Archive
It’s time to put a priority on state-operated care for the developmentally disabled
Here’s our letter to the Baker administration, asking them to put a priority on state-operated care for the developmentally disabled:
Kristen Lepore
Secretary
Executive Office of Administration and Finance
State House, Room 373
Boston MA, 02133 January 12, 2015
Dear Secretary Lepore:
We are writing to urge you to consider making the funding of state-operated care for the developmentally disabled a priority of the Baker administration.
For too long, state government has been divesting itself of its responsibility to provide care for the most vulnerable of its citizens, and has failed to adequately monitor and control the handover of human services to state-funded corporate providers.
The state’s priority has been to boost funding dramatically to corporate residential providers, in particular, while at the same time slowly starving state-operated care, including state-run group homes and developmental centers, of revenue. This has led to a gross imbalance in the Department of Developmental Services budget. The chart below depicts this imbalance.
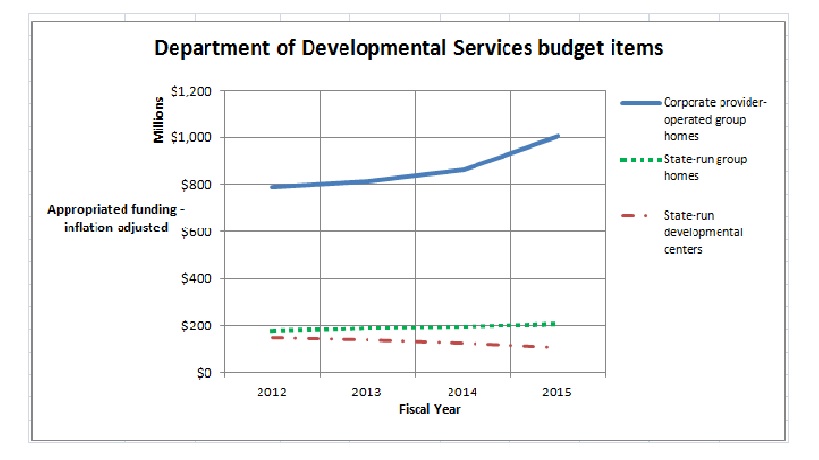
As the chart shows, funding to DDS corporate residential providers (line item 5920-2000) rose past the $1 billion mark for the first time in the current fiscal year. The line item was increased by more than $140 million –or more than 16 percent—over prior-year spending in FY 2015 dollars. At the same time, both the former governor’s and the legislative budgets either cut or provided much more meager increases for most other DDS line items.
The state-run developmental center line item (5930-1000) was cut in the current fiscal year by more than 13 percent in inflation-adjusted dollars, while the state-operated group home line item (5920-2010) was raised by less than 7 percent.
We have calculated that if the increase in the provider residential line item had been reduced by just 2.1 percent – to a 14.7 percent increase – as much as $18 million could have been redirected to the state-operated group homes, DDS service coordinators, the Autism Division, Turning 22 program, Respite and Family Supports, and the remaining developmental centers in the state.
But the previous administration was not satisfied even with a $140 million increase in funding for the corporate provider line item. In late November, despite a projected $329 million budget deficit in the current fiscal year, the Patrick administration proposed a supplemental budget increase of $42 million in the provider residential line item. While the administration made more than $200 million in emergency “9C” cuts and proposed additional cuts to address the projected deficit, it included the $42 million in proposed supplemental funding for the DDS corporate residential line item in the same bill (H. 4536) proposing mid-year cuts in local aid and other accounts.
In addition to the erosion of critical state-funded care, the state’s priority of boosting funding to corporate providers has created a poorly monitored system of DDS contractors that has financially benefited provider executives. Our own survey of the DDS provider system has shown that the state has provided between $80 million and $90 million a year to a bureaucratic layer of corporate CEO’s, vice presidents, executive directors, and other executives. At the same time, wages of direct-care workers in provider residences have been flat or have declined in recent years.
State-operated group homes and developmental centers
We believe the misplaced priority on funding of corporate providers ignores the wishes of family members and guardians around the state for more choice and availability in state-operated care. DDS data show that close to 42 percent of the 372 individuals moved out of developmental centers in the state since 2008 were placed in state-operated group homes. Another 45 percent of those residents were transferred, at the request of their families, to remaining developmental centers. Just 13 percent of those individuals went to provider-run group homes.
Yet, since 2008, 157 new provider-operated group homes have been built in the state, according to information provided by DDS. In that time, only 38 new state-operated group homes have been built, and three have been closed or converted to provider-operated homes. DDS has projected that it will build an additional six state-operated group homes, but will close or convert five state-operated facilities to provider residences.
Additional funding is needed for the state-operated group home system to preserve it as a choice for people waiting for residential care in the DDS system.
State-operated developmental centers
As a result of class-action lawsuits dating back to the 1970’s, the State of Massachusetts dramatically improved care in its state-run developmental centers, bringing them to a world-class level of care with dedicated, highly-trained staff. But starting in 2003, the Romney administration and subsequently the Patrick administration began efforts to close the state’s then six remaining developmental centers.
Starting in 2008, the Patrick administration stepped up the closure efforts and shut the Monson, Glavin, Templeton, and Fernald Developmental Centers, in many cases over the strong objections of families and advocates of the residents there. And despite the demonstrated desire of families and guardians for the intensive and high-quality care that the developmental centers provide to the most profoundly developmentally disabled, the developmental center line item has been cut repeatedly since 2008. The current-year DDS budget cut the developmental center line item by more than 13 percent in the current fiscal year alone, as noted.
We hope the Baker administration will consider restoring balance to DDS budget accounts by increasing funding to the developmental center and state-operated group home line items. State-operated care continues to be better monitored than provider operated care; and training as well as pay and benefits provided to staff in state-run facilities continue to be higher than in provider-run residences.
Ultimately, only government is in a position to respond directly to the public interest and to the wishes of families and guardians of the most vulnerable people among us. Federal law recognizes that fact by designating families as the “primary decision makers” in the care of individuals with developmental disabilities [(42 U.S.C. §2001(c)(3)].
Thank you for your consideration.
Sincerely,
Colleen M. Lutkevich Thomas J. Frain, Esq. Edward Orzechowski
Executive Director President President, Advocacy Network
When Big Brother (thinks he) knows best about the developmentally disabled
It can be frustrating when government administrators take it upon themselves to tell citizens what is in their best interest, and that includes telling them what is in the best interest of their family members with developmental disabilities.
It’s particularly frustrating when the state and federal governments tell people that they know best where their family members should or should not live.
For instance, the folks at the federal Centers for Medicare and Medicaid Services (CMS) have determined that farm-based residential programs are not good for developmentally disabled people. Also bad are residential schools for the developmentally disabled, group homes on the grounds of a private developmental or Intermediate Care Facility (ICF), and group homes located in “close proximity” to each other.
Both CMS and the Massachusetts Department of Developmental Services have decided that all of those types of residential settings “isolate” the participants from the “broader community.” But while the feds are not banning those particular settings outright, the state DDS, in a new policy, appears to be proposing to do just that. According to the DDS policy, residents of “noncompliant programs” will be given “the opportunity to move to a compliant setting” or else face possible dis-enrollment from the HCBS program.
It doesn’t appear to matter that the participants may greatly enjoy living on a farm, for instance, or that they may derive many important skills from farm programs that improve their self-care, receptive and expressive language, learning, mobility, self-direction, and capacity for independent living. It doesn’t matter either that their families and guardians may value those skills highly and consequently value those programs themselves.
It also doesn’t appear to matter that thousands of people in Massachusetts are waiting for residential and other care options, and that eliminating potential options, as CMS and DDS are doing, is only going to make that situation worse.
