Archive
DDS turns COFAR’s public records request over to a computer, resulting in an initial processing fee estimate of over $22k
The Department of Developmental Services (DDS) has begun using computers and algorithms to locate and process records in response to our public records requests, and that doesn’t appear to have been a good thing for transparency.
In the latest case, I had asked DDS in January for records listing reasons for the closures of seven state-operated group homes during a two-year period from 2021 through this year.
You would think it would not be difficult for DDS to locate and provide a reasonably reviewable number of documents listing those reasons.
But in a response to my records request, a DDS attorney said the Department had “requested information technology (‘IT’) staff” to search for internal emails, and that the computer search had identified 33,541 such emails and attachments “that may be responsive.”
The DDS records attorney then noted that the Public Records Law allows agencies to charge $25 per hour for staff time in compiling and redacting documents in order to comply with privacy and other laws such as HIPAA.
The attorney stated that because it would take an estimated 837 hours to process the 33,500 emails, the fee for providing them to us would be $22,925. And that fee could go higher if the hourly estimate turned out to be low.
DDS supposed to use its “knowledge of the records”
Arguing that DDS could have located a small number of responsive records, I appealed the DDS response on January 23 to Manza Arthur, the state’s public records supervisor, who heads a division in the office of Secretary of the Commonwealth Bill Galvin. The Public Records Division was established to ensure that state agencies comply with the Public Records Law.
Arthur issued an initial “determination” on February 3 that DDS needed to explain more fully how it had calculated its fee. In addition, the supervisor stated that DDS must “must use its knowledge of the records to facilitate providing any responsive records.”
Arthur didn’t elaborate on what is involved in using knowledge in providing records. But to us, it seems to mean that DDS presumably has personnel who have knowledge of the issues involved, and that those individuals should be able to use that knowledge to find and produce a small number of responsive records.
In that case, there wouldn’t be a need to redact and process thousands of documents that may or may not be responsive to our records request.
A Guide to the Massachusetts Public Records Law published by CommonWealth magazine states, in fact, that a state agency’s “records custodian is required to use his or her ‘superior knowledge’ to determine the exact records that are responsive to (a public records) request.”
The use of such knowledge appears to be what was missing from the Department’s response to my records request. DDS appeared to have simply conducted a computer search for the records using search terms. Anyone can feed search terms into a computer. Institutional knowledge is much different.
DDS says it lacks “capacity,” apparently for a records search based on knowledge
In a phone conversation with the DDS records attorney on February 8, I suggested that instead of conducting a computer search for the records I was seeking, DDS should query departmental personnel with that knowledge of the issue and the records. I also offered to narrow my original request for documents to a period of four months between August and November 2021.
But in a February 17 written response to me, the DDS attorney stated that DDS “does not have the capacity to conduct searches for the documents responsive to your request.” Therefore, he said, DDS had once again requested It staff to conduct a computer search.
This time, the number of “potentially responsive documents” was narrowed to 2,399 emails. The attorney said that using an “algorithm for computing costs…,” DDS had calculated a new fee for producing records of $1,499.38.
While this estimated fee was down from DDS’s original fee estimate of $20,925, the revised estimate is still unacceptable to us. The DDS attorney didn’t elaborate on what he meant by lacking “capacity.” But the end result was the same as the first time. The Department was continuing to feed search terms into a computer.
A test for the state’s Public Records Division
As a result, on February 21, I once again appealed to the supervisor of records.
In my second appeal, I stated that using computers and algorithms to respond to public records requests — which DDS has now done on several occasions — invariably results in a large number of “potentially responsive” documents, which may or may not be truly responsive. Such computer searches also result in inordinately large processing fees for producing the records.
As noted, my narrowed records request concerned seven DDS-run group homes that were closed during the period from August through November 2021.
Does DDS lack such superior knowledge of records concerning those seven homes? Are there no employees within the Department who have an understanding of the reason or reasons that the homes, which the Department managed, were closed in that short period of time?
Is that what the Department means by lacking capacity? If there are no such knowledgeable employees in DDS, the Department should state that to be the case.
