.
Both Karen and Mercy contend the DDS Area Office has deliberately sought to reduce Karen’s pay as part of a continuing vendetta against them for having complained last year that two employees of Venture had emotionally abused Mercy. Karen said the pay cut will it very difficult for her to continue to care for Mercy and to survive financially.
Contract termination followed by involuntary removal from home and disenrollment from program
Mercy has been living in Karen’s Sutton home for the past five years. Karen had been Mercy’s paid shared-living caregiver from 2018 until Venture terminated its contract with Karen in May 2022 without providing a stated reason for the termination. DDS pays corporate providers such as Venture to contract directly with shared-living caregivers.
Prior to the contract termination, Mercy and Karen had complained to Venture that a Venture job coach and a second Venture employee had emotionally abused Mercy.
On the same day that Venture terminated its contract with Karen, a Venture employee removed Mercy against her will from Karen’s home and placed her with another caregiver in Worcester whom Mercy had never met.
When Karen, at Mercy’s insistence, brought Mercy back to her home two days later, DDS moved to disenroll Mercy from its federally reimbursed HCBS program. DDS argued that in leaving the stranger’s home, Mercy was refusing DDS services.
Meanwhile, both Karen and Mercy’s therapist filed complaints with the Disabled Persons Protection Commission (DPPC) of abuse of Mercy by Venture. However, a subsequent review by DDS did not result in any findings concerning those charges, indicating that the charges were not investigated.
In July 2022, Mercy appealed her disenrollment to DDS. In February of this year, a DDS-appointed hearing officer upheld the disenrollment, but left the door open for Mercy to “work with” the DDS area office to reapply for shared-living services.
Melanie Cruz, Mercy’s service coordinator supervisor in the DDS Worcester area office, subsequently told Mercy she would refer her to a new shared-living contract agency. But Cruz then texted Mercy in March to say she would have to undergo an eligibility “reprioritization” before she could be “considered for residential services.”
By that time, Mercy had been without a shared living program for more than a year after Venture’s termination of Karen’s contract. Mercy has nevertheless continued to live with Karen, who continued to provide shared-living services to her without financial compensation.
DDS regulations appear to have been violated: No eligibility team and no notice
DDS regulations (115 CMR 6.02(3)) require that eligibility for DDS services be determined by “regional eligibility teams,” each of which must be comprised of a licensed doctoral level psychologist, a social worker with a master’s degree, and a “Department eligibility specialist.”
Karen said the eligibility reassessment of Mercy was carried out in April by Cruz, the service coordinator supervisor, who is employed by the Area Office. In an email I sent on Tuesday to DDS Commissioner Jane Ryder, I stated that having Cruz undertake the reassessment, on its face, does not appear to comply with the regulations.
In addition, the regulations (115 CMR 6.03 and 6.08) state that after completion of an eligibility determination or redetermination, the regional eligibility team must notify the individual of the determination and their right to appeal within 30 days after receiving the notice.
However, Karen said that as of today (August 4) Mercy still had not received a notice of the reassessment. On Tuesday, Mercy texted Cruz, asking for a copy of the reassessment. But Mercy has not received a response from her, Karen said.
Cruz had previously testified against Mercy
In questioning Cruz’s rationale for reassessing Mercy’s level of functioning, Karen also noted that Cruz had previously testified in favor of Mercy’s disenrollment in a November 2022 DDS hearing on Mercy’s appeal. Karen said she believes Cruz was therefore facing a conflict of interest in subsequently reassessing Mercy for shared-living services.
Reassessment reportedly states that Mercy was without services for the past year
Karen was informed that one of the reasons cited by Cruz for the increase in Mercy’s level of functioning was that Mercy was living “unsupported for the past year.” If that statement is actually contained in Cruz’s reassessment, it is untrue. Karen, in fact, continued to support Mercy over the past year. The only difference between that period and the period prior to it is that Karen was not paid over the past year for caring for Mercy.
It appears that the DDS area office has mishandled this case from the start and has carried out what appears to be a vendetta against Mercy and Karen for having reported the alleged abuse against Mercy.
At the very least, we think, a properly constituted regional eligibility team that is independent of the DDS Worcester area office should assess Mercy’s functional level for shared-living services. DDS should then approve a realistic payment schedule to Karen for providing those services.
DDS hearing officer won’t allow COFAR blog post to be submitted as evidence in couple’s effort to place son at the Wrentham Center
A Department of Developmental Services (DDS) hearing officer has denied a couple’s request to submit a COFAR blog post to him for consideration as part of their appeal to place their son at the Wrentham Developmental Center.