CMS issued a new regulation earlier this year that states that the residential settings they have identified as isolating may not qualify for Medicaid funding that is specifically earmarked for “home and community-based services.” In “guidance” provided on the regulation, CMS criticized residential farm programs, in particular, because “an individual generally does not leave the farm to access HCBS (Home and Community Based Services) or participate in community activities.” CMS said similar things in the guidance document about residential schools for people with developmental disabilities, and about other programs that “provide multiple types of services and activities on-site.”
In its new policy based on the CMS regulation, DDS states that it will not fund or support new residential settings such as farmsteads, “gated or secured communities,” residential schools, settings that “congregate a large number of people with disabilities for significant shared programming and staff,” or even new group homes with more than five residents.
DDS has scheduled public forums on its policy and a “transition plan” to comply with the CMS regulation on November 6 at 6 p.m. at Massachusetts Bay Community College in Wellesley, and November 12 at 10:30 a.m. at Westfield State University in Westfield.
It is not clear what evidence CMS has to make the claims that people in farm-based and other congregate care programs are not provided with access to community activities. The federal agency’s guidance offers no citations or backup information or studies to support its claims.
Moreover, even if it were true that on most residential farms and in other programs providing “multiple services” that the residents are not regularly taken into the community, wouldn’t it make more sense to require that those programs periodically take participants into the community than to effectively ban the programs altogether? Isn’t that throwing the baby out with the bath water? CMS acknowledged that it received many comments about how valuable and therapeutic those farm programs, in particular, are.
By the same token, CMS appears to be ignoring evidence that there is often little or no community integration by residents of small group homes. Yet, even CMS isn’t willing to prohibit Medicaid funding for farm programs, residential schools, or multiple group home settings outright. In contrast to the Massachusetts DDS, CMS has stated that it will subject so-called isolating programs to “heightened scrutiny,” which may result in continuing to fund them if a state makes the case that the settings do not have institutional qualities.
CMS, in fact, specifically rejected the idea of banning group homes with more than a set number of residents. In responses posted on the Federal Register to public comments on the proposed regulation, CMS stated that it had previously proposed defining institutional care based on the number of residents living in a facility, but that:
…we were persuaded by public comments that this was not a useful or appropriate way to differentiate between institutional and home and community-based care. As a result, we have now determined not to include or exclude specific kinds of facilities from qualifying as HCBS (home and community based services) settings based on the number of residents in that facility (my emphasis).
CMS also noted on the same Federal Register site that the goal of its new Medicaid regulation:
… is not to take services from individuals, or make individuals move from a location where they have always lived… The goal of this regulation is to widen the door of opportunity for individuals receiving Medicaid HCBS… to have a choice in how, when, and where they receive services; and to remove unnecessary barriers and controls. (My emphasis).
So CMS states that its goal is to give people choices and NOT to make people move from a location where they have always lived; but the Massachusetts DDS has made it their goal since the Patrick administration came into office to move people away from where they’ve always lived. It’s evident from the language of the DDS policy and from DDS’s own actions over the past several years that the choices of individuals and their families and guardians do not signify here. For instance, only corporate provider-run settings are routinely offered by DDS as options for people seeking residential care.
Yet while the Massachusetts DDS is going beyond what CMS apparently intended in moving to eliminate available options for residential care, CMS has given the states the latitude to do so. As Tamie Hopp of the VOR, a national advocacy organization for the developmentally disabled, noted, states have “incredible discretion in terms of how they operate their Medicaid programs.”
In a publication, VOR contends that the new CMS regulation “continues to demonstrate an ideological bias against disabled people who find friendships and benefits from living together and accessing services and amenities ‘under one roof.'” VOR further suggests that:
…if CMS determines some settings to be too ‘institutional’… it is likely that states will realize higher costs to accommodate transitions to likely smaller, scattered settings where economies of scale will not be realized. Quality of care and access to specialized services may also be affected, exacting an untold cost on affected individuals.
For some, this is really all about cutting Medicaid programs and diverting Medicaid funding to corporate providers, who are being encouraged to operate more and more widely dispersed, and smaller, group homes. The corporate providers in Massachusetts are apparently fine with all of this. In fact, DDS notes in its transition plan that it consulted with “a small stakeholder group (including providers, advocates and participants/family members).” The usual advisors to DDS are listed in the transition plan, including the Arc of Massachusetts and The Association of Developmental Disability Providers (ADDP).
It may just be that the people who are truly isolated in institutions are the folks working at CMS and the Massachusetts DDS, who appear to have little idea of how things work in the real world. Someone needs free them from their ivory towers!
You can help by sending your comments on DDS’s policy to their email address at HCBSWaivers@MassMail.State.MA.US. You can also write to: HCBS Waiver Unit, 1 Ashburton Place, 11th Floor, Boston, MA 02108. Comments must be submitted by November 15.
Why we won’t be at the bill signing at Fenway Park
Tomorrow, Governor Patrick will be at Fenway Park for the ceremonial signing of three pieces of legislation that are intended to make major changes in the care and services for the developmentally disabled in Massachusetts.
Many advocates will be there, but many if not most of those in attendance will be corporate providers to the Department of Developmental Services, who played key lobbying roles in the drafting of each piece of legislation last spring. As a result, as we have pointed out, each of these new laws (because Patrick signed them for real in August) is flawed in a major way.
There really is no reason to celebrate unless and until changes are made in the laws, so we won’t be at the event tomorrow. In a nutshell, here are the problems with the laws:
1. National Background Check law: The law authorizes national criminal background checks for persons hired to work in an unsupervised capacity with persons with developmental disabilities. It will ultimately require that both current and prospective caregivers in the DDS system submit their fingerprints to a federal database maintained by the FBI. Those requirements are long overdue, but they will be further delayed under the new law.
The fingerprint requirements will not be phased in under the law for all current employees in the system until January 2019, and will not take effect for new employees until January 2016. Another provision in the new law that raises questions appears to allow employees to be hired before the results of their background checks are obtained.
COFAR and the VOR, a national advocacy group for the developmentally disabled, sent a joint message to lawmakers this week that states: “Much harm can be done to vulnerable people due to the delayed implementation and the ambiguous language that we hope was not the intent of the Legislature.”
When COFAR contacted the Legislature’s Judiciary Committee last summer to ask why the committee had approved the delays and the ambiguous provision in the new law’s requirements, a staff member referred us to Johnston Associates, a Beacon Hill lobbying firm. A member of the firm said providers and some other advocates had pushed for the delays. No one could or would give us an answer as to why language was inserted that appears to allow the hiring of employees before their background checks are done.
2. The ‘Real Lives’ law: This legislation had been pushed for years on Beacon Hill by the providers. The stated intent of the measure is to introduce “person-centered planning” into the DDS care system by allowing each DDS client to “direct the decision-making process” and manage their own “individual budgets” for care.
In the wake of criticism earlier this year from COFAR, legislators removed a provision from the bill, which would have named the Association of Developmental Disabilities Providers and the Arc of Massachusetts to a board that would advise DDS in developing the person-centered planning system. Another provision that was thankfully removed would have established a “contingency fund” to compensate providers that lose funding when clients move out of their residential facilities.
But the new law still raises a number of concerns, including providing what appears to be only a limited role for guardians and family members in the person-centered planning process. The law also introduces a central role in the process for vaguely defined “financial management services” and other privately run entities.
In a joint statement this week, the VOR and COFAR called on legislators to “ensure that vulnerable individuals with intellectual and developmental disabilities have the support of legal guardians, when appointed, rather than financial managers or independent facilitators” in undertaking person-centered planning.
