Archive
COFAR asking Baker administration whether DDS residents and staff will be among first to get COVID vaccine
In the wake of a recommendation earlier this week from a federal advisory panel that healthcare workers and residents of long-term care facilities get the first doses of the coronavirus vaccine, COFAR has asked the Baker administration whether that would include residents and staff in the Department of Developmental Services (DDS) system.
So far, we haven’t gotten an answer.
According to a Politico article, the recommendation on Tuesday of the advisory panel to the Centers for Disease Control (CDC) isn’t binding. But the article stated that many states that are putting together vaccination plans are looking to the CDC as a guide.
In an email on Wednesday morning to state Health and Human Services Secretary Marylou Sudders and DDS Commissioner Jane Ryder, I asked whether the Baker administration will include DDS residents and staff in its plans for distribution of the first doses of the vaccine that Massachusetts gets.
It appears the primary thrust of the recommendation on Tuesday of the CDC panel is to ensure the early vaccination of residents and staff of nursing homes and other long-term care facilities for the elderly.
Protecting residents of nursing homes from COVID-19 has been a priority of the Baker administration as well, given the large number of those residents that have died from the virus.
In my email to Sudders and Ryder, I noted that we support the early distribution of the vaccine in nursing homes, assisted living facilities, and correctional centers. But we want to make sure the DDS system is included in those distribution plans, and that it is clear that both group homes and developmental centers in the DDS system fall into the category of long-term care facilities, in the view of the administration.
We have long been concerned that the administration has overlooked the DDS system in its efforts to protect the state in general from the impact of the COVID pandemic.
The Politico article stated that Trump administration officials say that up to 40 million doses of vaccines from Pfizer and Moderna will be available by the end of 2020. That is enough to vaccinate 20 million people. Between 5 and 10 million additional doses are anticipated to be available per week in early 2021.
Pfizer and Moderna are both seeking FDA authorization for their vaccines.
End to lockdown
The vaccinations will obviously bring an end to the ongoing isolation of DDS clients in group homes and developmental centers. Those residents have been subjected to increasingly strict and often inconsistent lockdown measures during the current surge of the virus.
Most of the increased COVID cases in the DDS system have been among staff, but the burden of the lockdown has fallen most heavily on the residents themselves.
Deaths among DDS residents do not currently appear to be rising; but, as of the latest two-week surveillance testing period ending November 25, the number of staff testing positive for the virus in DDS provider-run group homes had risen from 504 to 526.
As of December 1, the number of residents testing positive in provider-run group homes actually appeared to be leveling off from the week before, at 175.
We’re sure that all of the residents in the DDS system and their families would like to know how the Baker administration is interpreting the CDC’s definition of long-term care facilities with regard to distribution of the vaccines. We hope we get an answer from the administration soon.
Outdated DDS visitation guidance leads to contradictory provider policies
The Department of Developmental Services appears to be leaving it up to its residential providers to impose family visitation restrictions in light of the latest surge in COVID-19 cases in the DDS system.
This appears to have resulted in inconsistencies and contradictions among visitation policies among different providers, and potentially overly restrictive policies on testing and quarantines in some cases.
The last time DDS appears to have updated its visitation guidance was September 23, prior to the current COVID surge.
I sent an email query on Monday (November 30) to DDS Commissioner Jane Ryder, asking whether she intends to update the Department’s September 23 guidance on visitation, and whether some standardization of requirements for indoor visits and quarantines might be necessary. I haven’t yet received a response to my query, which was also sent to the DDS ombudsman.
Indoor visits banned, contradicting DDS guidance
At least three providers have recently banned indoor visits entirely by family members, and enacted varying requirements for testing and quarantining group home residents who were taken by family members home for Thanksgiving and other visits.
One provider is banning all visits of group home residents to their family homes until further notice.
The September 23 DDS guidance permits indoor visits by family members and allows off-site visits by residents.
The same provider, however, has not allowed any indoor visits since March, according to a family member. The provider has also sharply limited outdoor visits, and, as noted, banned out-of-group home visits.
In a directive issued last week, a second provider stated that visits to its group homes would only be permitted outdoors or via Zoom or Facetime.
Another provider stated that on-site visitation was being suspended until further notice “due to rising COVID rates nationally and in the state.”
Contradictory directives on quarantines after off-site visits
Different providers appear to have adopted widely varying policies on quarantining residents after the residents have left group homes even for short visits
One provider allows off-site visits by residents, but has lately required a three-day quarantine of any resident who is taken out of the group home. Another provider now requires a 14-day quarantine for any resident taken out of state.
As one family member said, however, it is very upsetting to residents to be subjected to multi-day, in-room isolation after returning to a group home, and it results in “very little benefit.”
The September DDS guidance does not require quarantines if residents are taken off site, but states only that they must be monitored for 14 days after returning to their group homes. Quarantines are required only if the resident shows symptoms.
Providers have different requirements on testing after off-site visits
Providers similarly appear to have contradictory policies regarding COVID testing after off-site visits.
One provider has required that residents taken off site receive a negative COVID test less than 48 hours before returning to a group home or other DDS-funded setting.
Two other providers, however, appear to require residents taken off site to wait a minimum of 72 hours between getting tested and returning to the group home.
One of those providers requires the resident to remain at the family home for 14 days before even getting the test. Even if the test is negative, the provider’s directive states that the resident must remain in isolation in the group home for an additional 72 hours and then needs a second COVID test.
Staff don’t appear to be subject to similar restrictions
As we have reported, the biggest jump in COVID infections in the DDS system, in terms of absolute numbers, appears to be among staff.
The number of COVID-19 positive staff in all provider-operated group homes (in DDS and other agencies in the Executive Office of Human Services) rose by more than 100% in the two-week period ending November 11. Yet, it is clear that staff regularly go in and out of group homes without the need for quarantines, in particular, unless they are symptomatic.
We have long suspected that the biggest risk to residents in the DDS system does not come from family members who visit them either outdoors or indoors under controlled conditions, but from staff who face few such restrictions.
We think DDS needs to reassess where the risks in the current COVID surge really lie, and to adjust their guidance accordingly. The burden imposed by restrictions on visits should not fall disproportionately on the families and the residents themselves.
Moreover, that updated guidance should be followed by all providers.
State data appear to show COVID has been the leading cause of death this year in the DDS system
Data obtained by COFAR from the state under a Public Records Law request unsurprisingly appear to show that COVID-19 has been the leading cause of death in the Department of Developmental Services (DDS) system since January.
Despite that, deaths among residents in the DDS system fortunately do not appear to be currently rising at as rapid a rate as COVID infections are rising among those residents. Most of the COVID-related deaths appear to have occurred during the first peak-COVID period in the state as a whole, in April and May.
