Archive
Has the state been using hundreds of millions of taxpayer dollars in a reserve fund as promised to boost direct-care wages?
The state has appropriated more than $400 million in taxpayer funds to a human services provider reserve fund over the past two years, with at least three quarters of that amount supposed to be used to raise wages of direct-care staff of human services providers in Massachusetts.
Low wages have caused a continuing staffing shortage and worsening care in corporate provider-run group homes funded by the Department of Developmental Services (DDS).
Governor Healey is now pledging an additional $390 million to the “Chapter 257 Human Services Reserve” line item in the coming Fiscal Year 2025 budget, bringing the total appropriations to nearly $800 million. Chapter 257 was a law passed in 2008 that was intended to biennially set and increase state payment rates to human services providers.
But there seems to be little or no available information thus far as to:
- The amount of money in the reserve fund that has actually been spent to date to boost direct-care wages;
- How the administration or Legislature are able to track whether providers are raising those wages.
The reserve line item has included language in the FY ’23 and ’24 budgets stating that “any human service provider receiving revenue under said Chapter 257 shall use not less than 75 percent of received funds for compensation for their direct-care, front-line and medical and clinical staff.” However, the line-item language does not explain how that requirement would be carried out or enforced.
An administration spokesperson told us that that the governor’s proposed $390 million appropriation to the provider reserve fund in FY ’25 “is based on a model that supports wages no lower than $20/hour.”
One provider executive told us their agency was paying direct-care workers $17.50 an hour. So, presumably, the administration expects that that provider’s workers will receive at least a $2.50 per hour increase in their wages.
But whether those wage increases will actually happen is unclear. Similar promises in the past haven’t been met.
Funding rates for provider-run group home and day programs are set by regulation, after a public hearing process. Those rates are calculated based on what appear to be “benchmarked” expenses for wages and non-salaried costs. It isn’t clear, however, that the providers are required to pay those benchmarked wages.
What does seem to happen regularly is that the provider executives are paid higher and higher salaries and other compensation, while direct-care worker wages stay relatively stagnant.
Compare, for instance, the average direct-care salary in Massachusetts in FY ’22 of $43,260 (see below) with the total compensation that year to David Jordan, president of the Seven Hills Foundation, a DDS provider, of $1.2 million, and to his wife Kathleen Jordan, executive vice president and CEO, of $455,351.
Inspector general and state auditor had similar oversight concerns about payment of wages
In 2022, the Massachusetts Inspector General’s Office stated it had investigated complaints that state Executive Office of Health and Human Services (EOHHS) providers had misused $139 million in COVID pandemic relief funds that were supposed to be spent on direct-care staffing and other activities. Instead, providers allegedly spent the funds on executive salaries.
The IG stated that EOHHS did not fully implement its recommendations to develop detailed provider expenditure reports regarding state funding intended to be spent on staffing. The IG also stated that EOHHS failed to provide guidance to providers on reporting those expenditures.
In 2019, the state auditor found that major increases in funding to the human services providers Under Chapter 257 had led to surplus revenues for the providers, but had resulted in minimal increases in wages to direct-care workers.
We are asking both the IG and State Auditor to investigate the management and oversight of the reserve fund.
No clear oversight or tracking of direct-care wages by the state
It remains unclear how the state verifies or tracks the amount that human services providers pay in wages to their direct-care and other frontline workers. We asked this question of both administration officials and legislators, and have received no answer to it.
Oversight processes used by the state involving the provider reserve fund raise a number of similar questions.
For instance, in the FY ’23 and FY ’24 state budgets, the provider reserve fund language required EOHHS to provide a report to the Legislature’s House and Senate Ways and Means Committees on “ongoing and proposed initiatives” to increase direct-care wages. Those reports were required to be submitted in March 2023 and April 2024 respectively.
However, the March 2023 report, which COFAR obtained under a Public Records request, did not appear to provide that information. There was no mention in the report of any specific initiatives to raise direct-care wages, or even of the amount of funding appropriated under the provider reserve line item in that fiscal year.
The requirement that providers spend 75% of their reserve account funding on direct-care wages wasn’t mentioned in the March 2023 EOHHS report. The report was simply a spreadsheet that listed provider wage information, which the report stated had been collected from state Uniform Financial Reports (UFRs) and from the federal Bureau of Labor Statistics (BLS).
The EOHHS report did show that the average direct-care wage in Massachusetts as reported on provider UFRs was $43,263, or $20.80 per hour, in FY ‘22. That average had increased from $18.38 – or by 13% — from FY ’21.
Those wage averages were lower than BLS median numbers listed in the EOHHS report. The BLS median for FY ’22 was $21.94 per hour. It doesn’t appear that there is any requirement that providers pay the BLS median amount.
Also, based on our own review of UFRs, it doesn’t appear that those reports offer a way to track whether individual providers are actually spending 75% of their state revenues on direct-care wages. The reports we reviewed showed the amounts providers paid in total salary and wages, but did not appear to us to clearly break out the providers’ expenditures on direct-care wages.
We asked OSD for an explanation of the breakdown of expenses under the UFR system. An OSD official referred us to EOHHS, which did not respond to our request.
No directives issued on raising direct-care wages
In January, we also sent two Public Records Law requests to EOHHS and DDS, seeking documents concerning the impact of the Reserve fund on direct-care wages and any directives that have been issued to providers about spending 75% of their reserve account funding on direct-care wages.
In response to our Public Records requests, both EOHHS and DDS stated that they had no records of any such directives; and they provided no records concerning the impact of the reserve account funding on wages.
Healey’s budget doesn’t include wage increase language
It appears that the administration and the Legislature have at least one major difference in their planned approach to addressing the wage problem. Governor Healey’s proposed budgets for FY ’24 and ’25 have not included the provider reserve fund language inserted by the Legislature requiring providers to direct 75% of their funding to direct-care wages.
That language was inserted by the Legislature in the Fiscal ’23 and ’24 budgets. It remains to be seen whether the Legislature will once again insert the language in the FY ’25 budget.
It’s unclear why the governor has not included that language in her budget proposals. A request to the governor’s Office of Constituent Services and to EOHHS for a response to that question about the reserve fund requirement has gone unanswered.
We support higher pay to direct-care and frontline workers. We ourselves have called for a minimum wage of $25 per hour for those workers.
At the same time, we have heard the promises before. Each year, more taxpayer money is given to the providers in line with those promises. DDS-funded group home providers received roughly $1.7 billion this year. Yet, the promises don’t appear to be kept. A few years ago, the state auditor found that those providers were earning surplus revenues as a result of all of that state funding.
We think the state needs to enact tighter controls over the billions of dollars it gives to the providers in order to ensure that they really do honor the promises of higher direct-care wages. To the extent providers are still earning surplus revenues due to funding from the reserve account, the state needs to make sure that the money really is going to direct-care workers and not to executives.
Governor Healey’s proposed FY ’25 budget for DDS raises questions about her priorities for state vs. corporate-run care
Governor Maura Healey last week proposed a budget for Fiscal Year 2025 that includes an increase in funding for the Wrentham and Hogan Intermediate Care Facilities (ICFs) and state-operated group homes in Massachusetts.