In my latest appeal, I asked the public records supervisor to order DDS to more fully explain what it means in saying the Department lacks the capacity to conduct anything other than a computer search for responsive records, and specifically why the Department cannot use its superior knowledge in searching for the requested records.
In our view, this is a potentially important test for the state’s Public Records Division.
Will the public records supervisor require DDS to query its employees about these records, which is something DDS apprently doesn’t want to do? Or will the supervisor find that doing a computer search is sufficient to constitute a use of institutional knowledge?
In that latter case, it would seem that DDS and other agencies would have the green light to turn every public records request entirely over to computer searches.
It’s certainly possible that the supervisor will come up with a different solution to the problem. We expect a determination from the supervisor next week.
State data appear to show COVID has been the leading cause of death this year in the DDS system
Data obtained by COFAR from the state under a Public Records Law request unsurprisingly appear to show that COVID-19 has been the leading cause of death in the Department of Developmental Services (DDS) system since January.
Despite that, deaths among residents in the DDS system fortunately do not appear to be currently rising at as rapid a rate as COVID infections are rising among those residents. Most of the COVID-related deaths appear to have occurred during the first peak-COVID period in the state as a whole, in April and May.
The highest rate of COVID infection in the DDS system currently appears to be among staff. But the current death rate, if any, among staff isn’t publicly known. The Baker administration does not publish any current data on deaths among staff in the DDS system.
Data provided by the Disabled Persons Protection Commission (DPPC) under a public records request indicate that of the 650 residents in the DDS system who were reported to DPPC to have died between January 1 and November 4 of this year, the largest single reported cause of death has been COVID-19.
A total of 143 of the 650 reported deaths in the DDS system — or 22% — were reported to be due either solely or partly to COVID. That total includes numbers of cases where COVID was one of multiple reported causes.
Meanwhile, the number of COVID-infected residents and staff has surged in the DDS system in recent weeks. As shown in the first graph below, the number of DDS provider-operated group home residents testing positive for COVID-19 rose from less than 20, in one week in mid-October, to 131 as of the seven-day period ending November 17.
The graphs are based on weekly online state facilities data from the administration.
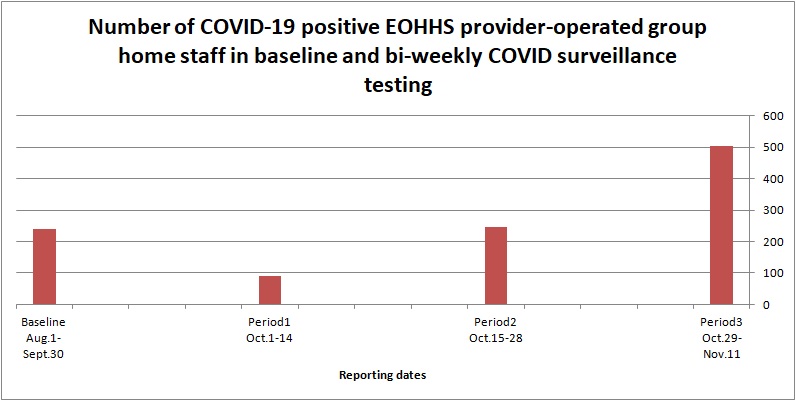
As the second graph shows, the number of COVID-19 positive staff in all provider-operated group homes (in DDS and other agencies in the Executive Office of Human Services) rose from 245 in the two-week surveillance testing period ending October 28, to 504 in the two-week period ending November 11. That is an increase over the previous two-week period of more than 100%. The number of COVID tests increased over the previous period by only about 12%.

Source: EOHHS online weekly state facilities reports
Source: EOHHS online weekly state facilities reports
At the same time, deaths among residents in the DDS system do not appear to be increasing at anywhere near the same rate as COVID infections. The rate of deaths of residents has stayed at less than five deaths per week in the DDS group home system since the end of October.
Between five and 10 deaths were recorded in the state’s two developmental centers in November, which does mark an increase over the absence of any deaths in the centers between the end of June and this month.