The highest rate of COVID infection in the DDS system currently appears to be among staff. But the current death rate, if any, among staff isn’t publicly known. The Baker administration does not publish any current data on deaths among staff in the DDS system.
Data provided by the Disabled Persons Protection Commission (DPPC) under a public records request indicate that of the 650 residents in the DDS system who were reported to DPPC to have died between January 1 and November 4 of this year, the largest single reported cause of death has been COVID-19.
A total of 143 of the 650 reported deaths in the DDS system — or 22% — were reported to be due either solely or partly to COVID. That total includes numbers of cases where COVID was one of multiple reported causes.
Meanwhile, the number of COVID-infected residents and staff has surged in the DDS system in recent weeks. As shown in the first graph below, the number of DDS provider-operated group home residents testing positive for COVID-19 rose from less than 20, in one week in mid-October, to 131 as of the seven-day period ending November 17.
The graphs are based on weekly online state facilities data from the administration.
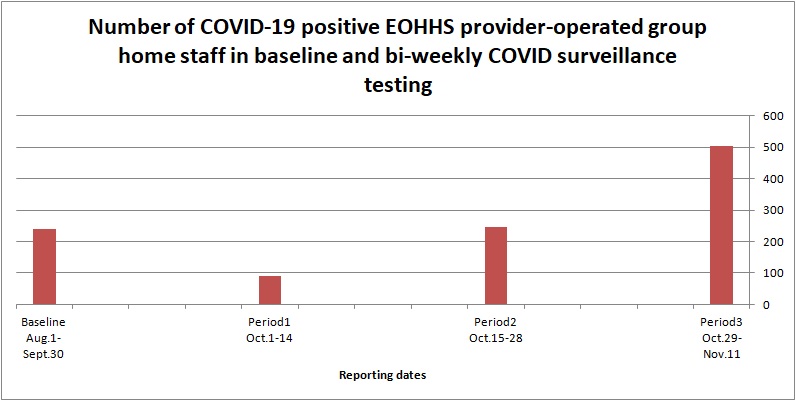
As the second graph shows, the number of COVID-19 positive staff in all provider-operated group homes (in DDS and other agencies in the Executive Office of Human Services) rose from 245 in the two-week surveillance testing period ending October 28, to 504 in the two-week period ending November 11. That is an increase over the previous two-week period of more than 100%. The number of COVID tests increased over the previous period by only about 12%.

Source: EOHHS online weekly state facilities reports
Source: EOHHS online weekly state facilities reports
At the same time, deaths among residents in the DDS system do not appear to be increasing at anywhere near the same rate as COVID infections. The rate of deaths of residents has stayed at less than five deaths per week in the DDS group home system since the end of October.
Between five and 10 deaths were recorded in the state’s two developmental centers in November, which does mark an increase over the absence of any deaths in the centers between the end of June and this month.
Data on causes of deaths are difficult to interpret
Data on causes of deaths, provided by DPPC, are not always clear and can be difficult to interpret. The data are based on causes of death as reported at or near the time of death to DPPC, and therefore appear to be unofficial.
As a result, it appears possible that some causes of death listed in the DPPC’s records may differ from causes listed in actual medical records of the deceased clients. However, DDS, which holds those medical records, would not disclose even aggregated numbers from those records of causes of death to us. (More about that below.)
All deaths in the DDS system must be reported at the time to DPPC; and DPPC did agree to disclose the aggregated numbers from those reports of the causes of those deaths.
As the chart below based on the DPPC data shows, COVID appears to have been the leading factor in causes of deaths of DDS clients since January, as reported to DPPC. Respiratory failure was the second highest factor, followed by cardiac arrest, cancer, and aspiration pneumonia (caused by choking).

Source: Reports to DPPC
One other problem we had in trying to interpret the DPPC data was that many different types and combinations of causes of death were listed by that agency. As a result, we had to try some creative approaches to grouping the data.
For instance, we grouped respiratory failure and pneumonia into one category, and counted 96 deaths in that category, or 14.8% of the total deaths between January 1 and November 4. We would note that if COVID was listed along with respiratory failure or pneumonia, we counted it in the COVID category as well.
That appears to raise a possibility that the total of 143 COVID deaths would be an underestimate of the real number of COVID-related cases in the DDS system if COVID was actually a factor in more of the respiratory failure cases than was reported. It seems possible that in some of those cases, COVID may have been a factor, but wasn’t reported or known at the time to be a cause.
Death rate dropped in the summer
Most of the deaths that have occurred in the DDS system that have been either fully or partly attributed to COVID appear to have happened in April and May. As the graph below shows, those deaths rose sharply from less than five in the second half of March to a total of 56 in each of the months of April and May.
The deaths just as abruptly tailed off from June through the middle of October. It remains to be seen whether what appears to be a slight uptick in the number of deaths in the second half of October will continue.
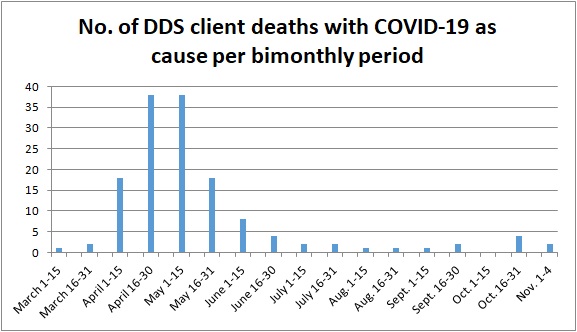
Source: Reports to DPPC
Loophole prevents release of DDS data
As noted above, the data from DPPC on deaths are based on reports to the agency, sometimes on the same day as each death occurred. DDS, which apparently has official causes of death in its records, denied our request for the numbers of clients per month who died from all causes, including COVID.
Due to what we see as a loophole in the state’s Public Records Law, the state’s public records supervisor reversed herself last month, and gave DDS blanket authority to deny our request for that information. DDS claimed the information is kept in confidential patient records and is therefore confidential.
In asking for that same information from DDS, we were not asking, however, for information that could reveal the identify of any particular client. Yet the Public Records Law contains a blanket exemption, known as “Exemption (a),” that states that if a state agency has an enabling statute that says its records are private, that statute overrides the Public Records Law.
(The DPPC has been trying to change its enabling statute to explicitly state that its records are not public, possibly for the reason above. That agency apparently wants to be able to cite Exemption (a) in many records requests. We have opposed DPPC’s attempt to change its statute.)