The joint statement also urged legislators to add a provision to the law ensuring that persons seeking DDS services would have an explicit choice among a range of care options and settings, including state-operated facilities and group homes, provider-operated homes, shared living arrangements, and home-based care. State-operated care is often not presented as an option to people seeking DDS residential services. Those persons are instead presented only with the option of corporate provider-operated residential care.
3. The DDS eligibility expansion law: This legislation is intended to fill a major gap in DDS care in Massachusetts by extending eligibility for services to people with autism and two other specified disabilities known as Prader-Willi Syndrome and Smith-Magenis Syndrome.
Until the enactment of this law, DDS had restricted eligibility for DDS services to people with “intellectual disabilities,” as measured by a score of approximately 70 or below on an IQ test. That left out many people with developmental disabilities, including autism, even though those conditions may severely restrict an individual’s ability to function successfully in society. If those people score higher than 70 on an IQ test, they are routinely denied services.
However, in specifying three developmental disabilities that make individuals eligible for DDS services, the new law necessarily leaves out other conditions that often result in many of the same types of functional limitations, such as Williams Syndrome, spina bifida, and cerebral palsy. The new law was the product of closed-door negotiations among legislators, administration officials, and selected advocacy organizations.
In addition to changing that eligibility standard, the new law establishes a permanent new autism commission and authorizes the establishment of tax-free, individual savings accounts to pay for a variety of DDS and other services. The commission will consist of 35 members, including legislators, administration officials, the Arc of Massachusetts, and advocates from autism advocacy organizations. There are no seats on the commission for any advocates of state-run care for the developmentally disabled.
The VOR and COFAR urged legislators this week to make changes in the law “to better identify and serve eligible individuals in need of services and supports.”
In sum, while these new laws have many well-intentioned supporters, major changes are needed in each piece of legislation to enable it to fulfill its purpose and prevent it from doing more harm than good. It is not yet time for everyone to pat themselves on the back as will no doubt be happening tomorrow at Fenway Park.
Heavily redacted state reports raise more questions than answers in sudden deaths of DDS clients
More than three years after the sudden death of a former resident of the Templeton Developmental Center, we have received a report on the matter from the state Disabled Persons Protection Commission, which found that the resident had adequate care and services at the time of his death and that there was no evidence he had been neglected or abused.
But the report is so heavily redacted that it is difficult to determine whether a number of specific questions and allegations that had been raised about the person’s care were actually investigated. It is also unclear why it took nearly two years for the DPPC to provide us with the report, which was completed and approved by a supervisor in the agency in November 2012.
The former Templeton Center resident died on July 24, 2011, four days after he was transferred to a state-operated group home in Tewksbury. The cause of death was reportedly a blood clot in his lung.
This was one of three cases we heard about in 2011 and 2012 in which clients of the Department of Developmental Services, each of whom happened to be a man in his 50’s, died suddenly after being transferred from developmental centers to state-run group homes operated by Northeast Residential Services, a division of DDS. A second case was that of a former resident of the Fernald Developmental Center, who died on July 6, 2011, after having ingested a plastic bag in a Northeast Residential Services group home in which he was living in Tyngsborough.
In that second case, a DPPC report concluded that there was a lack of adequate supervision of the man by his caregivers, although the investigative agency was unable to determine whether the man had ingested the plastic bag while he was in the group home or his day program or was being transported between the two. That report was also so heavily redacted that it left numerous questions about the incident unanswered for us, including whether the man’s care plan may have been significantly changed after he left the Fernald Center.
In a third case, a 51-year-old resident of a Northeast Residential Services home in Chelmsford died of acute respiratory failure on February 7, 2012, after having been sent back to his residence twice by Lowell General Hospital. That man had formerly lived at the Fernald Center as well. We have just requested that report from the DPPC.
While it is of course disturbing that three DDS clients would die suddenly in a relatively short span of time in the same regional group home system, we have no information to indicate that staff in any of the Northeast Residential Services homes were at fault in any of the deaths. These cases may in fact raise more questions about the DPPC’s investigation and reporting procedures than they do about care in DDS-run group homes.
In the case of the man who died of a blood clot four days after leaving Templeton, we raised questions at the time whether the stress of the move may have contributed to his death, or whether there was a medication error or other care issue involved. It was also unclear whether staff familiar to the man while he was at Templeton was available to accompany him to his new residence in Tewksbury. Moreover, we noted that DDS may not have had uniform policies or procedures in place as to whether familiar staff should accompany transferred residents to their new locations.
The DPPC report found that the man had direct-care staff available 24 hours a day and nursing staff “as needed” in his group home, and that there was no evidence that any medication error had occurred.
I have written to the DPPC to ask why it took so long to release the report on the former Templeton resident’s death. I had requested a copy of the report by letter on October 31, 2011. The report is dated as having been completed on November 1, 2012, and as having been approved by a DPPC supervisor that same day. It was mailed to us with a cover letter, dated September 17, 2014.
In contrast, the report on the July 2011 death of the former Fernald resident who ingested the plastic bag, while also heavily redacted, was dated March 29, 2012, and provided to us in May of 2012.
The former Templeton resident’s guardian, who was also his niece, told me after his death in July 2011 that her uncle had had a blood clot in his leg about a year before the move from Templeton (deep venous thrombosis), but the problem had been cleared up. She said he had been put on a blood thinner called Coumadin, but that she later found out that he was taken off that medication while he was still at Templeton. She said she was never consulted about the decision to take him off the medication. The guardian said that other than the instance of thrombosis, her uncle had only minor health problems. He had worked every day in the dairy barn at Templeton.
While most of the discussion in the DPPC report on the issue of the former Templeton resident’s medication appears to have been redacted, there was a statement in the report that “all necessary medications were continued,” and that a review of documentation from July 19 through the day of his death on July 24, 2011, “indicates no medication error occurred.” Due to the redactions, however, it could not be determined from the report which medications the DPPC considered to be necessary. There was no mention in the unredacted portions of the report of any allegation that the Coumadin had been discontinued.
The guardian had also told me the staff from the group home had spent about a week at Templeton with her uncle prior to the move, but she was not sure whether any familiar staff from Templeton accompanied him during the actual transfer to the new residence. The unredacted portions of the DPPC report were not clear concerning this potential allegation either.
According to the DPPC report, the man’s move from Templeton to the Northeast Residential group home had been planned, and staff from both facilities attended the planning meetings. The resident was actively involved in choosing the new residence and visited it along with familiar staff and family prior to moving there, the report stated.
In discussing the circumstances of the man’s death, the DPPC report stated that he had left his bedroom at 9:15 on the morning of July 24, 2011, and had indicated he was not feeling well. Three staff members responded immediately. The man became short of breath and then unresponsive, so CPR was initiated immediately and 911 was called. CPR was continued until the arrival of paramedics, who continued it while the man was transported to a hospital by ambulance. He was pronounced dead at 9:47 a.m.
The March 29 DPPC report on the death of the man who ingested the plastic bag also leaves many questions unanswered about his care, including whether the man’s Individual Support Plan (ISP) had been changed in a significant way after he left the Fernald Center, and whether his level of supervision in the group home was less than the level he had received while at Fernald. There is an indication in the report that the man’s ISP was changed in September 2010, apparently after he moved to the group home, to remove “target (presumably inedible) items” from mention in the plan. Much of this discussion, however, was redacted in the report.
The man reportedly had a history of ingesting foreign objects, a condition known as pica. However, even what was apparently the word “pica” was redacted throughout the report.
It is understandable that public health and human service agencies have a desire to protect the privacy of individuals in their care or their jurisdiction. But it often seems that the desire to redact or withhold information goes much farther than necessary and fails to protect the public’s right to know about these cases. In our view, the two DPPC reports discussed here fall into that latter category. We believe much of the redacted information in both cases could have been made public without compromising either of these individuals’ privacy in any way.