But the governor’s budget doesn’t appear to be an attempt to change a longstanding practice of underfunding those state-run services and steadily increasing funding to corporate group home and community-based day program providers.
Healey proposed an increase of only $1.2 million in the ICF line item, which would amount to a funding hike of less than 1%, for FY ’25. That is well under the current average inflation rate for New England of 2.9%. As such, the governor’s budget proposal represents a cut in the ICF line item when it is adjusted for inflation.
Healey’s proposed $15.3 million increase in the state-operated group-home line item would amount to a 4.8% funding boost. While that is above the inflation rate, it is still far less than the governor’s proposed percentage increases in many DDS corporate provider line items.
For instance, Healey is proposing an 18.5% increase in the community-based day program line item, a 19.3% increase for transportation providers, and a 22% increase for respite providers.
Corporate group home cut would be offset by reserve account increase
Healey cut the DDS corporate provider group home line item by $40.3 million earlier this month as part of an across-the-board series of “9C” cuts in the face of a decline in projected revenues in the current fiscal year.
But in her FY ’25 budget, the governor is proposing not only to restore $23.2 million of the $40.3 million cut to the line item, she is also proposing a record-breaking $217 million increase to a separate reserve fund for the corporate providers. The governor’s FY ’25 budget would bring total funding under the Human Services Provider Reserve fund to $390 million.
So it would appear that despite the declining revenues, corporate DDS and other human services providers would receive a net increase of nearly $200 million under the governor’s budget plan.
Questions about provider reserve fund
Last week, The Boston Globe reported that Healey was planning in her FY ’25 budget to “tackle the staffing crisis plaguing social service care providers with a big investment…” That investment appears to include the governor’s proposed $390 million appropriation to the human service provider reserve fund, plus $95 million from a number of other reserve funds.
The total of $485 million in proposed additional funding is projected by the administration to raise direct-care wages to $20 an hour, “at the lowest,” the Globe reported.
We have a number of questions about the oversight of the reserve fund, however. We have long been unable to get answers to those questions, including the amount that has been spent from the fund to actually raise direct-care wages.
Also, for the past two fiscal years, the Legislature has inserted language into the line item for the reserve fund stating that 75% of the funding under the account must be directed to boost direct-care wages. Yet, this language is not included in Governor Haley’s FY 25 proposal for this line item.
Also. the governor’s FY ’25 budget plan indicates that zero dollars were expended in FY ’23 from this same line item that year even though $285 million had been appropriated to it. (See screenshot below.) It’s not clear what has been expended from the line item in the current fiscal year. This raises further questions for us as to where the money in the line item gone.

Minimal increase for ICFs
Gov. Healey’s FY ’25 budget would increase the ICF line item (5930-1000) by $1,777,048, or less than 1% over the current year appropriation. The FY ’25 ICF line item proposed amount is $124,809,632.
We are recommending a $5 million, or 4%, increase in the ICF line item in the FY ’25 budget. That would nominally raise the line item to $128,577,887. That increase would allow the line item to keep pace with inflation moving forward.
The news is better for the state-operated group home line item (5920-2010). The governor’s FY ’25 budget would raise that line item by $15,327,687 or 4.8%. That would raise the line item to $333,099,736.
ICF budget language
We are continuing to recommend changes in the ICF line item language. (The language doesn’t appear to be a part of the governor’s proposed budget. It gets added by the Legislature.)
The legislative language in the current year budget states that DDS must report yearly to the House and Senate Ways and Means Committees on “all efforts to comply with …(the) Olmstead (U.S. Supreme Court decision)…and… the steps taken to consolidate or close an ICF…” (my emphasis). However, closing institutions was not the intent of the Olmstead decision, which was written by the late Justice Ruth Bader Ginsburg.
We are concerned that the misstatements in the ICF line item in the state budget each year could allow the administration to justify continuing to underfund the line item, and possibly to seek the eventual closures of the Wrentham and Hogan centers.
We believe the budget language should be changed to state: “…the steps taken to consolidate or close an ICF and the steps taken to inform families of the choices available for residential care including ICF care.”
Secondly, the legislative line item lists three conditions for discharging clients from ICFs to the community, but leaves out one of the key conditions in Olmstead, which is that “the client or their guardian does not oppose the discharge.” We are requesting that that condition be added to the language in the line item.
In sum, we hope the governor and her staff will begin to understand the importance of state-run services as a part of the fabric of care for persons with intellectual and developmental disabilities. We are seeking a meeting with the governor and her staff to explain the disastrous result if current budget trends are allowed to continue.
Secondly, we think the administration and the Legislature need to understand that adequate oversight is needed of the hundreds of millions of dollars in budget appropriations that are intended to raise direct-care staff wages.
Family thanks DDS commissioner for referral of sister to the Wrentham Center
[Editor’s Note: We are reprinting a letter below that was written by Joan Norman, a sister of Ellen Gallagher. Ellen, who has an intellectual disability, had been living in a corporate, provider-run group home, which was moving to evict her because they admittedly couldn’t meet her needs.
Ellen has Alzheimer’s disease and limited mobility mainly due to limited vision issues and age. Joan describes her as “sweet and social,” but said she had been declining in the group home due the advancement of her disease and “sub-par medical and mental health care.”
In November, after advocacy on Ellen’s behalf by her family and members of COFAR, Department of Developmental Services (DDS) Commissioner Jane Ryder granted Ellen a rare admission to the Wrentham Developmental Center.
The number of residents at Wrentham and the Hogan Regional Center has been steadily declining for several years. That is because a succession of administrations has had a policy of declining to offer Wrentham or Hogan as residential options even when families ask for them.
We think Joan’s letter to Commissioner Ryder is an eloquent testimonial to the quality and importance of the care provided by state-run Intermediate Care Facilities (ICFs) such as the Wrentham and Hogan Centers.]
_____________________________________________________________________________________________
Dear Commissioner Ryder,
This letter is to formally thank you for supporting our sister’s referral to the Wrentham Developmental Center (WDC) back in November.
As you might remember, Ellen Gallagher, a 55-year-old Down Syndrome woman on hospice, with advanced Alzheimer’s, was living in her group home’s family room due to losing the ability to walk or get to her 2nd floor bedroom for almost 4 months.
We fought hard to find the appropriate placement with 24/7 nursing care so that Ellen could live out her remaining time with dignity and proper medical and mental health services. She needs services that include continuity and onsite care, rather than visiting the ER, hospital stays and unnecessary tests when she has had minor issues such as dehydration.
Now that she has settled in at WDC and has spent 6 weeks there, we can confirm it is an amazing living environment where her medical needs are finally being met and she is safe. She now has a handicap accessible bathroom and there are appropriate safety measures to match her abilities and changing needs.
We realize there is a push to keep people out of ICFs like WDC, but for medically complex clients it should be an option and it should be offered willingly by DDS. Families should not have to fight so hard for the care they need. ICFs are not the institutions of the past.
In this case, WDC is an example of the type of culture that is needed in community-based homes where a client’s medical care doesn’t involve neglect, safety issues and unprepared front-line workers.
We suspect costs are a driving factor behind limiting ICF placements. If you look at costs in community-based homes, many medically complex people end up with unnecessary emergent care because they don’t have onsite nursing care. Caretakers (with little to no medical background) use ambulances and hospitals “to be safe” when issues arise. Or worse, many clients go without proper medical care when they need it.