As we’ve said before, we think there is a compelling need, particularly during the ongoing crisis over the virus, for government to be open and transparent with the public about the impact of the pandemic on the lives and health of ourselves and our loved ones. We see no reason for the apparent bunker mentality that has been adopted by agencies such as DDS in that regard.
Administration now reporting human services staff COVID data, but not specifically for DDS
After months of failing to report the COVID-19 status of staff working in provider-run group homes and other facilities funded by the Department of Developmental Services (DDS), the good news is the Baker administration is at least finally starting to take those numbers publicly into account.
Staff-related testing information is now contained in weekly state facilities reports, which are posted online every Wednesday evening.
The bad news is the testing data listed are for all “congregate care sites operated by state-contracted (human services) providers.” The numbers of provider staff testing positive are not broken down among facilities funded by DDS, the Department of Mental Health, the Department of Youth Services, and possibly other agencies falling within an umbrella agency — the Executive Office of Health and Human Services (EOHHS).
The latest weekly state facilities report doesn’t break the data down by individual provider either. And that’s not to mention that there is still no testing even being done on DDS community-based day program staff.
The newly reported numbers of total EOHHS provider-staff who have tested positive in the past month can be found on Page 6 of the latest weekly report.
In addition to the lack of a breakdown of staff testing numbers by EOHHS department, there are other questions about the nature of the data presented in the latest report. It’s not clear, for instance, what is meant in the report by “congregate care” staff, particularly whether that refers only to group homes or includes larger Intermediate Care Facilities (ICFs) such as the DDS-run Hogan Regional Center and Wrentham Developmental Center.
Also, the Page 6 data reflects two-week testing periods while the rest of the report shows current numbers of COVID cases in the latest week.
This lack of specific and clear information in the weekly reports continues to be concerning, particularly since the data that we do have shows what appears to be the start of a second wave of the COVID-19 virus within the DDS system, in addition to the second wave that has hit the state as a whole.
Data show a surge of provider staff cases
The staff data on Page 6 of the latest weekly state facilities report show that the number of staff testing positive for COVID-19 in all EOHHS provider-run group homes started from a baseline of 240 as of September 30. Those positive provider staff rose by 91 in the first half of October, and by 245 in the second half of October, based on biweekly surveillance testing.
It is important to note that the baseline number of 240 is not a cumulative number of the total number of staff that contracted the virus since the start of the pandemic, but is only the number found to be positive during baseline testing conducted between August 1 and September 30.
The increase of 336 in positive staff cases during the two biweekly surveillance testing periods in October is a jump of 140%; and it would appear to mean that some 400 staff in provider-run group homes were potentially positive as of October 28.
Of course, the document doesn’t show how many of those staff are in DDS group homes, although DDS does have the largest number of group homes of any EOHHS department.
On page 2 of the report, the data show the number of residents testing positive in DDS provider-run group homes jumped from 46 to 65, as of the 7-day period ending November 3. The number of residents testing positive in state-operated group homes rose in that same period by only 1, to a total of 10.
State-operated “congregate care” staff cases
The number of staff, specifically in DDS, DYS, and DMH state-operated “congregate care” sites are also now listed on Page 6 of the latest weekly state facilities report. The number of those staff testing positive started from a baseline of 6 as of September 30, according to the latest report. Positive staff in those facilities rose by 2 in the first half of October, and by 20 in the second half of October.
Pages 1 and 2 of the weekly state facilities report have continued to list 7-day residential and staff data for both the Hogan and Wrentham facilities and state-operated group homes.
Surge in COVID cases could affect visitation
With the numbers showing, or at least implying, an increase in staff and some residents testing positive for COVID in the DDS system, DDS has indicated that it is leaving it up to providers to determine whether to reimpose restrictions on visitation by family members and guardians.
While visitation had been sharply restricted in the first several months of the pandemic, the latest guidance on the DDS website, which was issued in September, continues to allow both in-home and outdoor visitation.
However, as of the end of October, at least one provider was banning in-house visits. We received a notice from a parent of a resident of a group home run by American Training, a DDS provider, that all visits inside the provider’s group homes would be prohibited due to an increase in COVID rates in the Andover area. The parent said she was told visits to the home would still be permitted outdoors.
In response to a query from COFAR, a DDS spokesman said that despite the Department’s guidance, final decisions on visitation are being left to the discretion of the providers.
Unfortunately, we’ve heard about a number of cases in which providers have used the COVID crisis to ban or discourage visitation in order to keep family members and guardians in the dark about conditions in their homes.
Until a vaccine becomes available, it is clear that the COVID crisis will continue to present a major threat to DDS clients and staff, just as the crisis has for the general population throughout the country.
In the meantime, we hope that the Baker administration will take further steps to improve and clarify its public reporting of the testing status of clients and staff in the DDS system, and will provide clearer guidance and direction to both families and providers regarding visitation.
No Data: DDS group home staff data largely absent from administration’s public COVID test reports
Even though the Baker administration announced in August that they were requiring staff to be tested for COVID-19 in group homes for persons with developmental disabilities, it appears only a small portion of the results of those tests on staff are being made publicly available.
The administration’s Weekly State Facility Reports list numbers of state-operated group home and developmental center residents and staff who are currently COVID positive. But they do not contain any COVID testing data on what may be more than 25,000 staff working in the much larger network of provider-operated group homes.
Further, there is no information listed in the weekly reports on the numbers of deaths of staff working in any type of DDS setting. Data provided by DDS in June showed that anywhere from 3 to 15 staff members in group homes had died of COVID-19 as of the end of that month.