The questions raised about the care and services that were investigated in these cases are important ones. Something seems to be wrong when investigative and other agencies withhold key facts about cases like these and end up being the only ones who know those facts.
DDS policy will disperse people and care
A new Patrick administration policy statement on care and services for people with developmental disabilities states that its intention is to enable people to lead “fully integrated lives” in the community.
But the statement, which was issued on September 2 by the Department of Developmental Services, would appear to take us further down a path of dispersal and isolation of people in the DDS system.
Among other provisions, the policy states that DDS will limit the number of people living in new group homes to five or fewer. Individuals who continue to live in “non-compliant” residences could be dis-enrolled from the Department’s Medicaid-funded programs, the policy states.
In setting the five-person limit, the policy goes even further than a new Obama administration regulation on Medicaid-funded, community-based care on which the state policy is supposedly based. The Massachusetts policy even bans new programs that provide farm-based residential care to people with developmental disabilities, and further appears to ban new residential programs that provide recreation or other programs to groups of disabled people.
All of those programs and services are apparently too “institutional” for the Patrick administration, which apparently believes that any setting that serves more than five disabled people automatically “isolates them from the broader community.”
Massachusetts DDS Commissioner Elin Howe signed the policy, which states that it is based on the new federal rule issued by the Centers for Medicare and Medicaid Services (CMS), which sets new standards for providing Medicaid funding to community-based providers. But while the Massachusetts policy is supposedly based on the CMS rule, the CMS specifically rejected a proposal to specify the number of people who are allowed to live in community-based facilities.
In responses to comments about its proposed rules, the CMS stated that while they initially proposed a limit on the number of people who can live in group homes and still qualify for Medicaid funding, they were persuaded by public comments that “this was not a useful or appropriate way to differentiate between institutional and home and community based care.”
The DDS policy is not as draconian as that of the highly ideological National Council on Disability, which has determined that any facility housing four or more people is “institutional” in nature and should be shut down. Nevertheless, one has to ask why the Patrick administration would set a limit on the number of people who can live in new group homes when even the federal administration, which strongly favors community-based care, has determined that such a limit is not useful or appropriate.
As was the case with sheltered workshops, the Patrick administration has shown itself to be more ideologically opposed to state-run and congregate care than the federal government. It seems to us DDS’s policies on sheltered workshops and community-based care will only further disperse people and services, and ironically, further isolate them. While advocates of deinstitutionalization have long argued that community-based care is intended to reduce isolation, the opposite appears to be occurring.
Other troubling aspects of the new DDS policy on community-based care stem from its statement that DDS will not license, fund or support new residential settings with “characteristics that isolate individuals from the broader community.” That’s fine in itself, but the policy goes on to say that those isolating characteristics are to be found in:
- “Settings that have limited, if any, interaction with the broader community.”
But what does limited interaction mean and who judges it? The policy doesn’t define this. In fact, we often hear complaints from family members and guardians that small group homes provide for virtually no interaction with the broader community. In this sense, we have always considered that larger, congregate facilities provide more of a sense of community, almost by definition, than do many group homes.
- “Settings that use or authorize restrictions that are used in institutional settings.”
What restrictions? The policy gives no further information on this.
- “Farmsteads or disability-specific farm community (sic).”
Why the ban on farmsteads? Farm-based programs have been found to be highly conducive to treatment and well-being of developmentally disabled individuals. Last year, I wrote a post on the SAGE Foundation blogsite about three successful farm-based programs, each of which provides a range of treatment, crafts, and other programs and services to people with either developmental disabilities or mental illness. Many of these farm programs were founded by parents frustrated by the lack of services available to people with autism, in particular.
- “Gated or secured communities for people with disabilities.”
The DDS policy provides no further information on this.
- “Settings that are part of or adjacent to a residential school.”
This provision is a troublesome aspect as well of the CMS rule. How does being adjacent to a residential school somehow makes a residential setting institutional?
- “Multiple settings co-located and operationally-related that congregate a large number of people with disabilities for significant shared programming and staff.”
This appears to limit many potentially effective programs and ideas. I’ve written about two of these ideas to develop residential services and programs for a larger number of people in both community and developmental-center settings. Given the large number of people waiting for care and services in Massachusetts and other states, it makes sense to consider these proposals.
DDS should be looking, as noted, at ways to serve people who are waiting for care. As the Massachusetts Developmental Disabilities Council pointed out in its 2014 state plan, Massachusetts is lagging behind other states in funding and providing care and services for people with developmental disabilities.
The Developmental Disabilities Council described “limited options due to a lack of adequate resources” for adults entering the DDS system. In light of all of that, we fail to understand why the Patrick administration has issued a policy that will only further limit options available to people with developmental disabilities.
Why the Fernald land deal should include a plan for the developmentally disabled
The history of what is now known as the Fernald Developmental Center hasn’t been free of some serious blemishes or controversy. But from 1889 to the present time, Fernald’s 200-acre campus in Waltham has been the site of a facility providing residential care for persons with intellectual disabilities.
That’s all about to change permanently.
Under legislation negotiated among representatives of the Patrick administration, the City of Waltham, and local legislators, the state will sell the campus to the city for $3.7 million, which comes to 18,500 per acre — a price that has been described as “dirt cheap.” It appears there is also a requirement that the city pay the state up to half the proceeds from the re-sale of any of that land to developers.
There is just one group of people that seems to have been left out of the plans and negotiations. That group is the developmentally disabled — the very persons who had been living at Fernald all along. Other than keeping the therapeutic swimming pool open at Fernald and maintaining a 29-bed nursing home on the campus, there appear to be no plans to continue to provide care or services at the Fernald site for persons with disabilities who live in the surrounding community.
This is an unfortunate oversight, not only for the residents who have been forced to leave Fernald, but for developmentally disabled people in the community. As I’ll explain, the lack of a plan for integrated, community-based care at the Fernald site has been, and will continue to be, both a missed opportunity to help those waiting for services and a potential waste of taxpayer money.
First, I would note that the Fernald Working Group, a coalition of local organizations, had recommended that a portion of the campus remain the site of residential care and services for the intellectually disabled. Similar proposals have been made over the years by the former Fernald League and COFAR. Both of those latter groups suggested a “postage-stamp” arrangement under which existing residents would live in housing situated in a small area of the campus while the rest of the campus was converted to other uses. And Waltham Mayor Jeannette McCarthy, the chair of a Fernald Reuse Committee, also publicly supported the continued use of part of the campus for institutional, residential and health care.
But the then Romney and subsequent Patrick administrations were interested only in one thing — closing Fernald and three other developmental centers in the state, contending the state would save tens of millions of dollars a year in doing so. They never considered any of the proposed alternatives to the closures, and have never done what administrations in other states have done, which is to propose the integration of congregate care facilities for the developmentally disabled with their surrounding communities.
The result is that since 2008, two of six remaining developmental centers in Massachusetts have been closed; a third center is being converted to state-run group homes, and just two residents of the Fernald Center remain on the campus out of a total of 160 who were there at that time. Most of the residents living in the four facilities targeted for closure were dispersed around the state, with the majority going either to state-operated group homes or to the Wrentham Developmental Center. Why has all of this been a missed opportunity and a potential waste of taxpayer money?
First, with regard to the cost to taxpayers, the administration projected that Fernald would be closed by July 2010, but the closure was blocked for four years by administrative and court appeals filed by guardians on behalf of some 20 remaining residents there. The administration elected to keep Fernald open only for the remaining residents there, pending resolution of their administrative and court appeals. This turned out to be an extremely inefficient way to proceed.