In my sister’s situation, in one incident, she was so dehydrated she ended up in the hospital nearly unconscious for days after being left virtually alone with a COVID infection. The staff handed her over to us after her isolation period, and we took her directly to the ER. She never gained back her strength, and it began a downward spiral of physical and mental decline for her.
In theory, nursing staff should be available to coordinate client medical care in group homes, but that is not how it often works. This can result in sub-par care, but also higher costs for the state’s Medicaid program when emergent care and unnecessary hospitalizations are used in place of qualified medical workers who can properly assess and address medical issues properly.
We urge you to continue supporting families who are seeking placements in an ICF like Wrentham, particularly for medically complex clients. Quality 24/7 medical care is not available in community-based homes, or it is patched together at best. WDC can offer this type of care.
There is a federal regulation supporting the choice of an ICF: Individuals seeking care, and their families and guardians, should be given the choice of either institutional or home and community-based services. [42 C.F.R. § 441.302(d)]. We got our choice for Ellen, and we sincerely thank you for supporting that decision. Please consider supporting others as well.
Sincerely,
The family of Ellen Gallagher
Globe update report has devastating findings about DDS provider-run group home system. Is the administration listening?
In the second of two reports on the corporate, provider-based group home system in Massachusetts, The Boston Globe last week characterized the system as “hobbled by poor staffing and struggling with allegations of abuse and neglect.”
Last week’s article was a follow-up to a report in September by the Globe’s Spotlight Team, which had focused on widespread abuse and neglect in provider-run residential schools for children and teens with autism.
We think the Globe’s reporting raises some important questions, one of which is whether the Healey administration and the Legislature are listening.
The Globe’s reporting echoes assertions about abuse and neglect in the system that we have been making for years. Moreover, we think the Globe is on the right track in noting a key factor plaguing the system, which we have long emphasized, of underpaid and undertrained staff.
Last week’s Globe article stated that most of the parents of autistic children whom the paper had interviewed asserted that, “Massachusetts has never solved long-term systemic problems of low pay and inadequate training” in the system.
The paper noted that although “the state has directed millions of dollars to group home providers to help them recruit and keep staff, pay remains similar to that of some retail and fast food workers; $17 to $20 an hour is typical.”
The Globe further stated that “a number of parents who spoke with (the newspaper) requested anonymity because they were afraid that (as we have long reported) state officials or providers would retaliate against them or their child if they spoke out.”
Paper needs to examine the causes
We hope the Globe will investigate the causes of that culture of retaliation and intimidation of families who complain about inadequate care and even abuse and neglect of their loved ones; and that it will investigate the causes of the underpayment of staff.
Understanding the causes of the underpayment of staff might help explain where the millions of taxpayer dollars went, given the money, as the Globe implied, doesn’t appear to have been used to raise staff wages to any significant degree. It might also explain why direct-care workers in the provider system have historically been underpaid and undertrained.
We think an investigation of the causes will reveal that the corporate provider system has always been been about making as much money as possible for its executives while paying its direct care workers as little as possible. That appears to explain why the privatization of human services has never met the promise of both delivering high-quality care and saving money. It may also explain why continual efforts to raise the pay of direct care workers don’t seem to lead to that result (see Massachusetts Inspector General’s 2021 Annual Report, page 27).
State-run services ignored as potential solution
Last week’s Globe article referred to concerns raised by the Arc of Massachusetts and the Massachusetts Association of Developmental Disabilities Providers (ADDP) — both of which actually lobby for the providers — about the shortage of staff and a lack of available group homes.
But while organizations like the Arc and the ADDP publicly decry the poor care and abuse of clients and the underpayment and shortage of staff, they both oppose a key potential solution to the problem, which would be to open the doors of the Wrentham and Hogan Developmental Centers and provide state-operated group homes as options to individuals seeking residential placements.
The state-run Wrentham and Hogan Centers and state-operated group homes have better trained and better paid staff than the provider-run homes. Yet the state-run facilities are losing population even as the number of people waiting for placements is growing. That is because the administration is not offering state-run facilities as options to people seeking placements, and is even denying requests made by families to place their loved ones in them.
The Arc and the ADDP appear to offer no solutions to those problems other than to ask the state to direct more money to them. In our view, those problems will never be solved unless the state changes the incentives driving privatized care.
Real oversight needed
In addition to providing families with state-run facilities as options for residential care, the state needs to take steps to ensure that group home providers really do raise the pay of their direct-care workers. It could begin to do that by establishing true financial oversight of the provider system. Currently, that oversight is practically non-existent.
Successive administrations and the Legislature have been committed to the privatization of DDS care for decades. They have maintained an extraordinarily close relationship with the corporate provider system in that respect. As noted, the Globe pointed out that both DDS and the providers often retaliate against parents and family members who dare to complain about poor care in the group homes.
We hope the Healey administration will not allow the anti-family culture and the continuing underpayment of direct-care staff in the DDS provider system to continue. We also hope the administration will consider reversing the longstanding administration policy of allowing state-run residential facilities to die by attrition.
The breakdown of the DDS system caused by decades of runaway privatization and mismanagement is finally being reported by the Globe. We hope the Healey administration is listening.
DDS: We’re ‘not required to answer questions’ about the number of state-run group homes or of residents
As we have reported, the census or number of residents living in state-operated residential group homes and Intermediate Care Facilities (ICFs) in Massachusetts appears to be steadily declining.
But in response to Public Records requests filed by COFAR, first in January and then last month, the Department of Developmental Services (DDS) said it no longer has information on the actual number of people living in state-operated group homes during the past five years.
If it is true that DDS has no such records, it would indicate that the Department is unaware of the status of one of its most important operational programs.
DDS has also declined to clarify an apparent discrepancy in its claims concerning the number of state-operated group homes that have been closed since 2021.
We have appealed to the state’s public records supervisor in an effort to get clarification on those matters. In a response filed on Friday to our appeal, a DDS attorney said that under the Public Records Law, “an agency is not required to answer questions…”
Denial of group home information
Prior to this year, DDS did provide us with information on the declining census in state-operated group homes. That data showed a steady decline from a high of 1,206 residents in Fiscal Year 2015, to 1,097 in 2021. During that same time, the census in the much larger network of corporate, provider run group homes, also funded by DDS, rose from 7,793 to 8,290.
But as of January of this year, as noted, that information on the census in the state-operated group home system is apparently no longer available. What DDS said in January and again in September is that while it can provide information on the total available beds in, or capacity of, state-run group homes over the past five years, it now has no records on the census.
In September, DDS stated that the total capacity of the homes had declined from 1,173 beds to 1,131 beds between Fiscal 2019 and 2023.
But capacity numbers don’t tell the full story, particularly if DDS has not been allowing admissions to the group homes, and there consequently are vacancies in them. In fact, DDS acknowledged last month that there were 91 vacancies in the state-run group home system as of June of this year. That would imply that the actual census in the homes is lower than the capacity.
But DDS also said that while there were 91 vacancies as of June 30, it has no records on the number of vacancies each year since Fiscal Year 2019.