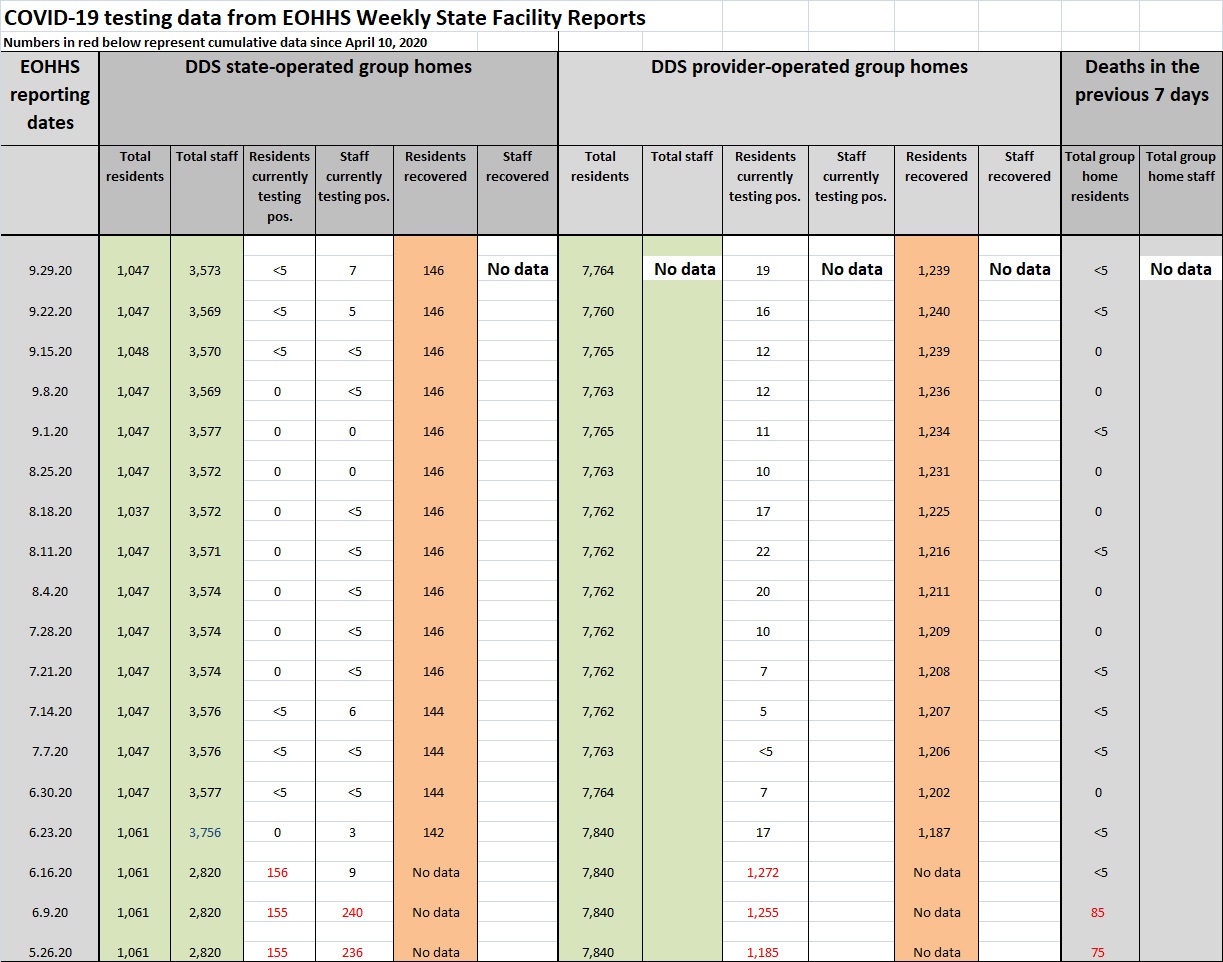
We created the chart below based on the administration’s online Weekly State Facility Reports from May 26 through the most recent report, dated September 29. (You can click on the chart to make it larger.)
The chart illustrates the data gaps, and points to some other problems with the way the administration reports the results of COVID testing in the Department of Developmental Services (DDS) system. In addition to the missing staff data, the positive test numbers are not cumulative, and there are no exact numbers given when there are less than 5 deaths or positive cases in any category in a given week.
We also have questions about the data on “residents recovered” from COVID. A note to the data states that the numbers “do not include all facility cases and recoveries over time.” As a result, it isn’t clear what portion of all recovered residents are included in the data.
As discussed below, the number listed in the weekly reports for residents having recovered from the virus in state-operated group homes — 146 — did not change from July 21 through September 29.
There is no similar data listed in the reports on recovered staff.
There are some 4,800 staff caring for some 1,400 residents in state-operated group homes and developmental centers run directly by DDS, according to the administration.
DDS has no figures on the total number of staff caring for the 7,800 residents in provider-run group homes around the state; but we are estimating that the number of such staff may be higher than 25,000.
EOHHS reports provide more limited data even for residents
The chart illustrates the gaps in staff data by including categories labeled “no data.”
Even with regard to residents, the Weekly State Facility Reports provide exact numbers only if more than 5 residents are positive or have died in a given week. As the chart shows, there are a number of entries that say <5, meaning the true numbers are anywhere from 1 to 4.
As a result, it can’t be determined in those instances exactly how many individuals were positive with COVID or died in a given week, in given settings.
For instance, it can’t be determined for the week of September 29 how many group home residents actually died of the virus. The data state only that the number was <5. It’s not clear why the numbers aren’t more exact. Among other problems, listing the data as a number range precludes adding numbers from different weeks together to obtain cumulative totals.
Data reporting changeover as of October 1
From April through September 30, DDS did provide us, upon written request, with total numbers of residents and staff testing positive in all group homes and developmental centers. DDS also provided exact numbers and provided cumulative testing data.
DDS has now referred us for testing numbers going forward to the Executive Office of Health and Human Services (EOHHS), which posts the Weekly State Facility Reports.
Since June 16, the Weekly State Facility Report numbers are for the current week only. Prior to that date, the reports did offer cumulative testing numbers, which are listed in red font in the chart above.
The changeover in data reporting from DDS to EOHHS coincides with a new testing system under which DDS and other human services providers must arrange for their own COVID testing.
I emailed Health and Human Services Secretary Mary Lou Sudders on Monday to ask whether EOHHS can provide us with more complete data, similar to the data that DDS provided. I also emailed Helen Rush-Lloyd, records access officer for the Department of Public Health (DPH). I was told DPH actually produces the Weekly State Facility Reports.
Neither Sudders or Rush-Lloyd has responded to my emails.
No longer listing cumulative data for positive tests
As noted, the Weekly State Facility Report data on positive test results are no longer cumulative. The reports list the number of group home and developmental center residents who are currently positive each week.
While previous weekly reports are available online, it isn’t clear if cumulative positive testing totals can be gleaned from them. As noted below, it also isn’t clear whether the numbers of recovered residents are actually cumulative.
The week of June 16 may have been the last Weekly State Facility Report listing clearly cumulative data. As of June 16, the report listed a cumulative total of 1,428 state and provider-operated group home residents as having tested positive.
That number, however, does not line up with our data from DDS. DDS at that time reported a cumulative total of 1,575 group home residents as having tested positive.
COVID recovery numbers didn’t change for state-operated group home residents
As noted above, it isn’t clear what the numbers listed in the Weekly State Facility Reports for recovered residents actually means, or whether the numbers are cumulative. The reports list the category as “Current Clients Recovered.”
A note at the bottom of each report states that the numbers listed for recovered residents “do not include all facility cases and recoveries over time.”
Recovered patients are further defined as having tested negative or having met symptom and time-based recovery guidelines issued by the Massachusetts DPH and federal Centers for Disease Control.