Not only has there been an undisclosed cost to the state in fighting the legal battle to close Fernald over the past decade, but as the population dwindled in all four targeted facilities, the cost per resident of care there shot up due to fixed costs such as heating and other utilities in larger buildings. This was particularly true for Fernald, which has remained open for more than four years with 20 or fewer residents.
The administration could have saved millions of dollars a year since 2010 had it been willing to consider and negotiate an alternative to outright closures of the facilities. The legal battle over Fernald would have ended immediately, and instead of continuing to house the remaining residents in several locations on campus, the state could have built small, cost-efficient housing in one location for the residents. That proposed alternative to closure has rarely if ever been reported on by the media, which has instead adopted the position of the administration and its corporate providers that the high cost of continuing to operate Fernald has been solely the fault of the residents remaining there.
Moreover, dozens of the Former Fernald residents were sent, as noted, to the Wrentham Center, which amounted to transferring residents from one developmental center to another. Not only was there no real savings in doing this, but the administration was forced to undertake renovations at Wrentham in order to accommodate the former Fernald residents — a project that cost taxpayers at least $3.2 million.
There is a second, and potentially greater, cost to taxpayers in closing Fernald and the other developmental centers without planning for any continuation of care at those sites that could be integrated with their surrounding communities. As we have noted, an undisclosed number of developmentally disabled people throughout the state have been unable to access services or care from DDS due to a lack of resources. The state has tried to address this problem by expanding the provider-run residential system, which has involved building more than 150 group homes spread around the state since 2008 and substantially increasing rates paid to the providers.
But there is no centralized system of care in the provider-run system. People have to be transported to day programs and for medical and other types of care — a process that is potentially much more expensive than if all of this care were available in centralized locations. Continuing to provide centralized care at developmental center sites could both allow more people in the surrounding community to receive services and provide those services more cost-effectively than is the case in a system consisting almost entirely of disbursed group homes.
We have also pointed out the potentially high cost of privatized care in Massachusetts and elsewhere due to the thick layer of highly paid corporate executives in that system.
That there isn’t necessarily a long-term savings in transferring people from developmental centers to decentralized, provider-based care has been acknowledged even by one of the leading proponents of deinstitutionalization in the Obama administration. I’ve blogged about a law journal article written by Samuel Bagenstos, a former top litigator in the Justice Department’s Civil Rights Division, in which Bagenstos stated that any cost savings in closing developmental centers “will shrink as people in the community receive more services.” He added that a significant part of the cost difference between institutional and provider-based care “reflects differences in the wages paid to workers in institutional and community settings — differences…that states will face increasing pressures to narrow.”
All of this is why we supported the vision of the Fernald Working Group, which described “a progressive site at Fernald where open space and greenways can be matched with an equal vision of integration for individuals with disabilities.” That vision encompassed both existing residents and disabled persons in the surrounding community. The Working Group specified that this vision included new housing and the preservation of the therapeutic pool and gym at Fernald as well as the chapel and programs for physical therapy, dental and medical services. As the vision statement noted, “all of these services could become part of the community and economic life of the Fernald redevelopment.”
But as far as we can tell, the Working Group’s vision has not been adopted by either the administration or the Legislature. While the newly signed legislation to sell the Fernald land to the city provides incentives for adopting “smart growth principles” and affordable housing in the development of the site, it makes no mention of continued services or care for persons with developmental disabilities.
Last week, I emailed Senator Michael Barrett and Representatives Tom Stanley and John Lawn, the key sponsors of the land sale legislation, to ask whether the continued use of a portion of the Fernald campus for individuals with disabilities was considered in the negotiations over the bill and whether any provisions for that might be made in the future.
A staffer in Barrett’s office said that no proposals to serve the developmentally disabled at Fernald were made at a public hearing on the land sale bill that was held in July by the Legislature’s State Administration Committee, and the idea was therefore not considered. But while the Village at Fernald concept for the disabled may not have been raised at a public hearing earlier this summer, most, if not all, of the negotiating parties to the legislation have long been aware of that concept. It should have been a part of the legislation from the beginning.
Federal agencies ignore realities of care of the developmentally disabled
Some agencies within the Obama administration have an ideological bias against congregate care for the developmentally disabled that has apparently blinded them to the damage done to countless lives in the name of deinstitutionalization.
That bias, which is held as well by the Patrick administration in Massachusetts, is on display in an article written by a key former Obama administration official about the deinstitutionalization movement from the 1960’s to the present.
The article is by Samuel Bagenstos, former principal deputy assistant attorney general in the Obama Justice Department’s Civil Rights Division and a key litigator in deinstitutionalization cases.
Bagenstos acknowledges in the article, published in the Cardozo Law Review, that the past and pending closures of institutions such as the Fernald Developmental Center in Massachusetts have not resulted in adequate funding for community-based care. But Bagenstos declines to acknowledge the role his own former agency has played in the often checkered expansion of the largely privatized community system that followed the closures of state-run Intermediate Care Level facilities for individuals with intellectual and developmental disabilities (ICFs/IID).
Instead, he argues that if only families of developmentally disabled individuals see fit to team up with advocates of further deinstitutionalization, they can work together somehow to ensure that care will be adequate in the community. We aren’t buying it, and the VOR, our national affiliate, isn’t buying it either.
In a response to Bagenstos’s article, the VOR contends that:
Bagenstos shows no willingness to take responsibility for the tragedies that he and the other advocates caused to these highly vulnerable individuals. Nor have past failures moved Bagenstos to take a more reasoned approach to deinstitutionalization efforts, one that insists on building quality, community placements and adequate oversight before displacing fragile individuals from ICFs/IID.
Instead, closure advocates are turning to new “battlegrounds” (private facilities, nursing homes and adult care homes), without apparent concern for the hundreds of thousands of individuals on waiting lists for community services or the history of abuse, neglect and death that has befallen countless community-based individuals.
In an article this month in The Nonprofit Quarterly, Tamie Hopp, VOR’s director of government relations and advocacy, adds that among the results over the past 30 years of deinstitutionalization of the developmentally disabled are waiting lists in states for residential care that now number nearly 317,000 people, emergency rooms that “have become de facto urgent care clinics” for developmentally disabled people, and correctional facilities that are “replacement treatment centers” for some individuals who have both mental illness and developmental disabilities.
As Hopp points out, U.S. Senator Chris Murphy (D-CT) has called for a U.S. Department of Health and Human Services Office of Inspector General investigation to “focus on the prevalence of preventable deaths at privately run group homes across this nation and the widespread privatization of our delivery system.” The VOR has catalogued hundreds of media reports of abuse and neglect in privatized group homes around the country in recent years.
Yet key current and former officials in the Obama administration seem oblivious to all of this, and so does the Patrick administration in this state. As we have noted, the Obama administration’s National Council on Disabilities (NCD) now labels any facility with four or more residents an “institution,” and has called for the closure of all such facilities. The NCD does not appear to have put any thought into what would replace the care provided in those settings.
Meanwhile, the federal Centers for Medicare and Medicaid Services (CMS) has written new regulations to terminate Medicaid funding for any facilities that happen to be located on the grounds of state-run or private ICFs/IID or even near to them. And just this past week, President Obama signed a bill into law limiting placements for people in sheltered workshops, which the CMS considers to be inappropriate centers of congregate care. Fortunately, the Massachusetts Legislature acted last month to preserve sheltered workshops in this state for those who choose to remain in them.