The June 15 COFAR post claims, among other things, that federal law requires DDS to give individuals a choice of care in a facility such as the Wrentham Center. DDS primarily informs people looking for residential settings only of the existence of corporate provider-run group homes.
The couple, who have asked that their names not be used, requested that they be allowed to submit COFAR’s post in rebuttal to a DDS closing brief in the case. The DDS brief claimed that people with intellectual disabilities do not have a right to care at facilities such as Wrentham.
Last October, the couple appealed their son’s DDS Individual Support Plan (ISP) to the Department in an effort to have him placed at Wrentham. DDS held a hearing on the couple’s appeal on April 21 after the Department denied the requested placement. Under the ISP appeal regulations, the Department appointed a hearing officer in the couple’s case.
The hearing officer, William O’Connell, has not yet issued a decision on the appeal. His July 11 order denying consideration of the June 15 COFAR blog post stated that the post was submitted after his June 2 deadline for closing submissions in the case. However, O’Connell had previously extended that deadline to allow DDS to submit its closing brief on June 5.
Despite submitting its own brief under that extension, DDS subsequently opposed the couple’s request to have the COFAR rebuttal similarly entered into the record.
Hearing officer’s ruling is taken almost verbatim from DDS attorney’s objection
DDS’s written objection to the COFAR post described the post as “a late Rebuttal to the Department’s closing argument and brief,” and as “new evidence and argument that was not presented during the hearing or in the parties’ final closings.”
The DDS objection then stated that, “The (COFAR) evidence, a public opinion blog post, is of little probative value, and would likely not be admissible even if it were not filed late.”
Key portions of O’Connell’s written order about the COFAR blog post appear to have been taken almost word-for-word from DDS’s objection. O’Connell stated in his July 11 order that:
The (couple) submitted the rebuttal (COFAR post) well after the deadline for closing submissions had passed. Notwithstanding that the record was closed for evidentiary purposes at the close of the hearing on April 21, the proposed rebuttal to the DDS closing brief that the (couple) are attempting to submit as evidence and argument is a public opinion blog that is not probative and has no foundation for admissibility” (my emphasis).
Couple believes the hearing officer is biased against them
The couple maintain that O’Connell’s reliance in his order on the language in the DDS objection to the blog post appears to be evidence of a bias on his part in favor of DDS. They noted that he didn’t dispute any claim made in the post itself, but simply repeated DDS’s assertions about it.
The couple, who were not represented at the hearing by an attorney, also contended that O’Connell treated them with impatience during the April 21 hearing, and was deferential to DDS. “During the hearing, the hearing officer interrupted me several times and asked me to ‘get to the point,’” the wife said. “However, the DDS attorney was able to say her piece without interruption.”
The couple said they feel their case was “quite strong” at the hearing. But they said they are so certain their appeal will ultimately be denied by O’Connell that they are already planning their next move, which will be to take their case to state Superior Court to get their son into Wrentham.
If the couple are right about O’Connell’s likely decision, it will be interesting to see whether he primarily relies on the DDS closing brief in writing that decision, as he did with their request to submit our blog post into the record.
Unclear why DDS controls ISP appeal hearings
As noted above, DDS is in charge of the ISP appeal process, and even appoints the hearing officer who issues a recommended decision in each case. The final decision on the appeal is made by the DDS commissioner. We would agree that this creates, at best, a perception that the process is biased in favor of the Department.
We think the ISP appeal process should be decided by the independent Division of Administrative Law Appeals (DALA), which conducts appeal hearings for more than 20 state agencies, including the Disabled Persons Protection Commission (DPPC).
Hearing officer provided no support for claim that COFAR post was inadmissible
O’Connell stated that his order denying admission of the COFAR post was issued pursuant to the Massachusetts statute and regulations on adjudicatory practice and procedure (M.G.L. 30A and 801 CMR 1.02.)
We believe, however, that those rules would allow the post to be entered into the case record at any time, just as the DDS closing brief was entered after the hearing officer’s arbitrary closing date for submissions.
The regulations that O’Connell cited as underlying his ruling (801 CMR 1.02) constitute “informal rules” of adjudicatory procedure in Massachusetts.