As the chart above shows, the number of state-operated group home residents listed as recovered remained at 146 from July 21 through the end of September. Prior to July, a cumulative total of 156 residents of those facilities were listed as having contracted COVID-19.
From June 15 on, as many as 24 additional state-operated group home residents, or as few as 6, contracted the virus, according to the data. It isn’t clear whether the 146 listed each week as having recovered represents the same group of residents, and whether no additional residents recovered from the virus after July 21.
We have similar questions about the number of residents listed as recovered in provider-operated group homes. While 1,187 residents of those facilities were listed as recovered in the June 23 Weekly State Facility Report, that number rose by only 52 — to 1,239 — as of September 29.
It isn’t clear to us whether only 52 additional residents recovered from the virus in the provider-run group homes in the three-month period after June 23. It is also unclear what the cumulative total was of those residents testing positive was during that same period of time.
We hope that EOHHS improves its public reporting of COVID testing results in the DDS system by eliminating the gaps in the data, making all the numbers exact, and providing cumulative data in addition to current data.
In not providing clear and complete reporting on the COVID crisis in the system, and in failing to respond to questions about the reporting, the administration loses a bit more of its credibility every day in that respect.
The state’s attorney general needs to do more than follow and grab COVID media headlines
Massachusetts Attorney General Maura Healey made national headlines and newscasts with her announcement last week of criminal charges against two leaders of the Soldiers’ Home in Holyoke for allegedly mishandling a COVID-19 outbreak at the facility that led to the deaths of 76 veterans.
We are not second-guessing Healey’s decision to criminally prosecute the Soldiers’ Home superintendent and former medical director in this matter. Our questions and concerns are over the overall investigative goals, or lack thereof, that not only Healey, but Governor Baker and the Legislature have with respect to the COVID crisis in the state.
What happened at the Soldiers’ Home was certainly horrific and potentially a case of grossly negligent management. But the Soldiers’ Home wasn’t the only institutional residential setting in which large numbers of people were infected and have died of the virus.
Our focus has been on the nearly 4,000 staff and residents of residential facilities in the Department of Developmental Services (DDS) system who contracted COVID-19 since April, and the 110 residents and an undetermined number of staff who have died of it.
Yes, Governor Baker has developed what has appeared to be a thoughtful plan over the past several months for testing the general population in the state for the virus, and reopening businesses and other venues as infection rates have declined.
But some groups of people appear to have been overlooked in this process, and we think people with intellectual and developmental disabilities are among them.
We’ve written repeatedly about the treatment of clients in the DDS system with respect to the COVID crisis as if they were an afterthought. Until very recently, there appeared to be no coherent plan for testing the thousands of residents and staff in the system, and huge gaps still potentially remain in the testing program and public reporting of the results.
DDS staff, in particular, have not faced a testing requirement until this month, and even that requirement is rife with questions and a potential loophole. The administration was slow to get personal protective equipment to the residential DDS system, and it still isn’t clear whether the level of training and oversight of staffing and care in the system is adequate.
Does any of this concern Govern Baker or Attorney General Healey or the state’s legislative leaders? We’ve seen little or no evidence that it does.
One might argue that 110 deaths in the DDS system is a relatively low percentage of the system’s total population. But 110 deaths is 110 deaths too many. How many of those deaths might have been prevented had there been adequate testing and training of staff?
How does bringing charges against two officials who ran one residential facility in the state ensure that there will be improvements in the practices and procedures in all other congregate care facilities?
While criminal charges in the Soldiers’ Home case may be warranted, we would submit that criminal charges should be among the last actions taken by the attorney general in response to a public health crisis like this one. Those charges should come only after the AG has conducted an investigation of the overall response of the state’s congregate care institutions and policies and practices, both public and private.
Those comprehensive investigations are almost never done, and we strongly doubt one was done by Healey’s office. Governor Baker, himself, ordered an independent review focused solely on the Soldiers’ Home deaths, which resulted in a report in June that was widely covered by the media.
That report proved the rule that the investigations that are done are targeted to specific events and almost never offer insights into underlying problems that are usually much wider in scope.
And public officials and administrators react almost exclusively to the resulting media reports in the hope of generating headlines favorable to themselves. It’s no surprise that headline-making indictments have come out of the Soldiers’ Home case.
While those deaths certainly warranted major media coverage, the media have been singularly uninterested in similar problems in the DDS system. After some initial coverage of concerns we, in fact, raised early on about the administration’s inadequate efforts to protect DDS clients from the virus, there has been almost no media coverage from roughly May onwards.
All of this may explain Attorney General Healey’s overall lack of interest in the DDS system. More than a year ago, we contacted Healey’s office to raise concerns about the AG’s apparent lack of focus on abuse and neglect of persons with developmental and other disabilities. While we appreciate that staff from her office did agree to meet with us, we received no indications in response to our subsequent queries that anyone was following up on our concerns.
Given that Healey had, at the time, taken an active role in scrutinizing and penalizing operators of nursing homes that provided substandard care to elderly residents, we asked her office for records of similar fines, settlements or penalties levied against DDS providers from the previous five years. Her office was unable to come up with virtually any records of such actions.
Many in the political system have been celebrating the Soldiers’ Home indictments as a signal that the state is aggressively going after the people responsible for failing to prevent COVID infections and deaths in the commonwealth’s institutions. Unfortunately, we’re not seeing a lot to cheer about at this point.
DDS ordered to provide records on causes of death in system. But will we ever see those records?
The state public records supervisor ordered the Department of Developmental Services (DDS) this week to provide records we have been seeking since early July on the numbers of DDS clients who have died since January and their causes of death.
It’s another win for us in our public records battles with several state agencies for COVID-related information. But these victories have had a hollow feeling lately because, as we’ve reported, these agencies have largely not been complying with the supervisor’s orders. We’re hoping this situation changes soon.
In this case, we have been trying to determine the percentage of total deaths in the DDS system that have been due to COVID-19.
DDS first denied the records in late July and then again in early September, arguing that the information is kept in each client’s “confidential client record,” and, as such, is exempt from disclosure under the Public Records Law. Secondly, DDS argued that it has not attempted to aggregate that data and is therefore not required to create such a record.
Public Records Supervisor Rebecca Murray essentially sided with us in our contention that both of DDS’s arguments for denying the records were flawed.
We argued that DDS’s claim that the information is exempt is based on a technicality that contradicts the spirit of the Public Records Law. The law exempts records that would disclose a client’s identity; but such a disclosure would not happen in this case.