For some within the Obama administration, the wishes and preferences of the individuals and families most affected by deinstitutionalization do not appear to be of importance. Since 2009, the Justice Department, while at least partly under Bagenstos’ leadership, has filed, joined, or participated in more than 40 lawsuits in at least 25 states to provide individuals what it considers to be “full community integration.” As a result, hundreds of people have been moved from ICFs/IID homes, regardless of whether they or their families or guardians wanted to close the facilities they were living in or not.
In his article, not only does Bagenstos neglect to acknowledge the suffering and damage that has been caused by these institutional closures, but he does not appear to understand the financial corruption that pervades the largely privatized system of care that has replaced the large institutions.
For instance, Bagenstos maintains that “deinstitutionalization advocates now are fighting to expand the amount of state money spent in the community—and, especially in tight budget times, to defend existing community services against cuts.” But this doesn’t appear to recognize that the most potent force for deinstitutionalization advocacy today is to be found among the corporate providers that have moved in to the vacuum created by the disappearance of ICFs/IID. They are actually fighting to expand the amount of state money going into their own pockets, particularly the pockets of the huge bureaucratic layer of corporate executives that run these companies.
Hopp points out that between 1977 and 2010, as ICFs around the country were being closed, the number of residential settings serving people with developmental disabilities increased by more than 1,500 percent, with most of these new settings being small and privately operated.
Bagenstos and many within the current administration also seem not to understand that the federal Americans with Disabilities Act (ADA) and the Olmstead v. L.C. U.S. Supreme Court decision both recognize the need for a range of services for the developmentally disabled, including institutional care for those who desire it. Bagenstos discusses the ADA and Olmstead only as potential legal avenues to boost funding for the community-based system. And he starts with an unproven assumption that community-based care is better in all respects than institutional care.
“Over time, an evidence base has developed that has both refined and demonstrated the superiority of these (community-based) service models,” Bagenstos states in his article. He includes no citation for this claim. In fact, in addition to the problems cited above of abuse and neglect in the privatized system, academic experts have drawn mixed conclusions as to whether people who have transferred from institutional to community-based settings have experienced improvements in the quality of their lives or care.
Bagenstos also appears off base in what he writes about the history of the litigation over the closure of Fernald. He writes:
When Massachusetts responded to fiscal concerns by seeking to close the Fernald Developmental Center, its oldest institution for people with developmental disabilities—even though it offered residents and guardians a choice of transferring to another state institution—Fernald parents sought to reopen a long-closed pre-Olmstead case [Ricci v. Okin] that had been settled in 1993. The parents argued that the closure actually violated Olmstead, because it deprived them of the opportunity to oppose placement in the community.
Bagenstos’s statements about the reasons for the reopening of the Ricci case are overly simplistic at best. The Fernald families alleged in 2004 that by instituting staffing reductions and budget cuts at Fernald, the then Romney administration was violating U.S. District Court Judge Joseph Tauro’s 1993 disengagement order in the Ricci case that required the maintenance of high standards for care at Fernald and in other ICFs. The families also alleged that the administration was re-writing residents’ care plans and failing to certify that the residents would receive equal or better care elsewhere.
Secondly, while the Patrick administration did offer the Fernald residents a choice of a different ICF, the concern among the families, starting prior to the Patrick administration, was that the ICF they moved to from Fernald might itself subsequently be closed, leaving them with the prospect of multiple moves. That concern proved to be well-founded in 2008 when the Patrick administration announced it was closing three additional ICFs in the state, out of six then remaining. Only one of the two remaining ICFs in the state was listed by the administration as not being on the closure list.
Bagenstos also mischaracterizes a bill filed by then Massachusetts Congressman Barney Frank that would have given guardians of persons with developmental disabilities the right to opt out of those lawsuits supposedly filed on their behalf by the Justice Department and federally funded legal aid agencies to close facilities in which those disabled individuals happened to be living. Frank’s bill would also have required the Justice Department to consult with the guardians in any investigations undertaken of those facilities. Bagenstos writes:
Evidently blaming the Massachusetts government’s decision (to close Fernald) on the pressures caused by the threat of litigation, Representative Barney Frank, who represented the district in which Fernald was located, responded by introducing legislation that would limit the ability of federally funded Protection and Advocacy agencies—the source of much Olmstead litigation—to bring cases that could lead to the closing and downsizing of institutions. Both VOR and AFSCME (a state employee union) have vocally supported this legislation. Though the legislation has not moved in Congress, the support by one of its most stereotypically liberal members for a bill that would limit public interest lawsuits highlights the unusual political alliances that continue to surround deinstitutionalization litigation.
In our opinion, Frank’s bill would not have limited any organization’s ability to bring cases to close institutions. As noted, it would only have given guardians a choice as to whether to participate in those suits.
We are glad to see that Bagenstos at least believes that the closures of ICFs will not necessarily save money in the long run. He states that:
Although studies of deinstitutionalization have found that people who move from institutions to the community can achieve better outcomes at lower cost, it is reasonable to expect that the cost gap will shrink as people in the community receive more services. This may be especially true because a significant part of the cost gap reflects differences in the wages paid to workers in institutional and community settings.
In the final analysis, we think, the major problem that the developmentally disabled face is not the threat of institutionalization, it is the lack of adequate care and services in the supposedly deinstitutionalized system. As Hopp notes:
The legal framework is in place to support individualized care and choice. Advocates must set aside efforts to eliminate options of care and work together to expand options. This begins with a commitment to serving each individual: true person-centered planning.
The problem with the approach advocated by Bagenstos and many within the Obama administration is that it advocates the elimination of options for people with disabilities. It is a one-size-fits-all approach to care and services, and that size appears to be steadily shrinking as Bagenstos and others in the administration promote smaller and smaller residential settings that no longer meet high standards of care.
DDS expands privatized services despite family preference for state care
Patricia Murphy had to file a federal lawsuit in order to get her intellectually disabled sister out of a corporate, provider-operated group home, where she says she was subjected to abuse and inadequate care, and into a state-operated group home.
Murphy’s case illustrates how difficult the Department of Developmental Services has made it for people either waiting for services or receiving inadequate services in privatized group homes to obtain state-run residential placements in Massachusetts. DDS funds group homes run by both corporate providers and by DDS staff.
At the same time, people living in state-run developmental centers have been given priority in finding state-operated group home placements when the developmental centers have been closed.
Here are some facts to consider:
- More than 87 percent of the 372 people who have been transferred since 2008 from four developmental centers marked by the administration for closure have gone either to state-operated group homes or to two remaining developmental centers (primarily to the Wrentham Developmental Center). Only 47 people — less than 13 percent of the total — were transferred to corporate, provider-run group homes. This, to us, indicates, a strong preference among families and guardians for state-run care.
- As a result of this apparent preference, DDS has built 49 new state-operated group homes since 2008. But it has closed 28 such residences during that same period, resulting in a net increase in state-operated residences of only 21.
- There are apparently vacancies in state-operated group homes. DDS figures show that nearly all of the 99 residents living in the 28 residences that have been closed were moved to other state-operated residences.
- Yet, DDS is placing a priority on boosting funding and resources not to state-operated care, but to corporate providers, and has either cut funding for state-run care or provided more modest increases for it. The governor’s proposed Fiscal Year 2015 budget would result in an increase in the provider residential line item of almost 17 percent in inflation-adjusted terms, more than double his proposed 6.5 percent increase in the state-operated residential line item.
The new state-operated group homes built since 2008 appear to have been intended to accommodate only the residents transferred from the developmental centers. They have apparently not been made available for virtually anyone else. DDS is not only not building new state-operated facilities for persons other than former developmental center residents, it is apparently not letting people other than developmental center residents even know about the existence of state-operated residential care options.