We calculated the apparent drop in the census as of Fiscal Year 2023
Based on the Department’s partial records, we did our own calculation of the census in the state-run group home network as of Fiscal Year 2023. That year, it appears the census would have dropped to 1,040.
That census or number of residents is based on DDS’s statement that the capacity of the state-run group homes was 1,131 in Fiscal 2023, and that there were 91 vacancies in the group homes as of June 30, the last day of that fiscal year. Subtracting the number of vacancies from the census that year equals 1,040. (1,131 minus 91).
If that is the case, it would indicate that the census in the state-run group homes dropped from 1,206 in Fiscal 2015 to 1,040 in Fiscal 2023, a 14% drop. See our chart below.
 (Source: DDS. Note: We were not able to calculate the census in the state-run group homes in Fiscal Year 2022 because DDS did not provide a figure on the number of vacancies in that fiscal year.)
(Source: DDS. Note: We were not able to calculate the census in the state-run group homes in Fiscal Year 2022 because DDS did not provide a figure on the number of vacancies in that fiscal year.)
DDS will not clarify number of homes closed
As noted, DDS is not willing to clarify seemingly contradictory information on the number of group homes that have been closed and subsequently reopened since August 2021, during the height of the COVID crisis.
In September, DDS indicated that a net of nine state-run homes were closed between August 2021 and September 2023, leaving 251 homes remaining. However, eight months earlier – in January — DDS indicated that a net of six state-run homes were closed between August 2021 and January 2023, leaving 250 homes remaining as of January.
The implication of the January data was that 256 homes existed as of August 2021, whereas the implication of the September data was that 260 homes existed as of August 2021. The discrepancy might also mean that the number of homes that DDS said were closed may have been inaccurate.
However, as noted, when I asked that DDS provide clarification regarding that apparent discrepancy, a DDS attorney stated that, “Under the PRL (Public Records Law), an agency is not required to answer questions…”
The Public Records Law does require clarity
As part of our appeal, we stated to the public records supervisor that we believe DDS is, in fact, obligated to clarify information it provides under the Public Records Law.
The Massachusetts Guide to the Public Records Law, updated in March 2020, states that, “(State agencies) must help the requestor to determine the precise record or records responsive to a request…”
Also, the Public Records Law [M.G. L. c. 66, § 6A(b)] states that:
(The state agency) shall: …(i) assist persons seeking public records to identify the records sought;… and (iii) prepare guidelines that enable a person seeking access to public records in the custody of the agency or municipality to make informed requests regarding the availability of such public records electronically or otherwise…Each agency and municipality that maintains a website shall post the guidelines on its website.
In asking for clarification regarding the number of homes that existed as of August 2021 and have subsequently been closed, we were seeking the Department’s help in determining the precise record or records that might be responsive to our Public Records requests.
In sum, DDS’s response to our latest records requests seems to be part of the Department’s usual pattern of providing as little information as it feels it can get away with under the Public Records Law. The only other explanation is that the Department doesn’t have basic information about the programs it runs. We’re not sure which explanation is more troubling.
DDS confirms 91 vacancies in state-operated group homes even after several homes are shut
The Department of Developmental Services has confirmed for the first time that there are dozens of vacant beds in its state-operated group home network, even though the Department also says it has closed a net of nine homes since August 2021.
That information was provided to us in response to a Public Records Request, which we filed earlier this month with the Department.
In a response on September 26 to our request, DDS stated that as of June 30, there were 91 vacancies in the state-operated group home system.
COFAR has long contended that there are vacancies in state-operated homes because DDS generally does not inform individuals seeking residential placements of the existence of that system. Instead, DDS seeks to place virtually all persons in its much larger network of corporate provider-run group homes.
We are frequently told by families seeking placements for their loved ones in the state-run system that there are no vacancies in state-operated homes.
DDS also does not inform or generally admit persons to either of its two remaining Intermediate Care Facilities (ICFs) in the state – the Wrentham Developmental Center or the Hogan Regional Center. As a result, the number of residents living in state-run residential facilities has continued to decline, while the number in corporate run group homes has been steadily increasing.
COFAR has periodically filed Public Records requests with DDS to track the declining census in both the state-operated group home system and the Wrentham and Hogan Centers. The Wrentham and Hogan centers are the last remaining, congregate ICFs in the state.
DDS has continued to maintain that the corporate provider system is less restrictive and better integrated into the community than is the state-run residential system. However, as a Spotlight investigation by The Boston Globe showed on September 27, the corporate group home system is beset by abuse and neglect.
The data provided by DDS on September 26 show the following:
- There were 91 empty beds in state-operated group homes as of June 30. The Department, however, said it “does not have any responsive records” pertaining to COFAR’s request for the number of vacancies in the state-operated group homes each year from Fiscal Year 2019 to the present.
- The census, or total number of residents, at the Wrentham Center dropped by 48%, from 323 residents in Fiscal 2013, to 167 in Fiscal 2023.
- The census at Hogan dropped from 159 in Fiscal 2011, to 95 in Fiscal 2023, a 40% drop.
- The total census in the state-run group home system dropped by nearly 10% between Fiscal 2015 and 2021, according to previous DDS data. However, DDS has not provided information on the census in the state-run homes since 2021. We have appealed that apparent information denial to the state supervisor of public records.
- The total capacity, or number of beds, in the state-run group home system declined by 3.6% from Fiscal Year 2019 to Fiscal 2023.
- DDS says it closed a net of nine state-operated homes between August 2021 and September of this year. As noted below, the numbers don’t appear to add up, however. We’ve appealed for clarification.
Declining capacity and census in state-operated group homes
As the chart we created below based on the DDS data shows, the total capacity or number of beds has continued to decline in state-run group homes. That capacity declined from 1,173 beds to 1,131 beds, or by 3.6%, between Fiscal 2019 and 2023.
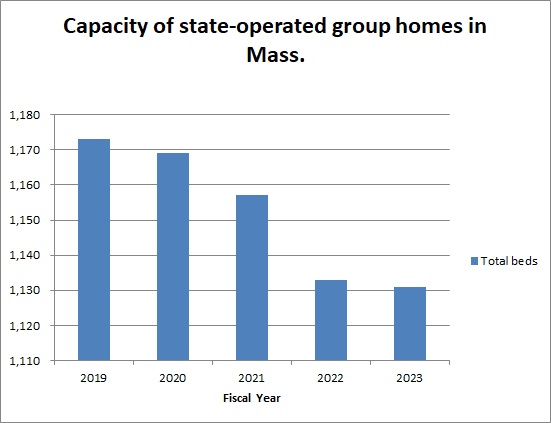
Previous data from DDS showed that the total census in the state-operated group homes declined from a high of 1,206 in Fiscal 2015, to 1,097 in 2021 — a 9% drop.
DDS numbers don’t add up
In addition to appealing the lack of census information regarding the state-run group home system subsequent to 2021, we are appealing to the public records supervisor to seek clarification from DDS regarding an apparent discrepancy in the numbers the Department has given of homes that have been closed since 2021.
The September 2023 DDS response to our Public Records request indicated that a net of 9 state-run homes were closed between August 2021 and September 2023, leaving 251 homes remaining.