Data on causes of deaths are difficult to interpret
Data on causes of deaths, provided by DPPC, are not always clear and can be difficult to interpret. The data are based on causes of death as reported at or near the time of death to DPPC, and therefore appear to be unofficial.
As a result, it appears possible that some causes of death listed in the DPPC’s records may differ from causes listed in actual medical records of the deceased clients. However, DDS, which holds those medical records, would not disclose even aggregated numbers from those records of causes of death to us. (More about that below.)
All deaths in the DDS system must be reported at the time to DPPC; and DPPC did agree to disclose the aggregated numbers from those reports of the causes of those deaths.
As the chart below based on the DPPC data shows, COVID appears to have been the leading factor in causes of deaths of DDS clients since January, as reported to DPPC. Respiratory failure was the second highest factor, followed by cardiac arrest, cancer, and aspiration pneumonia (caused by choking).

Source: Reports to DPPC
One other problem we had in trying to interpret the DPPC data was that many different types and combinations of causes of death were listed by that agency. As a result, we had to try some creative approaches to grouping the data.
For instance, we grouped respiratory failure and pneumonia into one category, and counted 96 deaths in that category, or 14.8% of the total deaths between January 1 and November 4. We would note that if COVID was listed along with respiratory failure or pneumonia, we counted it in the COVID category as well.
That appears to raise a possibility that the total of 143 COVID deaths would be an underestimate of the real number of COVID-related cases in the DDS system if COVID was actually a factor in more of the respiratory failure cases than was reported. It seems possible that in some of those cases, COVID may have been a factor, but wasn’t reported or known at the time to be a cause.
Death rate dropped in the summer
Most of the deaths that have occurred in the DDS system that have been either fully or partly attributed to COVID appear to have happened in April and May. As the graph below shows, those deaths rose sharply from less than five in the second half of March to a total of 56 in each of the months of April and May.
The deaths just as abruptly tailed off from June through the middle of October. It remains to be seen whether what appears to be a slight uptick in the number of deaths in the second half of October will continue.
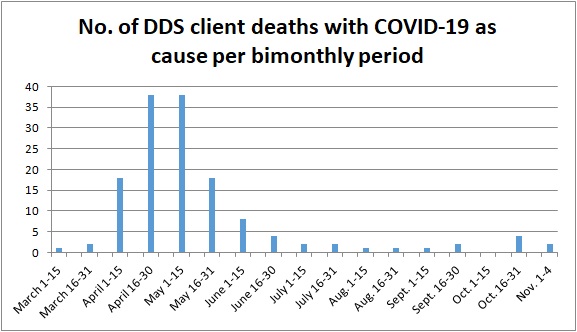
Source: Reports to DPPC
Loophole prevents release of DDS data
As noted above, the data from DPPC on deaths are based on reports to the agency, sometimes on the same day as each death occurred. DDS, which apparently has official causes of death in its records, denied our request for the numbers of clients per month who died from all causes, including COVID.
Due to what we see as a loophole in the state’s Public Records Law, the state’s public records supervisor reversed herself last month, and gave DDS blanket authority to deny our request for that information. DDS claimed the information is kept in confidential patient records and is therefore confidential.
In asking for that same information from DDS, we were not asking, however, for information that could reveal the identify of any particular client. Yet the Public Records Law contains a blanket exemption, known as “Exemption (a),” that states that if a state agency has an enabling statute that says its records are private, that statute overrides the Public Records Law.
(The DPPC has been trying to change its enabling statute to explicitly state that its records are not public, possibly for the reason above. That agency apparently wants to be able to cite Exemption (a) in many records requests. We have opposed DPPC’s attempt to change its statute.)
As we’ve said before, we think there is a compelling need, particularly during the ongoing crisis over the virus, for government to be open and transparent with the public about the impact of the pandemic on the lives and health of ourselves and our loved ones. We see no reason for the apparent bunker mentality that has been adopted by agencies such as DDS in that regard.
Baker administration appears to be ignoring state orders on releasing public records on COVID response in the DDS system
We have been trying for months to get records from the Baker administration about its policies and practices for protecting people with developmental disabilities from COVID-19.