Even though the cause of death is contained in a client’s confidential record, we are not seeking that full record and would not be able to determine any client’s identity based on an aggregate listing of causes of death.
In her September 22 decision, Murray wrote that, “The Public Records Law strongly favors disclosure by creating a presumption that all governmental records are public records.” She added that:
…it appears that the Department (DDS) does possess cause of death information, although not in aggregated form. Where the Department can redact the remainder of the client records that contain this information, it is unclear how providing this information would require “creation of a new record” ….Therefore, I find that the Department has not met its burden in responding to this request.
Murray ordered DDS to provide us with records “consistent with this order, the Public Records Law and its Access Regulations, within 10 business days.”
Hopefully, DDS will comply with the order. But, as we have previously noted, the Executive Office of Health and Human Services (EOHHS), the Department of Public Health, and DDS do not appear to feel that they are compelled to comply with Murray’s orders.
EOHHS has yet to comply with an order Murray issued on July 24 to provide us with clarification whether the agency possesses internal emails on mandatory staff testing in the DDS system. EOHHS has also not yet complied with an August 18 order to provide us with additional emails regarding public reporting of COVID results.
Finally, DPH has not complied with an order on August 10 to provide us with records on payments made to Fallon Ambulance Service, which has been conducting mobile testing for COVID-19 in the DDS system.
As I said, we’re hoping these agencies begin complying with the law. There are a few signs that that may be happening. I was told this morning by the public records supervisor’s office that EOHHS would have a response later today for us on the mandatory staff testing records. It would be their first response since July.
That would be good news. But the question remains: Will we ever see any of the actual records we’ve requested from EOHHS or any of these other agencies? I guess we’ll fully believe it when we see it.
Administration’s new COVID testing plan for DDS system may contain a staff loophole and reduce public reporting
Questions linger over a change in the way COVID-19 testing is being done in the Department of Developmental Services (DDS) system, including whether the change contains a loophole for staff testing and whether it could mean less publicly reported data.
The change in testing policy was instituted last month by the Executive Office of Health and Human Services (EOHHS), which has taken charge of the testing program. It appears DDS and possibly other agencies under the EOHHS umbrella will have little or no involvement in managing the testing.
Baker administration officials are not answering many of our questions about the new testing policy, which is outlined in an EOHHS directive last month to all residential DDS providers. The directive requires the providers both to undertake their own COVID testing for the first time and to include all residential program staff in that testing requirement.
Under the EOHHS directive, residential providers must now engage their own testing providers and labs, and will be reimbursed by the state for the costs. The directive changes a policy in the DDS system under which a single company, Fallon Ambulance Service, has been providing mobile testing to group homes around the state.
While we support a portion of the new policy requiring that residential staff undergo “baseline testing,” a number of questions have not been answered:
- Will residents and staff actually undergo follow-up biweekly “surveillance” testing, or will an apparent loophole in the EOHHS policy prevent surveillance testing in many regions of the state?
- Will day program staff avoid a testing requirement altogether, under the EOHHS policy?
- Will the results of the staff testing be made public, and who will report those results?
The apparent testing loophole
While the EOHHS directive specifies that baseline testing for staff and residents in all DDS group homes and developmental centers be done by September 30, it is not clear whether biweekly retesting, or “surveillance testing,” will actually go into effect in all regions of the state.
The EOHHS directive establishes a “regional transmission threshold” in order to determine the need for surveillance testing. Each of five regions of the state is identified as either a “high transmission” or “low transmission” region for COVID-19.
High-transmission regions are those that have a weekly average transmission rate equal to or greater than 40 cases per 100,000 residents. Low-transmission regions are those that have a transmission rate less than 40 cases.
According to the directive, providers located in high-transmission regions must undertake the surveillance testing. However, providers in low-transmission regions are required only to do surveillance testing when there are individuals in their facilities who show symptoms of the virus.
The transmission rates in each region are published weekly by EOHHS. As of the most recent weekly report, dated September 16, only one of the state’s five regions met that 40-cases threshold. That was the northeast region, which had 41 new cases. The western region had a low of 15 cases, followed by the central region with 21 cases, the southeastern region with 23 cases, and the Boston region with 31 cases.
Thus, as of this month, only the northeast region currently meets the threshold of positive cases among residents that would apparently trigger the ongoing surveillance testing requirement.
This threshold requirement sounds to us like a loophole that at least currently avoids surveillance testing in most of the DDS system. DDS staff, in particular, will only need to be tested once in most regions of the state, and will not have to be retested unless the rate of infection rises significantly among the general population in the region.
It is not clear, however, that the rate of COVID infection in group homes and other DDS facilities is directly related to the rate of infection in the general population. Without regular retesting of staff, in particular, it will be difficult to identify possibly rising infection rates in the DDS system.
Day program staff left out of testing requirement
DDS staff are also left out of the new EOHHS testing policy in another respect. As we have reported, the EOHHS directive did not include staff working in day programs. It is unclear what the reason is for that omission or whether extending the directive to day programs is under consideration.
We expressed concern to DDS Commissioner Jane Ryder in an email on August 28 that a failure to include day program staff in the directive appears to leave a major hole in the testing program in the DDS system. Ryder has not responded to our message.
Community-based and other types of provider-run day programs were reopened in early August as data began to indicate declining rates of the viral infection in the state. But the administration acknowledges that a risk of infection remains in the day programs.
Although day programs have been reopened, some residential providers are not sending residents to them because of the COVID infection risk. At this time, we don’t actually know how many day programs are operating or how many people are attending them. But whatever that number is, there is apparently no requirement that staff in those programs be tested.
Public reporting requirements may be reduced
As noted, in requiring that DDS residential providers arrange on their own for COVID testing of residents and staff, EOHHS is ending the Fallon Ambulance Service mobile testing program.
While that mobile testing program has been ongoing, DDS has provided us, upon written request, with cumulative testing data for clients and staff. That data has also shown the rate of testing being done by Fallon. It is not clear that that same level of data will continue to be reported after September 30, in part, because it does not appear that DDS will have testing data after that date to report.
On September 16, DDS ombudsman Christopher Klaskin told us that from September 30 on, “providers are required to report progress directly to (EOHHS) for completion of baseline staff testing – so they (EOHHS) are collecting that data point moving forward.”
Klaskin also said that “updated numbers moving forward are only reflective of that data point and will not include surveillance testing.” He did not respond to my query as to whether this means that results of surveillance testing will not be reported publicly by EOHHS.
EOHHS weekly online testing data do not show results for provider staff
Adding to our concern about the potential for reduced reporting of COVID test results is EOHHS’s ongoing policy of not publicly reporting the results of COVID tests done on provider staff.