Thousands of disabled individuals are reportedly waiting for residential services in Massachusetts, although the state does not maintain an official waiting list that would publicly identify the number of people of waiting. Others, such as Patricia Murphy, are apparently trying unsuccessfully to move family members or wards in the DDS system from provider-operated to state-operated care.
The administration’s policies of under-funding state-operated care, closing existing state-operated group homes, and preventing people from choosing state-operated care as a residential option are combining to reduce the availability of high-quality care throughout the DDS system. Direct-care workers in state-operated group homes have better training and benefits than workers in the provider-operated system. That’s why families from the closing developmental centers have chosen state-run facilities for their loved ones. But the administration appears to be more interested in promoting a privatized, provider-run system than in placing people in settings offering the best care.
According to information from DDS, 157 new provider-run homes have been built since 2008, bringing the number of such homes to more than 1,800 in Massachusetts. In contrast there are just 261 state-operated group homes in the commonwealth and only two fully functioning developmental centers that are not currently targeted for closure.
DDS has stated that it is currently projecting to build five new state-operated group homes, but it is also projecting to close six of them. Our question is why. Why build new state-operated homes and at the same time close existing homes, and moreover, why close these homes while people are waiting for residential placements?
Patricia Murphy’s lawsuit, which was filed last year, alleges that DDS routinely fails to disclose the existence of state-run homes and developmental centers to individuals applying for DDS care, and portrays corporate, provider-run homes as the only option for them. The plaintiff in the case, Kathleen Murphy, is severely intellectually disabled, and was a resident of a group home operated by a corporate provider to DDS. (Disclosure: Kathleen Murphy is represented by Thomas Frain, an attorney who is president of COFAR’s Board of Directors.)
“We had been asking DDS since 2006 to get her (Kathleen) into a state-operated group home, and they wouldn’t do it,” Patricia Murphy says. The federal complaint maintains that Kathleen Murphy suffered severe psychological harm and a risk of death in provider-run group homes. She was finally moved to a state-operated group home in February, but only after the lawsuit was filed.
According to the complaint, Kathleen was over-medicated in a provider-run residence with Depakote and Risperdal, drugs for bipolar disorder; however, that diagnosis of bipolar disorder later turned out to be mistaken. The suit alleges that DDS’s failure to move Murphy to a state-run facility coupled with its failure to provide people waiting for DDS care with the option of state-run residential care violate federal laws. Those laws include the Home and Community Based waiver of the Medicaid Law (42 U.S.C., Section 1396), which requires that intellectually disabled individuals and their guardians be informed of the available “feasible alternatives” for care. In addition, the complaint alleges that the state is violating the federal Rehabilitation Act (29 U.S.C., Section 794), which states that no disabled person may be excluded or denied benefits from any program receiving federal funding.
DDS’s projected number of transfers to provider residences didn’t materialize
In 2009, DDS projected that a substantial number of former developmental center residents would choose provider-run residential care. In its Community Services Expansion and Facilities Restructuring Plan in 2009, DDS projected that slightly more than half of a then estimated total of 402 developmental center residents would be transferred to provider-run group homes. In other words, DDS was projecting a major increase in the number of clients living in provider-run residences — a situation that would result in millions of dollars of additional state revenue to the providers.
As it turned out, the 47 former developmental center residents who actually transferred to provider-run residences was 77 percent fewer than the 206 that DDS had projected. The number of residents who actually transferred to state-operated group homes (156) was 39 percent higher than what DDS projected in 2009, and the number that transferred to other developmental centers (169) was more than double what DDS originally projected.
In actuality, things didn’t work out the way DDS and the providers had projected or apparently hoped. Possibly for that reason, it would appear that DDS is continuing to try to maximize the providers’ revenue and business opportunities at the expense of adequate and appropriate care and services for the vulnerable people in the Department’s care. DDS needs to rethink its policies in this regard. At the very least, DDS should let people seeking residential care know about existing vacancies in state-operated group homes. That is after all the law.
Setting the record straight yet again about the Fernald Developmental Center
Every year at budget time, the corporate providers funded by the Department of Developmental Services trot out the Fernald Developmental Center and the families that have appealed the transfers of their loved ones from the center as an example of an egregious waste of taxpayer dollars.
As today’s story in The Boston Herald demonstrates, this year is no exception. There are six or so residents left at the facility, which was targeted for closure by the Patrick administration in July 2010. But because those residents’ appeals are still pending in court or have only recently been decided, Fernald has remained open and is now costing $11 million a year to continue to operate. Ergo, the guardians and advocates of these residents have conspired in an evil plot to force the state to continue to pay to run this huge and unnecessary institution.
The problem with this argument is it’s not true. The reason it costs so much per resident right now to operate Fernald is because the administration never properly downsized the center as the population there was reduced. Admittedly, this would have taken some planning and possibly the construction on the campus of group homes for the remaining residents, which could have been operated cost-effectively.
The Fernald guardians and advocates had long proposed what we considered to be a win-win approach for both the residents and taxpayers, which would have allowed for the continued operation of Fernald and other developmental centers in Massachusetts that provide intensive, federally regulated care for some of the state’s most profoundly, intellectually disabled and medically involved residents. The Fernald proposal included both the downsizing of the facility and a “postage-stamp” arrangement under which the remaining Fernald residents would continue to occupy a small portion of the existing campus while the rest of the campus was opened up to other uses or development.
The administration, however, refused to discuss or even consider anything other than closing Fernald entirely and moving the residents to other locations around the state. About 14 Fernald guardians and family members exercised their legal right to appeal the decision to move their loved ones, many of whom had spent close to their whole lives at Fernald and had benefited greatly from the expert care there.
Yesterday afternoon, I got a call from a Boston Herald reporter, who was dutifully writing up a story about this outrageous situation at the behest of DDS, the Arc of Massachusetts and the Association of Developmental Disabilities Providers (ADDP). These three organizations bring up the Fernald situation every year to lawmakers and the media in order to make the case that more state funding should go to DDS corporate providers and less to state-run programs such as the remaining developmental centers and state-operated group homes.
The Herald reporter first asked whether COFAR was supporting or working with the remaining Fernald residents. I said that we haven’t been actively involved in advocating for Fernald for several years because the closure has been in litigation, but that we believe the Fernald guardians have exercised their legal right to appeal the transfers of their wards. I stressed that while the cost per resident at Fernald might be very high right now, those guardians should not be blamed for it because it is the administration that never considered proposals described above to downsize Fernald and operate it cost-effectively. I also said it is incorrect to consider that closing Fernald will eliminate all costs of caring for these people. It will still be expensive to care for those residents in the community, I said, adding that no one knows the real cost because no one has ever done an independent study on it.
I added that the administration never agreed even to negotiate the downsizing and postage-stamp proposals. I also provided the reporter with information about a key cost of DDS care that has not been counted in the developmental center closures: the cost of salaries of the executives running the hundreds of corporate provider agencies that contract with DDS. We have looked at the tax records of more than 250 of these contractors and found that the cost of paying their CEOs, executive directors, and other executives runs to between $80 million and $90 million a year. That’s where the waste of our taxpayer dollars really is.
I wasn’t surprised to see that very little of what I said made it into the actual story, which also made it sound as though COFAR is still actively involved in the fight to save Fernald. The story did accurately quote me as saying the state has mismanaged Fernald and could downsize it; but beyond that no mention was made in the article of the postage-stamp proposal and the administration’s failure to consider it, or of the lack of an independent study on the cost of care in the community system. And there was no mention of the provider executive salary issue.
The story, however, does include a quote from Leo Sarkissian, executive director of the Arc, about how “outrageous” it is to be “spending that amount of money (on Fernald) when there’s the existence of very good options for each of the people living there.” In other words, let’s blame the families for this. And there’s a quote from Gary Blumenthal, president of the ADDP, who termed Fernald “almost a ghost town” — a phrase that provides no valid insight into the situation at Fernald, but predictably made it into the headline of the Herald story.