However, data previously provided in January indicated that a net of 6 state-run homes were closed between August 2021 and January 2023, leaving 250 homes remaining as of January.
The implication of the January data was that 256 homes existed as of August 2021, whereas the implication of the September data was that 260 homes existed as of August 2021.
We have asked the public records supervisor to require DDS to account for the apparent difference between the two responses in the number of homes that existed as of August 2021.
DDS consistently maintains it has no records regarding the future of state-operated care
Despite the continuing downward trend in the census at Wrentham and Hogan, DDS said in January and again in September that they have no records concerning projections of the future census of those facilities or concerning plans to close them. Nevertheless, we maintain that unless DDS opens the doors at those settings to new residents, they will eventually close.
Violation of federal law not to offer state-run facilities
In a June 5 legal brief, DDS argued that federal law does not give persons with intellectual or developmental disabilities the right to placement at either the Wrentham or Hogan Centers. We think the Department’s argument in the brief misrepresents federal law, and reflects an unfounded bias among policy makers in Massachusetts against ICFs.
As Medicaid.gov, the federal government’s official Medicaid website, explains, “States may not limit access to ICF/IID service, or make it subject to waiting lists, as they may for Home and Community Based Services (HCBS)” (my emphasis). In our view, the federal Medicaid law and its regulations confer the right to the choice of ICF care to individuals and their families and guardians.
Meetings with state and federal lawmakers to bring these concerns to their attention
Last week, we met online with state Representative Jay Livingstone, the new House chair of the state Legislature’s Children, Families, and Persons with Disabilities Committee, to raise our concern about the declining census in state-run facilities and to discuss their vital contribution to adequate care in the system. We are similarly seeking a meeting with Senator Robyn Kennedy, the new Senate chair of the committee.
So far, we have also met online with legislative staffs of U.S. Senators Elizabeth Warren and Ed Markey, and of U.S. Representatives James McGovern, Lori Trahan, Catherine Clark, Seth Moulton, and Stephen Lynch, and have imparted that message. We still have four additional members to meet with in the Massachusetts congressional delegation.
In our meetings with the staff members of the congressional delegation, we are urging that the lawmakers oppose pending bills that would expand funding to the largely privatized, community-based system, but would not direct similar funding to either Wrentham or Hogan.
In sum, the data we have gotten from DDS have shown a consistent pattern by multiple administrations of building up the privatized DDS group home system while letting state-run residential facilities wither and ultimately die. As we’ve said before, we think that will result in a race to the bottom in the quality of care in the DDS system.
In our experience, state-run residential facilities in Massachusetts, as in most other states, meet higher standards for care than do privatized settings, and tend to have higher paid, better trained, and more caring staff. We want to bring that message to our state and federal legislators before it’s too late.
In ruling criticized as biased, DDS denies family’s request to place son at the Wrentham Center
As had been expected, Department of Developmental Services (DDS) Commissioner Jane Ryder last week upheld the denial of a request by a couple to place their intellectually disabled son at the Wrentham Developmental Center.
Ryder upheld a recommended decision by DDS Hearing Officer William O’Connell, who had previously denied a request by the couple to submit a COFAR blog post in rebuttal to a DDS closing brief in the case.
The COFAR post claims, among other things, that federal law gives individuals a right to care in an Intermediate Care Facility (ICF) such as the Wrentham Center.
The couple, who have asked that their names not be used, have sought the Wrentham placement as part of an appeal of their son’s Individual Support Plan (ISP). They contend the DDS-funded corporate provider that operates their son’s group home and day habilitation program does not provide services their son needs, such as nursing, speech and occupational therapy; and they note that these services are provided at Wrentham.
O’Connell’s 24-page recommended decision denying the couple’s appeal was dated July 20. The couple maintain that the language and reasoning in O’Connell’s decision confirms that he held a bias against them and in favor of DDS.
Son had been abused at day hab program and is facing eviction from group home
The couple also stated in their appeal that their son had been sexually and physically abused in his day hab facility. They further stated that the provider sought last September to evict their son from the group home after he had a toileting accident on the group home’s outside deck.
The eviction is currently on hold based on the couple’s objection to it under DDS regulations.
The couple said they are considering an appeal of O’Connell’s decision in state Superior Court. They said their hope is that a win in court would establish a precedent for other families seeking to place their loved ones with intellectual and developmental disabilities at either Wrentham or the Hogan Regional Center, the two remaining congregate ICFs in Massachusetts.
In ruling against the couple, O’Connell cited the testimony of two DDS regional directors during a hearing on the couple’s appeal in April. O’Connell stated that based on that testimony, he concluded that “the assessments and/or goals used to develop (the son’s) ISP…form a more than adequate basis for service planning for (the son), including his needs and treatments.”
O’Connell also stated in his decision that the son’s current services are “the ‘least restrictive’ to meet (his) current needs.”
O’Connell’s decision, however, largely did not address the couple’s contention that the actual services their son has received in his group home are inadequate.
Also, as COFAR pointed out in the blog post, which O’Connell would not allow to be submitted, “a statement that a community-based setting is necessarily less restrictive than an ICF is an ideological position that ignores the evidence.”
Hearing officer appeared to have a bias against the family
The couple further noted to us that the regional directors whose testimony was cited by O’Connell are bureaucrats who are largely unfamiliar with the day-to-day care of the son. Yet, the couple said, O’Connell clearly placed all of his credence in the directors’ testimony and not in their own testimony.
In his final decision, O’Connell used the term “credible” or “credibly” to describe the testimony of the two DDS regional directors at least 14 times, while repeatedly stating that the couple had “not met the burden of proof” and had not provided “probative evidence” to support their request that their son be placed at Wrentham. He didn’t explain why their evidence wasn’t probative.
The mother also told us that during the April hearing, O’Connell had expressed repeated impatience with her, telling her to “get to the point…” She said he never interrupted the DDS attorney.
O’Connell had also stated in his previous ruling that the COFAR Blog post was “not probative” as a reason for refusing to consider COFAR’s rebuttal to the DDS closing brief. The blog post would have required him to address several points including:
- That the federal Medicaid statute does provide a right and choice to individuals and their families to ICF care.
- That care at Wrentham and Hogan is not necessarily more restrictive than in provider-run group homes.
- That the couple’s son’s care in the community-based system has not been successful for the past 13 years, as the DDS closing brief stated, and O’Connell repeated.
- That DDS’s policy for many years of blocking new admissions to both Wrentham and Hogan is likely to result in the eventual closure of both of these vitally important backstops of care for some of the state’s most vulnerable residents.
In his decision, O’Connell also repeatedly stated that the couple had rejected all providers of community-based residential services that DDS had identified for them. But he did not acknowledge that the couple said they did so because they believe the community-based system has failed their son and will continue to do so.
ISP hearing process inherently unfair
COFAR has additionally questioned the fairness of the ISP appeal process, under which both the hearing officer is appointed by the DDS commissioner, and the commissioner then makes the final decision whether to uphold the hearing officer’s ruling. COFAR has called for such appeals to be decided by the state’s independent Division of Administrative Law Appeals.
Hearing officer discounted the impact of sexual and physical abuse of couple’s son
In his decision, O’Connell played down the impact of two incidents of sexual and physical abuse of the couple’s son, which the couple said were part of the reason they don’t believe the community-based system is safe or adequate for him. Both incidents had occurred in the bathroom of the day hab facility.