While online EOHHS Weekly Facility Reports show the number of clients in DDS-funded group homes and developmental centers who are currently positive for the virus, the reports do not include the testing results of staff of group homes run by DDS corporate providers. For reasons that have never been explained to us, the EOHHS reports only provide results for testing of staff in the DDS’s much smaller network of state-run group homes.
As noted, DDS has provided us up to now with the results of provider staff tests.
As we have reported, top EOHHS administrators discussed proposals in June for reducing public reporting of COVID testing results in DDS and other congregate care facilities, including the reporting of staff testing results.
Agencies not complying with Public Records Law on mandatory staff testing records
In general, as we have reported, information about COVID testing in the DDS system has been difficult to get from the administration. We have been asking since May for internal emails and other records from EOHHS, DDS, and the Department of Public Health (DPH) on mandatory staff testing.
To date, we have received zero records from those agencies in response to our request.
On July 24, the state’s public records supervisor ordered EOHHS to clarify whether they possessed any records responsive to our request, and to respond to our request “as soon as practicable.” To date, we have received no communication from EOHHS.
In sum, the jury is still out, in our opinion, as to whether EOHHS has adopted a serious and effective COVID testing policy for the DDS system. As of now, we have substantial doubts that it has done so.
Direct care workers need more than an official state day and billboards in their honor
Governor Baker and an employee union recently honored home care workers in Massachusetts with an official state day and billboards.
But we think those workers might appreciate better pay and health benefits even more.
Baker and the 1199SEIU health care worker union teamed up to declare “Home Care Day” on September 4. The SEIU also funded the placement of 13 billboards in Boston, Worcester, Springfield, and other cities to highlight minority home care workers.
Tim Foley, vice president of 1199SEIU, told the State House News Service he hoped the billboards will “let home care workers know they are valued by so many families across the commonwealth and push elected leaders to invest in the workforce.”
We agree that the governor and Legislature need to do more to narrow the enormous gap that exists between the wages of direct-care workers and the executive salaries of the primarily private providers that employ them.
In 2018, Baker did sign legislation to raise the minimum wage of direct-care and other workers to $15 an hour; but it won’t reach that amount until 2023. In 2017, the Legislature rejected efforts to raise direct-care wages to $15 as of that year, and rejected a bid last year to raise direct care wages to $20 per hour.
A bill (H.4171) that would similarly raise hourly direct care wages to $20 has been stuck in the Health Care Financing Committee since last November.
Yet, it’s not as if the governor and Legislature are reluctant to provide continually rising levels of funding to the providers themselves. It’s just that the provider executives have chosen not to pass much of that increase through to the direct-care workers. Instead, they have greatly boosted their own personal wealth.
We reported in 2012 that direct-care workers working for corporate providers contracting with the Department of Developmental Services (DDS) had seen their wages stagnate and even decline in previous years while the executives running the corporate agencies were getting double-digit increases in their compensation.
Since 2012, the line item in the state budget for DDS-funded residential providers has increased by nearly 45 percent in inflation-adjusted terms, to over $1.5 billion in Fiscal 2020. That is according to the Massachusetts Budget and Policy Center’s online Budget Browser.
Yet, as State Auditor Suzanne Bump’s office reported last year, while that boost in state funding resulted in surplus revenues for the providers, those additional revenues led to only minimal increases in wages for direct-care workers.
Bump’s May 8, 2019 audit found that the average hourly direct-care wage was $11.92 in Fiscal 2010, and rose only to $14.76 as of Fiscal 2017. That’s an increase of only 24 percent over that eight-year period, an amount that only barely exceeded the yearly inflation rate.
Meanwhile, according to the audit, the increased state funding to the providers enabled them to amass a 237 percent increase in surplus operating revenues (total operating revenues over total operating expenses) during that same eight-year period. The increased state funding was at least partly intended to boost direct-care wages, but it “likely did not have any material effect on improving the financial well-being of these direct-care workers,” Bump’s audit stated.
In 2017, SEIU Local 509 in Massachusetts issued a report similarly asserting that increases in funding to human services providers enabled the providers to earn $51 million in surplus revenues. The union contended that the providers could and should have used the surplus revenues to boost direct-care wages.
Confirming our 2012 findings, the SEIU’s 2017 report stated that during the previous six years, the providers it surveyed paid out a total of $2.4 million in CEO raises. The SEIU report concluded that:
This all suggests that the amount of state funding is not at issue in the failure to pay a living wage to direct care staff, but rather, that the root of the problem is the manner in which the providers have chosen to spend their increased revenues absent specific conditions attached to the funding. (my emphasis)
So, as noted, it isn’t a matter of the providers not having the money. The governor and Legislature need to pass a bill such as H.4171, which would require providers to use up to 75 percent of their total state funding to boost direct-care worker salaries to at least $20 per hour.
In other words, if state-funded providers aren’t willing to pay a living wage to the workers they employ, then it’s time for the state to step in and require them to do so. If that were to happen, Governor Baker would have put some substance behind a declaration of a Direct-Care Worker Day in Massachusetts.
Baker administration appears to be ignoring state orders on releasing public records on COVID response in the DDS system
We have been trying for months to get records from the Baker administration about its policies and practices for protecting people with developmental disabilities from COVID-19.
Not only have we largely been unsuccessful in prying what should be public information from three state agencies, but even Rebecca Murray, the state’s public records supervisor, has been unsuccessful in extracting that information on our behalf.
The public records supervisor heads a division within the office of Secretary of the Commonwealth Bill Galvin, which is charged with enforcing the state’s Public Records Law.
Since July, we have filed several appeals to Murray for records from the Executive Office of Health and Human Services (EOHHS) and the Departments of Developmental Services (DDS) and Public Health (DPH). Those agencies have either denied our requests for the records, given us contradictory indications as to whether they have the records, or simply failed to respond to our requests.
Murray has subsequently issued several orders to the agencies either to provide records to us or clarify whether those agencies have the records we’re seeking. But it appears these agencies either feel free to ignore Murray’s orders or to slow-walk their compliance as much as possible. Since the end of July, they have shown few if any signs of compliance.
It isn’t clear what Murray is going to do about it. Yet it is a basic tenet of democracy that government follow the Public Records Law.
At this point, we have four outstanding public records requests to the three agencies, and the agencies have failed to comply with Murray’s orders in at least three of those cases. In the fourth case, which involves our request for information on the causes of deaths in the DDS system since January, we believe the Department is misinterpreting the law in denying us that information.
In nearly all of these cases, it has been so many weeks or even months since we first asked for the records that fast-changing circumstances involving the COVID pandemic have made many, if not most, of the records we might receive out of date.