Also, M.G.L.c. 30A, s. 11 states, with regard to the admissibility of evidence, that:
Unless otherwise provided by any law, agencies need not observe the rules of evidence observed by courts, but shall observe the rules of privilege recognized by law. Evidence may be admitted and given probative effect only if it is the kind of evidence on which reasonable persons are accustomed to rely in the conduct of serious affairs. Agencies may exclude unduly repetitious evidence, whether offered on direct examination or cross-examination of witnesses.
(3) Every party shall have the right to call and examine witnesses, to introduce exhibits, to cross-examine witnesses who testify, and to submit rebuttal evidence.
As we argue below, the COFAR blog post was intended to present evidence on which reasonable persons would rely in the conduct of serious affairs. It was not intended, as DDS and O’Connell casually dismissed it, to be a “public opinion blog.”
Both DDS and the hearing officer mischaracterized the nature of the COFAR blog post
As noted above, both DDS and O’Connell characterized the COFAR blog post as “a public opinion blog that is not probative and has no foundation for admissibility.”
However, the blog post directly rebutted the DDS assertion in its closing brief that federal law does not give persons with intellectual or developmental disabilities the right to placement at either the Wrentham Developmental Center or the Hogan Regional Center.
The post presented new evidence in the case regarding a succession of administrations in Massachusetts, which have allowed the residential population or census at the Wrentham and Hogan centers to decline. This decline, the post noted, has been due to DDS’s apparent policies of denying admission to those facilities to most persons who ask for it, and failing to inform persons looking for placements that those facilities exist as residential options.
We think the blog post therefore helped explain the almost automatic denial by DDS of the couple’s request to have their son placed at Wrentham.
Secondly, the blog post directly rebutted a statement in the DDS closing brief that the couple’s son currently lives in “a less restrictive community-based setting” than he would in an Intermediate Care Facility (ICF) such as the Wrentham Center.
The blog post then presented evidence that directly rebutted the DDS closing brief’s statement that the couple’s son “…has been successfully supported in the community for 13 years,” and that “he is well served by his community-based services and supports.”
Finally, the blog post revealed a misrepresentation in the DDS closing brief of the U.S. Supreme Court’s 1999 Olmstead v. L.C. decision with regard to institutional care. The post explained how the brief had wrongly implied that the Court had held that in all cases, individuals should be placed in community-based rather than institutional settings.
The statute that governs adjudicatory practice and procedure (M.G.L. c.30A, s.11), states that:
In all cases of delayed statement, or where subsequent amendment of the issues is necessary, sufficient time shall be allowed after full statement or amendment to afford all parties reasonable opportunity to prepare and present evidence and argument respecting the issues.
In our view, the couple were denied a reasonable opportunity to present evidence and argument in response to the evidence and argument in the DDS closing brief.
For all of the reasons discussed above, we believe the hearing officer erred in his denial of the couple’s request that the COFAR blog post be entered into evidence in their appeal.
Couple with disabled son who complained about second-hand cigarette smoke in their apartment are facing possible eviction
A couple that complained that second-hand cigarette smoke from another unit in their Kingston housing complex was harming the health of their disabled son are facing the possibility of eviction from their apartment.
Nicole and Cang Duong have accused the Alexan Kingston housing complex management and its attorneys of delaying their application for a state program that would help them keep up with their monthly rent.
As a result, Nicole Duong said, their RAFT rental assistance application expired on July 13, increasing their chance of eviction. They reapplied for the assistance on Monday (July 17).
The Duongs maintain that even though they took the proper steps to obtain rental assistance, they may still face eviction because of the application processing delay.
We reported on July 5 that the Duongs had complained to the management in May of a cigarette smoke odor that was coming from the air ducts in their apartment. Their 3-year-old son Caleb has Down Syndrome and severe obstructive sleep apnea. Cigarette smoke is particularly dangerous to his health, Nicole said.
Nicole said that while the housing complex management did subsequently inspect the ventilation system in their apartment and placed filters in the air ducts in response to their concerns, the management never sent anyone to their unit to investigate the origin of the alleged cigarette smoke. Yet, the complex has a strict no-smoking policy that applies to all areas, inside and outside.
In fact, the management suggested that the Duongs themselves should move out of the complex. The Duongs believe this is a violation of federal and state fair housing laws, which forbid discrimination against persons with disabilities.
Management’s lawyers allegedly “dragged their feet” in approving a rental payment plan
Nicole said she and her husband had been struggling to pay the rent on their apartment, and first applied for the RAFT assistance on June 7. She said that in compliance with the RAFT rules, they did not pay their June or July rent while the original RAFT application was being processed.