In one case in 2017, a staff member at the day hab program slapped the son on the head, punched him in the back, grabbed his genitals, and was verbally abusive to him over the course of several days.
In a second case in 2015, the son arrived from the day hab facility with a belt tightened so tightly that the parents couldn’t get it off. They said the belt was used to keep their son from going to the bathroom and moving his bowels. Their son has Crohn’s disease and needs to use the bathroom frequently.
According to the couple, their son cried and screamed when they tried to get the belt off. They said he had clear marks and indentations on his stomach which they photographed. In both cases, abuse was substantiated by the DDS investigations unit.
But O’Connell stated in his decision that:
I credit the (couple’s) concerns regarding (their son’s) well-being and safety given these terrible events, but find they were at day supports, not a residential placement, and thus do not have particular probative effect to the (couple’s) current appeal of the ISP and POC (Plan of Care).
O’Connell also stated, in line with the DDS closing brief, that the abuse happened five or more years ago.
But O’Connell didn’t mention that the same provider that runs the son’s day hab program also runs his group home. Also, there was no evidence presented by DDS or the hearing officer that abuse and neglect in the DDS provider system has become less prevalent in the past five years or that the abuse is unlikely to occur again.
Also, abuse in the provider system in general is not restricted to day programs, but occurs in residential settings. If the son were to be admitted to Wrentham, he would attend a day program there, where the abuse rate is likely to be lower than in the provider system.
We have found that abuse overall is lower in the ICFs than in provider run group homes.
Did not address specific services allegedly missing from the community
In a brief that they filed with their original appeal, the couple stated that there is no speech, occupational, recreational, or vocational therapy available to their son in his group home. The group home provider doesn’t provide those services, but Wrentham does.
The couple also stated that their son’s group home and day hab provider have not assigned a nurse to him or provided the name of a nurse to call in case a medical issue arises. They also said there is no nursing listed on his ISP or day hab service plan.
Also, the couple stated that no one at the group home “knows about (their son’s) health status at any given time.” For instance, they said, no member of the staff was aware their son was due for a colonoscopy in June.
The couple also maintained that in most doctors’ offices in the community, there are no accommodations for individuals like their son who have trouble waiting for long periods of time to be seen by the doctor.
O’Connell’s decision largely did not address these specific issues. However, O’Connell did respond to the couple’s contention that their son is not receiving the proper nursing care, writing that “DDS has indicated they will work with (the provider) and any subsequent residential agency to support (the son’s) specific nursing needs.”
The couple maintained to us, however, that saying DDS will “work with” the provider is a tacit admission that the service doesn’t currently exist, and is not an assurance that anything concrete will be done. Those nursing services, however, do exist at Wrentham.
O’Connell also stated that one of the DDS regional directors “credibly testified” that the couple had stated during an informal conference prior to the hearing that the son’s doctor is “excellent.” While that may be the case, the fact remains that the medical staff at Wrentham are highly trained to deal with people with intellectual disabilities, while medical staff in the community are not.
Also, O’Connell stated that the son’s difficulties in waiting at doctors’ officers “are common and easily managed by staff.” The parents disputed this, saying that if that behavior were easily managed, the problem would have been solved long ago.
Couple says son did not face discharge due to their actions
In his decision, O’Connell, once again adopting the DDS closing brief position, stated that the couple were notified last September that the son’s provider “was looking to discharge (him) from their residential placement services due to the (couple’s) actions, not due to any issue with (the son) or (the provider’s) ability to serve (the son).”
O’Connell did not say what those actions were that the parents allegedly committed. Moreover, the couple disputed O’Connell’s characterization of the matter. According to the couple’s original appeal brief, the incident that led to the discharge notice started when no staff were available in the residence to let their son inside to use the toilet.
The group home blamed the couple following the son’s accident on the group home deck, claiming they failed to clean up the area and failed to notify the staff about it. The couple dispute that charge, saying they used a sheet in their car to clean up the area and then emailed both provider and DDS officials about it.
The couple said there was one other incident that precipitated the discharge notice having to do with a Facebook post that the mother made that was critical of the staff of the group home. Neither of these incidents, in our view, are sufficient reasons to have issued a notice to evict the son. No details were provided in the hearing officer’s decision about either of those reasons for the discharge notice.
In sum, O’Connell’s decision in this case, in our view, shows exactly why the ISP appeal process is inherently unfair to families and guardians. His decision was entirely supportive of DDS’s position, and was entirely dismissive of the testimony and evidence put forth by the parents.
For the reasons the couple enumerated, we too hope they will win in court should they decide to appeal, and that this case would then set a precedent that might serve to save the Wrentham and Hogan Centers and other state-run residential programs and services from eventual extinction.
DDS hearing officer won’t allow COFAR blog post to be submitted as evidence in couple’s effort to place son at the Wrentham Center
A Department of Developmental Services (DDS) hearing officer has denied a couple’s request to submit a COFAR blog post to him for consideration as part of their appeal to place their son at the Wrentham Developmental Center.
The June 15 COFAR post claims, among other things, that federal law requires DDS to give individuals a choice of care in a facility such as the Wrentham Center. DDS primarily informs people looking for residential settings only of the existence of corporate provider-run group homes.
The couple, who have asked that their names not be used, requested that they be allowed to submit COFAR’s post in rebuttal to a DDS closing brief in the case. The DDS brief claimed that people with intellectual disabilities do not have a right to care at facilities such as Wrentham.
Last October, the couple appealed their son’s DDS Individual Support Plan (ISP) to the Department in an effort to have him placed at Wrentham. DDS held a hearing on the couple’s appeal on April 21 after the Department denied the requested placement. Under the ISP appeal regulations, the Department appointed a hearing officer in the couple’s case.
The hearing officer, William O’Connell, has not yet issued a decision on the appeal. His July 11 order denying consideration of the June 15 COFAR blog post stated that the post was submitted after his June 2 deadline for closing submissions in the case. However, O’Connell had previously extended that deadline to allow DDS to submit its closing brief on June 5.
Despite submitting its own brief under that extension, DDS subsequently opposed the couple’s request to have the COFAR rebuttal similarly entered into the record.
Hearing officer’s ruling is taken almost verbatim from DDS attorney’s objection
DDS’s written objection to the COFAR post described the post as “a late Rebuttal to the Department’s closing argument and brief,” and as “new evidence and argument that was not presented during the hearing or in the parties’ final closings.”
The DDS objection then stated that, “The (COFAR) evidence, a public opinion blog post, is of little probative value, and would likely not be admissible even if it were not filed late.”
Key portions of O’Connell’s written order about the COFAR blog post appear to have been taken almost word-for-word from DDS’s objection. O’Connell stated in his July 11 order that:
The (couple) submitted the rebuttal (COFAR post) well after the deadline for closing submissions had passed. Notwithstanding that the record was closed for evidentiary purposes at the close of the hearing on April 21, the proposed rebuttal to the DDS closing brief that the (couple) are attempting to submit as evidence and argument is a public opinion blog that is not probative and has no foundation for admissibility” (my emphasis).