Not only have we largely been unsuccessful in prying what should be public information from three state agencies, but even Rebecca Murray, the state’s public records supervisor, has been unsuccessful in extracting that information on our behalf.
The public records supervisor heads a division within the office of Secretary of the Commonwealth Bill Galvin, which is charged with enforcing the state’s Public Records Law.
Since July, we have filed several appeals to Murray for records from the Executive Office of Health and Human Services (EOHHS) and the Departments of Developmental Services (DDS) and Public Health (DPH). Those agencies have either denied our requests for the records, given us contradictory indications as to whether they have the records, or simply failed to respond to our requests.
Murray has subsequently issued several orders to the agencies either to provide records to us or clarify whether those agencies have the records we’re seeking. But it appears these agencies either feel free to ignore Murray’s orders or to slow-walk their compliance as much as possible. Since the end of July, they have shown few if any signs of compliance.
It isn’t clear what Murray is going to do about it. Yet it is a basic tenet of democracy that government follow the Public Records Law.
At this point, we have four outstanding public records requests to the three agencies, and the agencies have failed to comply with Murray’s orders in at least three of those cases. In the fourth case, which involves our request for information on the causes of deaths in the DDS system since January, we believe the Department is misinterpreting the law in denying us that information.
In nearly all of these cases, it has been so many weeks or even months since we first asked for the records that fast-changing circumstances involving the COVID pandemic have made many, if not most, of the records we might receive out of date.
The following are our outstanding records requests, and what has transpired with them so far:
Records on mandatory testing of staff in the DDS system
On May 26, we first requested internal emails and other records from EOHHS, DPH, and DDS regarding mandatory testing of staff in the DDS system for COVID-19. To date, more than three months later, we have not received any records from any of those agencies.
We first appealed to Murray on July 14 regarding EOHHS, which gave us contradictory responses as to whether it possesses emails responsive to our request. On July 24, Murray issued an order to EOHHS to clarify whether it does possess the emails. To date, more than a month after Murray’s order, we have received no response from EOHHS in compliance.
Meanwhile, given the amount of time since we first asked for those internal communications, the situation involving mandatory staff testing has changed. In mid-August, EOHHS issued a directive requiring testing of all staff.
Given the amount of time that has passed since our May 26 records request, it does not appear likely that the records — if we ever do receive them — would cover the period of time in which the administration made the decision to issue the mandatory testing directive. But if and when we file a new request for updated records, who knows if we will get those either.
As noted, we received conflicting indications from EOHHS and later DPH as to whether they possessed the emails we were seeking.
In early June, an EOHHS official responded to us only to say that our request was so broad, it would result in a voluminous number of emails, and the agency would have to bill us an undetermined amount to retrieve and evaluate the records for release. As a result, on June 9, we we offered, at EOHHS’s request, to narrow our request to emails solely among EOHHS Secretary Mary Lou Sudders and her executive team, and sent during a two-month time-frame from April through June.
However, more than a month after we made our offer, EOHHS stated that they now could find zero responsive emails to our narrowed request.
In her July 24 decision, Murray ordered EOHHS to clarify whether they possessed any records responsive to our request, and to respond to our request “as soon as practicable.” To date, as noted, we have received no communication from EOHHS.
On August 13, we also appealed to Murray for help in getting similar records from both DDS and DPH regarding mandatory staff testing.
DPH also had responded to us, on June 17, that they had identified 2,762 emails as being potentially responsive to our request, and that it would cost us $1,626 to provide them. On June 18, the next day, we similarly offered to narrow our request in order to avoid that large a charge for the documents. To date, more than two months later, we have not received a response to our offer from DPH.
We never received any response from DDS to our May 26 records request, other than a notice on June 9 that the Department needed an additional five days to provide a response. That response never came.
On September 2, Murray ordered both DPH and DDS to respond to us within 10 business days with either a response to our June 18 offer to narrow our request, in DPH’s case, or a response to our original May 26 request, in DDS’s case.