The Duongs’ monthly rent for their two-bedroom apartment, which is classified as an affordable rental unit, is $2,256.
Nicole said the approval of the RAFT assistance by the state Department of Housing depended on the family reaching agreement with the Alexan Kingston management by July 13 on a payment plan for two months’ worth of back rent.
Emails show that the Housing Department repeatedly asked Nicole earlier this month to provide a signed rental payment agreement under which the Duongs would pay $903 toward the overdue rent, and the RAFT program would pay the remainder of the $4,512 in back rent.
The first request from the Housing Department for the agreement was on July 6. An email from the Department to Nicole stated that the agreement must be submitted by July 13 “or your application process will be discontinued, and you will need to begin the application process again.”
Nicole said that while she provided the suggested RAFT agreement amount to the apartment management, the management turned the matter over to its law firm, and the law firm didn’t immediately respond. Emails show Nicole asked the apartment management and their attorneys for a copy of such an agreement on July 10 and July 11.
On July 10, the Alexan Kingston resident manager responded to Nicole, saying that he had contacted the management attorneys “to follow up on this item for us. I’ll touch base with them tomorrow as I know it’s very time sensitive.”
On July 11 at 4:53 p.m., still not having received a proposed agreement, Nicole emailed a member of the law firm, saying the RAFT application was scheduled to “time out” or expire two days later, and that a response from the management “needs to be done ASAP.”
The law firm finally sent an email with the proposed agreement to the Duongs at 7:10 p.m. on July 12, the day before the expiration of the original RAFT application. Nicole maintained that the law firm’s proposed agreement was unacceptable to them, but that it was too late in the day to contact either the management or the law firm about it.
Management’s proposed agreement included extra charges
Although the Duongs owed $4,512 in back rent, the law firm’s proposed agreement would require them to use their RAFT assistance to pay a total of $5,183, including $293 in “court costs” and $378 in “utilities/fees” as of next February 28.
Nicole contends there is no reason for her and her husband to pay court costs because the payment agreement should not require Housing Court involvement. In addition, she said, the utilities/fees cost was not explained in the proposed agreement.
The proposed agreement specified a periodic monthly payment schedule for the Duongs of $115 in addition to their monthly rent payments. The agreement stated that any late payments would constitute a material breach, which would allow eviction proceedings to begin in seven days. The Duongs would also waive their rights to an appeal or trial in the Housing Court.
Nicole said the proposed agreement would shorten the usual eviction notice period from 30 days to those seven days. She also said she and her husband would not want to sign away their right to take their case to the Housing Court.
Waiting for Section 8 placement since 2020
Even though their apartment is classified as affordable, the Duongs said they have been on a waiting list in Massachusetts for a Section 8 housing voucher since 2020.
Nicole said their rent constitutes 65% of their total income from her husband Cang’s job. She said her husband works overnight from 6 p.m. to 6 a.m., and that she needs to stay home to care for her son.
“I’m at the point of a nervous breakdown because I don’t want to lose our home,” she said.
We previously wrote to the housing complex management to urge them to fully investigate complaints from the Duongs and other residents of cigarette smoke odors in their apartments. We have now written them again to urge them to commit to reaching a timely payment agreement with the family that will cover their rental costs only.
We hope the apartment management will work to ensure that this family is not forced into homelessness.
We still need the subminimum wage and work opportunities in day programs for people with intellectual disabilities
We are hoping we can help the members of the Massachusetts congressional delegation understand the severity of the problem caused by the lack of meaningful employment opportunities for people with intellectual and developmental disabilities (I/DD) in this state.
On June 27, we held a Zoom meeting with an aide to Senator Elizabeth Warren to discuss that problem and the decline of the state’s two remaining Intermediate Care Facilities (ICFs) as options for residential services. That latter issue will be a subject for another blog post.
Among those attending was Jim Durkin, legislative director for AFSCME Council 93 in Boston. Also attending was Patty Garrity, whose brother Mark, is one of potentially thousands of clients of the Department of Developmental Services (DDS) who are facing a lack of meaningful work activities in their day programs.
Unfortunately, when it comes to providing employment for people with I/DD, most members of Congress appear to be heading in the wrong direction. For years, members of the state delegation have supported legislation that we think would effectively discourage such opportunities.
While Senator Warren, in particular, has been a strong voice for workers, she has also unfortunately been out front in mistakenly opposing the payment of subminimum wages to people with disabilities in congregate and other work settings.