Couple believes the hearing officer is biased against them
The couple maintain that O’Connell’s reliance in his order on the language in the DDS objection to the blog post appears to be evidence of a bias on his part in favor of DDS. They noted that he didn’t dispute any claim made in the post itself, but simply repeated DDS’s assertions about it.
The couple, who were not represented at the hearing by an attorney, also contended that O’Connell treated them with impatience during the April 21 hearing, and was deferential to DDS. “During the hearing, the hearing officer interrupted me several times and asked me to ‘get to the point,’” the wife said. “However, the DDS attorney was able to say her piece without interruption.”
The couple said they feel their case was “quite strong” at the hearing. But they said they are so certain their appeal will ultimately be denied by O’Connell that they are already planning their next move, which will be to take their case to state Superior Court to get their son into Wrentham.
If the couple are right about O’Connell’s likely decision, it will be interesting to see whether he primarily relies on the DDS closing brief in writing that decision, as he did with their request to submit our blog post into the record.
Unclear why DDS controls ISP appeal hearings
As noted above, DDS is in charge of the ISP appeal process, and even appoints the hearing officer who issues a recommended decision in each case. The final decision on the appeal is made by the DDS commissioner. We would agree that this creates, at best, a perception that the process is biased in favor of the Department.
We think the ISP appeal process should be decided by the independent Division of Administrative Law Appeals (DALA), which conducts appeal hearings for more than 20 state agencies, including the Disabled Persons Protection Commission (DPPC).
Hearing officer provided no support for claim that COFAR post was inadmissible
O’Connell stated that his order denying admission of the COFAR post was issued pursuant to the Massachusetts statute and regulations on adjudicatory practice and procedure (M.G.L. 30A and 801 CMR 1.02.)
We believe, however, that those rules would allow the post to be entered into the case record at any time, just as the DDS closing brief was entered after the hearing officer’s arbitrary closing date for submissions.
The regulations that O’Connell cited as underlying his ruling (801 CMR 1.02) constitute “informal rules” of adjudicatory procedure in Massachusetts.
Also, M.G.L.c. 30A, s. 11 states, with regard to the admissibility of evidence, that:
Unless otherwise provided by any law, agencies need not observe the rules of evidence observed by courts, but shall observe the rules of privilege recognized by law. Evidence may be admitted and given probative effect only if it is the kind of evidence on which reasonable persons are accustomed to rely in the conduct of serious affairs. Agencies may exclude unduly repetitious evidence, whether offered on direct examination or cross-examination of witnesses.
(3) Every party shall have the right to call and examine witnesses, to introduce exhibits, to cross-examine witnesses who testify, and to submit rebuttal evidence.
As we argue below, the COFAR blog post was intended to present evidence on which reasonable persons would rely in the conduct of serious affairs. It was not intended, as DDS and O’Connell casually dismissed it, to be a “public opinion blog.”
Both DDS and the hearing officer mischaracterized the nature of the COFAR blog post
As noted above, both DDS and O’Connell characterized the COFAR blog post as “a public opinion blog that is not probative and has no foundation for admissibility.”
However, the blog post directly rebutted the DDS assertion in its closing brief that federal law does not give persons with intellectual or developmental disabilities the right to placement at either the Wrentham Developmental Center or the Hogan Regional Center.
The post presented new evidence in the case regarding a succession of administrations in Massachusetts, which have allowed the residential population or census at the Wrentham and Hogan centers to decline. This decline, the post noted, has been due to DDS’s apparent policies of denying admission to those facilities to most persons who ask for it, and failing to inform persons looking for placements that those facilities exist as residential options.
We think the blog post therefore helped explain the almost automatic denial by DDS of the couple’s request to have their son placed at Wrentham.
Secondly, the blog post directly rebutted a statement in the DDS closing brief that the couple’s son currently lives in “a less restrictive community-based setting” than he would in an Intermediate Care Facility (ICF) such as the Wrentham Center.
The blog post then presented evidence that directly rebutted the DDS closing brief’s statement that the couple’s son “…has been successfully supported in the community for 13 years,” and that “he is well served by his community-based services and supports.”
Finally, the blog post revealed a misrepresentation in the DDS closing brief of the U.S. Supreme Court’s 1999 Olmstead v. L.C. decision with regard to institutional care. The post explained how the brief had wrongly implied that the Court had held that in all cases, individuals should be placed in community-based rather than institutional settings.
The statute that governs adjudicatory practice and procedure (M.G.L. c.30A, s.11), states that:
In all cases of delayed statement, or where subsequent amendment of the issues is necessary, sufficient time shall be allowed after full statement or amendment to afford all parties reasonable opportunity to prepare and present evidence and argument respecting the issues.
In our view, the couple were denied a reasonable opportunity to present evidence and argument in response to the evidence and argument in the DDS closing brief.
For all of the reasons discussed above, we believe the hearing officer erred in his denial of the couple’s request that the COFAR blog post be entered into evidence in their appeal.
DDS wrongly claims federal law does not give individuals the choice of either the Wrentham or Hogan Centers
In a June 5 legal brief, the Department of Developmental Services (DDS) argues that federal law does not give persons with intellectual or developmental disabilities (I/DD) the right to placement at either the Wrentham Developmental Center or the Hogan Regional Center.
We think the Department’s argument in the brief misrepresents federal law, and reflects an unfounded bias among policy makers in Massachusetts against Intermediate Care Facilities (ICFs). The Wrentham and Hogan centers are the last remaining, congregate ICFs in the state.
As we argue below, we also think the DDS brief wrongly assumes that group homes necessarily provide their residents with more integration with the surrounding community than do ICFs. That assumption is based on an outdated perception of the way ICFs operate today, and an overly rosy perception of the community-based system.
As we have reported, a succession of administrations has allowed the residential population or census at the Wrentham and Hogan centers to decline. This decline is due to DDS’s apparent policies of denying admission to the ICFs to most persons who ask for it, and failing to inform persons looking for placements that those facilities exist as residential options.
The DDS brief appears to confirm those policies in stating that:
DDS avoids institutionalization at the ICFs except in cases where there is a health or safety risk to the individual or others, and generally, when all other community-based options have been exhausted.
The DDS legal brief was submitted in response to an appeal to the Department, which was filed by the mother of a man with I/DD who was denied admission to the Wrentham Center. We are withholding the names of the mother and her son, at the mother’s request.
Federal Medicaid law requires a choice of either an ICF or “waiver services”
In our view, the DDS policies regarding admissions to ICFs do not comply with the federal Medicaid law and regulations. Those rules require that ICFs be offered as a choice to all persons whose intellectual disability makes them eligible for care under the Medicaid Home and Community-based Services (HCBS) waiver program.
Persons who are found to be eligible for HCBS waiver care have been found to meet the eligibility requirements for ICF-level care.
The HCBS waiver was established to allow states to develop group homes as alternatives to institutional care. However, the Medicaid statute did not abolish institutional or ICF care. In fact, the statute states that if a state does include ICFs in its “State Medicaid Plan,” as Massachusetts does, the state must provide that:
…all individuals wishing to make application for medical assistance under the (state) plan shall have the opportunity to do so, and that such assistance shall be furnished with reasonable promptness to all eligible individuals. [42 U.S.C. § 1396a(a)(8)]
Federal Medicaid regulations state explicitly that individuals seeking care, and their families and guardians, should be “given the choice of either institutional or home and community-based services. [42 C.F.R. § 441.302(d)] (My emphasis.)