The following are our outstanding records requests, and what has transpired with them so far:
Records on mandatory testing of staff in the DDS system
On May 26, we first requested internal emails and other records from EOHHS, DPH, and DDS regarding mandatory testing of staff in the DDS system for COVID-19. To date, more than three months later, we have not received any records from any of those agencies.
We first appealed to Murray on July 14 regarding EOHHS, which gave us contradictory responses as to whether it possesses emails responsive to our request. On July 24, Murray issued an order to EOHHS to clarify whether it does possess the emails. To date, more than a month after Murray’s order, we have received no response from EOHHS in compliance.
Meanwhile, given the amount of time since we first asked for those internal communications, the situation involving mandatory staff testing has changed. In mid-August, EOHHS issued a directive requiring testing of all staff.
Given the amount of time that has passed since our May 26 records request, it does not appear likely that the records — if we ever do receive them — would cover the period of time in which the administration made the decision to issue the mandatory testing directive. But if and when we file a new request for updated records, who knows if we will get those either.
As noted, we received conflicting indications from EOHHS and later DPH as to whether they possessed the emails we were seeking.
In early June, an EOHHS official responded to us only to say that our request was so broad, it would result in a voluminous number of emails, and the agency would have to bill us an undetermined amount to retrieve and evaluate the records for release. As a result, on June 9, we we offered, at EOHHS’s request, to narrow our request to emails solely among EOHHS Secretary Mary Lou Sudders and her executive team, and sent during a two-month time-frame from April through June.
However, more than a month after we made our offer, EOHHS stated that they now could find zero responsive emails to our narrowed request.
In her July 24 decision, Murray ordered EOHHS to clarify whether they possessed any records responsive to our request, and to respond to our request “as soon as practicable.” To date, as noted, we have received no communication from EOHHS.
On August 13, we also appealed to Murray for help in getting similar records from both DDS and DPH regarding mandatory staff testing.
DPH also had responded to us, on June 17, that they had identified 2,762 emails as being potentially responsive to our request, and that it would cost us $1,626 to provide them. On June 18, the next day, we similarly offered to narrow our request in order to avoid that large a charge for the documents. To date, more than two months later, we have not received a response to our offer from DPH.
We never received any response from DDS to our May 26 records request, other than a notice on June 9 that the Department needed an additional five days to provide a response. That response never came.
On September 2, Murray ordered both DPH and DDS to respond to us within 10 business days with either a response to our June 18 offer to narrow our request, in DPH’s case, or a response to our original May 26 request, in DDS’s case.
Request for contract documents concerning Fallon Ambulance Service for COVID-19 testing
On June 16, we requested records from EOHHS concerning Fallon Ambulance Service’s contract to test for COVID-19 in the DDS system.
EOHHS responded a month later — on July 15 — with no records other than the contract itself. In response to a portion of our request, which was for records of state payments made to Fallon, EOHHS directed us to an online database maintained by the state comptroller. That database, however, did not clearly identify payments to the company.
On July 28, after fruitless efforts to get EOHHS to clarify its response, we appealed to Murray, who ordered EOHHS on August 10 to provide reasonable assistance to us in locating the payments to Fallon. To date, we have received no communication from EOHHS in compliance with that order.
Request for records relating to EOHHS Weekly State Facility reports on COVID-19
On June 25, we requested documents from EOHHS, DPH, and DDS concerning changes made to the presentation of COVID-19 data in online Weekly State Facility reports. We wanted to find out whether top administration officials had discussed changes that were made in late June to limit the information contained in the public reports.
On July 16 and July 28, we appealed the non-responses of all three agencies to those records requests. DPH and DDS subsequently stated that they possessed no responsive documents.
EOHHS did produce documents on July 31 — which is the last time we heard from them — partially responding to our records request. But we reinstated our appeal on August 4, arguing that the EOHHS response was incomplete. The agency clearly appears to have additional records that they did not provide.
Based on the limited records we did receive from EOHHS, we reported that top officials of the agency had indeed discussed reducing the information contained in the weekly online reports.
On August 18, Murray issued a decision in our appeal, stating that it was unclear whether EOHHS does possess additional responsive records, and ordering the agency to clarify that matter to us, once again, “as soon as practicable.” To date, we have received no further communications from EOHHS.
Records on deaths in DDS system
On July 9, we requested records from DDS on causes of death regarding all residents of group homes and other residential facilities in the DDS system since January 1 of this year. We wanted to determine the percentage of total deaths that have been attributed to COVID-19.
On July 23, DDS denied our request, citing, among other statutes, an exemption to the Public Records Law for “medical files or information.” We appealed, arguing that DDS is interpreting the exemption in a broader manner than it was intended or plainly states. The exemption specifically states that it pertains to:
…personnel and medical files or information; also any other materials or data relating to a specifically named individual, the disclosure of which may constitute an unwarranted invasion of personal privacy; (my emphasis)
We did not ask for information that pertains to any named individuals or that could therefore possibly constitute an invasion of anyone’s privacy. We noted that DDS could satisfy our records request by providing aggregate information on the total number of people who have died according to various causes. DDS already does this with regard to the number of deaths from COVID-19.
Murray ordered DDS on August 10 to provide us with a response as to whether the Department could provide us with aggregate data. No answer was forthcoming from DDS until September 3, at which time DDS issued yet another denial.
This time, DDS argued that while the Department does have information on the causes of death of DDS clients, that information is kept in their “confidential client record.” As such, the Department reasserted its contention that the information is exempt from the Public Records Law.
DDS’s September 3 response also stated that the Department has not attempted to aggregate that data and is not required to create such a record, even for the relatively short six-month period for which we are seeking it.
In a response we sent this morning to Murray, we maintained that DDS’s first argument is based on a technicality that contradicts the spirit of the Public Records Law, which is to prevent the disclosure of a client’s identity. Such a disclosure would not happen in this case. Even though the cause of death would come from a client’s confidential record, we are not seeking the record itself.
Secondly, while it is true that agencies are under no obligation under the Public Records Law to create new records, we believe aggregating data from existing records does not constitute creating a new record. The Department could choose to provide each cause of death as an individual record, with all other identifying information redacted, or could choose to list all causes of death in one separate record.
It’s hard to imagine that each of these three agencies has come to the conclusion independently that they will either ignore or stall as much as possible in complying with the Public Records Law. It seems the impetus for this has come from the top, or at least the top of EOHHS.
Sudders herself originally responded to our questions about the administration’s COVID strategies and responses, but then she stopped for some reason. Why stonewalling has become the administration’s strategy in midst of the COVID crisis is a question we find mind boggling.