Sarkissian is also quoted as saying, “Let’s move on. We have so many other important things that are issues.” To that, I’d just ask, who is it who keeps bringing this particular issue up each year?
Our proposal to Senate Ways and Means to redirect some DDS funding in Fiscal Year 2015
Governor Patrick and the state House of Representatives have specified funding for the Department of Developmental Services budget for the coming fiscal year that is way out of balance.
Budget legislation proposed by the governor and approved so far by the House would raise the level of funding to DDS corporate residential providers to more than $1 billion. That’s an increase to the providers of more than $140 million, or more than 16 percent, over current-year spending in FY 2015 dollars. At the same time, both the governor’s and the House budgets would either cut or provide much more meager increases for most other DDS line items.
Here’s a proposal to the Senate Ways and Means Committee to restore some balance to DDS funding. As noted below, we are suggesting to the Ways and Means Committee, which is now considering the entire state budget, that at least part of the proposed increase in the Community Residential (corporate provider) line item be redirected to other DDS line items.
We have calculated that if the governor’s proposed increase in the Community Residential line item were reduced by just 2.1 percent – to a 14.7 percent increase – the Legislature could re-direct close to $18 million of the governor’s $145 million increase to the state-operated group homes, DDS service coordinators, the Autism Division, Turning 22 program, Respite and Family Supports, and the remaining developmental centers in the state.
COFAR’s proposed changes in DDS line items for FY ‘15
| Suggested decreases from gov’s FY ’15 budget numbers | Percent inc. from FY ’14 | Suggested increases from gov’s FY ’15 budget numbers | Percent inc./dec. from FY ’14 | ||
| Community res. (providers) | ($18,142,085) | 14.7% | State-operated group homes | $6,755,404 | 10.0% |
| Adm. (service coordinators) | $2,714,544 | 5.0% | |||
| Facilities | $6,254,933 | -7.7% | |||
| Autism Div. | $446,207 | 6.0% | |||
| Turning 22 | $460,003 | 5.0% | |||
| Respite Family | $1,136,399 | 5.0% | |||
| Total | $17,767,489 | ||||
The following are the details of our proposal:
Community Residential: FY ’15 budget line item 5920-2000: 14.7 percent increase
Both the governor and the House have proposed a disproportionately large increase in this line item for the coming fiscal year. We would urge the Senate Ways and Means Committee to propose a lower increase.
The governor proposed a $145 million, or 16.8 percent, increase in Community Residential funding in FY ’15 dollars. The proposed increase would bring the line item to $1.009 billion. This would amount to a 63.7 percent increase in funding for the providers since FY ’07.
On April 30, the House approved a slightly lower increase in the line item to $1.006 billion – still a 16.4 percent increase from the current year in FY ’15 dollars.
If the governor’s proposed increase was reduced by just 2.1 percent in this line item, it would save $18.14 million in FY ’15 dollars, which could be directed toward other line items that have been proposed for little or no increase in funding, or else are slated to be drastically cut, such as the facilities line item.
We would note that our proposal would still allow for a 14.7 percent increase in funding for the Community Residential line item, which would bring the line item to $990.7 million in FY ’15 dollars in the coming fiscal year. This reduction in the line item increase to 14.7 percent would allow for the following increases, or reductions in proposed cuts, in the following line items:
State-operated Residential 5920-2010: 10 percent increase
Both the House and the governor have specified a $12.6 million, or 6.5 percent, increase in funding for DDS state-operated group homes, to $206.3 million. We would urge the SW&M Committee to increase funding for this line item by an additional 3.5 percent, which would add $6.7 million to the amount proposed by the governor in this line item.
DDS data show that close to 42 percent of the 372 individuals moved out of developmental centers in the state since 2008 were placed in state-operated group homes. Just 13 percent of those individuals went to provider-run group homes. (We’ll say more about this in an upcoming post.)
Since 2008, 38 new state-operated group homes have been built in the state, but 3 have been closed or converted to provider-operated homes. DDS has projected that it will build an additional 6 state-operated group homes, but will close or convert 5 state-operated facilities to provider residences. Meanwhile, 157 new provider-operated group homes have been built since 2008.
Additional funding is needed for the state-operated group home system to preserve it as a choice for people waiting for residential care in the DDS system.
State facilities 5930-1000: Reduction from a 12.7 percent cut to a 7.7 percent cut
The governor proposed a $15.8 million, or 12.7 percent, cut in the developmental centers line item for FY ’15, to $109.2 million. The House approved even a deeper cut of 13.5 percent. Since FY ’07, the line item will have been cut by close to 47 percent if the governor’s FY ’15 budget is adopted.
The administration is dismantling the developmental centers; however, since 2008, more than 45 percent of the individuals moved out of the centers have been sent to either the remaining Wrentham or Hogan developmental centers. Some funding should be restored to this account to ensure that current conditions in the remaining centers are maintained.
DDS administration 5911-1003: 5 percent increase
The governor proposed just a $551,000 increase in the DDS administrative account in FY ’15 dollars, to $65.9 million, which is less than 1 percent in inflation-adjusted numbers. The House approved even a smaller increase – just 0.43 percent.
The DDS administrative account pays for service coordinators, who are being phased out of their jobs as the administration and Legislature look to award service coordination work to corporate providers. Providing just a 5 percent increase in this line item would add $2.7 million to the amount proposed by the governor.
Autism Division 5920-3010: 6 percent increase
Both the governor and the House specified virtually no increase in the Autism Division line item, which amounts to a cut of 1.8 percent in FY ’15 dollars. Given the growing public awareness of the prevalence of people with autism in the population, it is troubling that neither the administration nor the Legislature appear to have placed a priority on funding this line item.
COFAR would suggest providing for a 6 percent increase in the Autism Division line item for FY ‘15, which would add $446,207 to the governor’s proposed amount.
Respite family supports 5920-3000: 5 percent increase
Both governor and the House specified a 2.9 percent increase in this line item, which would bring it to $54.9 million in FY ’15. The line item has been constantly under-funded and would be 12 percent lower in FY ’15 dollars than it was in FY ’07 if the governor’s budget is approved.
COFAR is suggesting a 5 percent increase in funding for this line item, which would add $1.14 million to the amount proposed by the governor and the House.
Turning 22 5920-5000: 5 percent increase
This line item has also been constantly under-funded for many years. Both the governor and the House specified no increase in funding for the line item for FY ’15, which amounts to a 1.9 percent cut in funding in FY ’15 dollars.
A 5 percent increase in funding for this line item would add $460,000 to the amount specified in the governor’s and the House budgets.
Our proposal emphasizes family choice
We think this proposal to redirect some DDS funding is consistent with our long-standing position that individuals and their families — and not the providers — should have the primary say in the type of care and services they receive. Families have consistently indicated, for instance, that they prefer state care to care provided by corporate providers. Our proposal would redirect millions of dollars to neglected or underfunded state-operated programs and services.
For that reason, we are not supporting the providers’ call for an additional $5.5 million increase in the DDS community day and work account (5920-2025) because the providers want the additional money to be used to transfer intellectually disabled persons from sheltered workshops to day programs that they run. COFAR is supporting the preservation of sheltered workshops in the state for those who choose to remain in them.
Finally, given the lack of adequate oversight of the DDS contracting system, our proposal to redirect DDS funding would at least reduce some of the increase that may well go straight into the pockets of the corporate executives of the provider companies. We hope the Ways and Means Committee will consider our proposal before releasing their version of the budget this week.