Request for contract documents concerning Fallon Ambulance Service for COVID-19 testing
On June 16, we requested records from EOHHS concerning Fallon Ambulance Service’s contract to test for COVID-19 in the DDS system.
EOHHS responded a month later — on July 15 — with no records other than the contract itself. In response to a portion of our request, which was for records of state payments made to Fallon, EOHHS directed us to an online database maintained by the state comptroller. That database, however, did not clearly identify payments to the company.
On July 28, after fruitless efforts to get EOHHS to clarify its response, we appealed to Murray, who ordered EOHHS on August 10 to provide reasonable assistance to us in locating the payments to Fallon. To date, we have received no communication from EOHHS in compliance with that order.
Request for records relating to EOHHS Weekly State Facility reports on COVID-19
On June 25, we requested documents from EOHHS, DPH, and DDS concerning changes made to the presentation of COVID-19 data in online Weekly State Facility reports. We wanted to find out whether top administration officials had discussed changes that were made in late June to limit the information contained in the public reports.
On July 16 and July 28, we appealed the non-responses of all three agencies to those records requests. DPH and DDS subsequently stated that they possessed no responsive documents.
EOHHS did produce documents on July 31 — which is the last time we heard from them — partially responding to our records request. But we reinstated our appeal on August 4, arguing that the EOHHS response was incomplete. The agency clearly appears to have additional records that they did not provide.
Based on the limited records we did receive from EOHHS, we reported that top officials of the agency had indeed discussed reducing the information contained in the weekly online reports.
On August 18, Murray issued a decision in our appeal, stating that it was unclear whether EOHHS does possess additional responsive records, and ordering the agency to clarify that matter to us, once again, “as soon as practicable.” To date, we have received no further communications from EOHHS.
Records on deaths in DDS system
On July 9, we requested records from DDS on causes of death regarding all residents of group homes and other residential facilities in the DDS system since January 1 of this year. We wanted to determine the percentage of total deaths that have been attributed to COVID-19.
On July 23, DDS denied our request, citing, among other statutes, an exemption to the Public Records Law for “medical files or information.” We appealed, arguing that DDS is interpreting the exemption in a broader manner than it was intended or plainly states. The exemption specifically states that it pertains to:
…personnel and medical files or information; also any other materials or data relating to a specifically named individual, the disclosure of which may constitute an unwarranted invasion of personal privacy; (my emphasis)
We did not ask for information that pertains to any named individuals or that could therefore possibly constitute an invasion of anyone’s privacy. We noted that DDS could satisfy our records request by providing aggregate information on the total number of people who have died according to various causes. DDS already does this with regard to the number of deaths from COVID-19.
Murray ordered DDS on August 10 to provide us with a response as to whether the Department could provide us with aggregate data. No answer was forthcoming from DDS until September 3, at which time DDS issued yet another denial.
This time, DDS argued that while the Department does have information on the causes of death of DDS clients, that information is kept in their “confidential client record.” As such, the Department reasserted its contention that the information is exempt from the Public Records Law.
DDS’s September 3 response also stated that the Department has not attempted to aggregate that data and is not required to create such a record, even for the relatively short six-month period for which we are seeking it.
In a response we sent this morning to Murray, we maintained that DDS’s first argument is based on a technicality that contradicts the spirit of the Public Records Law, which is to prevent the disclosure of a client’s identity. Such a disclosure would not happen in this case. Even though the cause of death would come from a client’s confidential record, we are not seeking the record itself.
Secondly, while it is true that agencies are under no obligation under the Public Records Law to create new records, we believe aggregating data from existing records does not constitute creating a new record. The Department could choose to provide each cause of death as an individual record, with all other identifying information redacted, or could choose to list all causes of death in one separate record.
It’s hard to imagine that each of these three agencies has come to the conclusion independently that they will either ignore or stall as much as possible in complying with the Public Records Law. It seems the impetus for this has come from the top, or at least the top of EOHHS.
Sudders herself originally responded to our questions about the administration’s COVID strategies and responses, but then she stopped for some reason. Why stonewalling has become the administration’s strategy in midst of the COVID crisis is a question we find mind boggling.