We strongly support the payment of at least a $15-per-hour minimum wage to all persons, including disabled persons, who want to be paid that amount or more. We have, in fact, called for a minimum $25-an-hour wage for direct-care workers in the DDS system.
But what even many advocates for the disabled don’t realize is that there are some people with I/DD who don’t seek or choose payment of a minimum wage even though they do want to work. Those people cannot perform the level of work necessary in most mainstream job settings to receive a minimum wage; and therefore, they face the prospect of having no work at all if employers are not allowed to pay them a subminimum wage.
As Patty Garrity told Senator Warren’s aide in our Zoom meeting, the lack of viable work opportunities for Mark began after his then sheltered workshop was closed along with the rest of the remaining workshops in Massachusetts in 2016. Mark was one of thousands of people whose workshops became day programs, which no longer provided them with the piecework that they used to do.
Patty maintained that Mark had taken pride in that previous work. The fact that he wasn’t paid at the minimum wage rate was immaterial to him because he doesn’t understand the value of money.
“My brother lost out with the closure of his sheltered workshop, and he is continuing to lose out,” Patty said. “He’s not a minimum wage candidate. There is now a big gap in Mark’s life.”
Staffing shortage in day programs making the problem worse
That gap for Mark is only likely to get worse because of the ongoing staffing shortage in day and other programs funded by DDS. Many of these programs offer few activities of any kind.
Even the Arc of Massachusetts, a key proponent of the closures of the sheltered workshops, now acknowledges that the staffing shortage is a cause of a “systemic failure” in the DDS system in providing services. Maura Sullivan, a senior Mass Arc official, was quoted in April as saying:
There are thousands of adults with developmental disabilities that are not being served or we consider them underserved — very, very few services…
I think of it as really a systemic failure. And we’re really waking up to the fact that, you know, human services is a workforce that has been neglected in terms of rate increases.
As Sullivan acknowledged, the underpayment of staff is a key cause of the staffing shortage. It is not DDS clients who choose subminimum wages who are underpaid; rather it is their caregivers who should be paid more.
Two bills in Congress would promote work opportunities
We are urging members of the Massachusetts delegation to sign onto two bills, which would promote work opportunities for persons with I/DD. So far, no member of the Massachusetts congressional delegation has signed onto either bill.
Subminimum wage bill
The first bill (H.R.1296) would give an individual a choice whether to accept employment at a subminimum wage.
As Patty Garrity noted, her brother Mark cannot perform at the level most employers are looking for in providing a minimum wage. Patty maintains that it is also not Mark’s choice to work in an integrated environment.
We think an intellectually disabled client’s choice is key in this matter as it is in virtually all aspects of their care. In fact, DDS regulations state that programs and services are intended “to promote self determination and freedom of choice to the individual’s fullest capability…” (115 CMR 5.03) (my emphasis).
In seeking to eliminate subminimum wages, lawmakers would take away a choice for clients such as Mark in addition to taking away employment opportunities for them. Those lawmakers are effectively arguing that it is better for those clients to have nothing to do than to take a job that pays less than the minimum wage. Yet doing nothing all day long is clearly not Mark’s preference or choice.
Integrated employment bill
The second bill we are supporting (H.R. 553) states that a location in which an individual is able to interact with “colleagues, vendors, customers, and superiors…” would be considered to be a “competitive, integrated employment” setting.
This legislative proposal runs counter to a long-held but misinformed ideology that all persons with I/DD can successfully participate in employment activities alongside persons without cognitive disabilities. That ideology has also been a basis for the closures of sheltered workshops in Massachusetts and other states.
According to the ideology, the workshops were segregated settings because most or all of the participants generally had I/DD. That label, however, makes little sense in our view because most clients in sheltered workshops were there by choice.
Current federal law, which H.553 would change, states that an integrated employment location must be one in which the disabled employee “interacts with other persons who are not individuals with disabilities (not including supervisory personnel or individuals who are providing services to such employee)…” (my emphasis).
H.R. 553 would allow interactions with those supervisory personnel and service providers to count as integrated interactions.
The current federal law prevents work activities from being reintroduced to day programs because those settings are not considered to provide opportunities for competitive, integrated employment. As a result, people like Mark languish in them.
While we understand that the payment of a minimum wage stems from an important principle of social equity, we hope the members of our congressional delegation would agree that not all individuals will necessarily benefit from the universal implementation of every such principle.
Individual choice is also a principle of social equity. If it is possible to give individuals a choice among wage policies without harming others, it can be a win-win situation for all.