The DDS brief, therefore, wrongly asserts that, “Federal law does not entitle the Appellant (the mother’s son) to admission to an Intermediate Care Facility.”
DDS brief wrongly assumes ICF settings are necessarily more restrictive than community-based group homes
The DDS brief also states, as a reason for denying admission to the Wrentham Center to the mother’s son in this case, that state regulations require the Department to place individuals “in the least restrictive and most community integrated setting possible.” According to the brief, the son currently lives in “a less restrictive community-based setting” than he would in an ICF such as the Wrentham Center.
But a statement that a community-based setting is necessarily less restrictive than an ICF is an ideological position that ignores the evidence.
This past Sunday, for example, I attended an annual birthday party for a DDS client who lives in a provider-run group home in Northborough. The home is located on a busy road. There is no sidewalk along the road, and only one other home in the area is faintly visible from the client’s residence.
There is no opportunity for the client to walk in the neighborhood around the residence, whereas residents at the Hogan and Wrentham Centers have access to acres of walking and recreational areas on the facility campuses.
While staff in the client’s Northborough group home do take him on trips to restaurants and other community events, those kinds of events are also provided, as our Board member Mitchell Sikora has recently described, to residents of the Wrentham and the Hogan Centers.
We’ve also written many times about restrictions imposed by DDS on visits and other types of contact by family members with residents of provider-run group homes.
The presumption that ICFs are necessarily more restrictive than group homes is based on an outdated characterization of facilities such as the Wrentham and Hogan Centers. Like many proponents of the privatization of DDS services, DDS chooses not to recognize the major improvements in congregate care and conditions that occurred, starting in the 1980s, in Massachusetts and other states as a result of both federal litigation and standards imposed by the Medicate statute.
DDS brief takes a we-know-best position
In addition to the questionable assumption it makes with regard to the level of restrictiveness of ICF care, the DDS brief also appears to accept, without question, that care and conditions in provider-run group homes are uniformly good.
The brief noted, for instance, that a DDS regional director had testified during a hearing in the case that the mother’s son “would not likely receive a greater benefit from admission to the ICF than he receives in the community.”
According to the brief, the son:
…has been successfully supported in the community for 13 years, his annual ISP (Individual Support Plan) assessments indicate that he continues to make progress toward his ISP goals, and he is well served by his community-based services and supports.
Conditions are not better in the community
Again, the DDS statements about what is best for an individual appear to be based on an ideological position that community-based placement options are always appropriate and available. In this case, however, the mother had sought to place her son at the Wrentham Center only after his group home provider had stated its intention to evict him from the residence.
The mother told us that in a meeting last year with DDS and provider officials, a provider manager cited two reasons for moving to evict her son. One was that her son had had a toileting accident on the deck of the group home, and that the mother had allegedly failed to notify the staff of the accident. The mother said the second reason was that she had posted a message on Facebook that was allegedly critical of the group home staff.
With regard to the toileting accident, the mother said she had taken her son back to the house after a planned outing, and that her son had the accident because the home was locked at the time and no one was there to let him in. Her son has Crohn’s Disease. The mother also said her son had also been physically abused on at least two occasions at the provider’s day habilitation facility.
Meanwhile, corporate group home and day program providers themselves in Massachusetts acknowledge that care and conditions in the DDS community-based system have been getting steadily worse.
In our view, all of this calls into question DDS’s assertion in the brief that the son in this case has been “successfully supported in the community for 13 years.”
DDS misrepresents the Olmstead Supreme Court decision
Finally, the DDS brief employs a common misrepresentation of the U.S. Supreme Court’s 1999 Olmstead v. L.C. decision with regard to institutional care. The brief wrongly implies that the Court held that in all cases, individuals should be placed in community-based rather than institutional settings. In fact, the Court held in Olmstead that three conditions must be met in order for persons to be placed in community-based care:
- The State’s treatment professionals determine that community-based placement is appropriate,
- The “affected persons” do not oppose such placement, and
- The community placement can be reasonably accommodated, taking into account the resources available to the state and the needs of others with mental disabilities.
The DDS brief, in arguing that Olmstead does not support the placement of the woman’s son at the Wrentham Center, cited only the first of the three conditions above. But all three conditions must hold under Olmstead in order to justify a placement in the community; and, clearly, the second condition doesn’t hold in this case — the affected persons do oppose continued placement in the community-based system.
In sum, the DDS closing brief in this case appears to provide the clearest indication we’ve seen of DDS’s reasoning and its policies with regard to admissions to the remaining ICFs in Massachusetts. It is clear to us that that reasoning and those policies are based on misinterpretations both of federal law and the history of congregate care for persons with I/DD in this state.
Unless the case can be made to key legislators and policy makers in Massachusetts that all family members and guardians should have the right to choose ICFs as residential options for their loved ones, the Wrentham and Hogan Centers will eventually be closed. If that happens, yet another critical piece of the fabric of care for many of the most vulnerable people in this state will be lost.
Retired Superior and Appeals Court judge writes about the care his brother receives at the Wrentham Developmental Center
[Editor’s Note: As we have previously reported, the number of residents remaining at the Wrentham Developmental Center and the Hogan Regional Center has continued to drop. As a result, these remaining, vitally important Intermediate Care Facilities (ICFs) in Massachusetts will eventually close if that decline is allowed to continue.
Mitchell Sikora, a member of COFAR’s Board of Directors, wrote the essay below about the importance of the Wrentham Center to his brother Stephen and himself, and submitted it to a member of U.S. Senator Ed Markey’s staff. We met last week on Zoom with one of the senator’s staff members to discuss our concerns about the future of the ICFs.
Mitch, 78, is a Massachusetts attorney and served as an assistant state attorney general for seven years; a private legal practitioner for 17 years; a justice of the Massachusetts Superior Court for 10 years; and a justice of the Massachusetts Appeals Court for 8 years. Since reaching the mandatory retirement at age 70, he has served as a voluntary mediator in the Superior Court.

Mitch and Stephen Sikora
We think Mitch’s account of the care that his brother receives at the Wrentham Center offers a clear explanation as to why ICFs are so important, and why eliminating those facilities as an option for care will be disastrous in Massachusetts.
It costs money to provide all of the specialists at Wrentham who care for Stephen and his fellow residents. But as we have seen, the closures of four of the six remaining ICFs in Massachusetts since 2012 has not resulted in a promised savings to the state. Over the past decade, the corporate provider-run group home line item in the state budget has grown from $760 million to $1.6 billion.
Moreover, We think Mitch’s list of recreational activities, both on-and-off-campus, that are provided to the residents at Wrentham debunks the myth that congregate-care facilities such as this one are institutional in character and warehouse or segregate those clients.]
My experience with ICFs in Massachusetts
By Mitchell Sikora
I am writing to report my experience with, and my support of, the continued operation of the remaining two ICFs for developmentally disabled residents of the commonwealth: the Wrentham Developmental Center in southeastern Massachusetts and the Hogan Regional Center in northeastern Massachusetts.
My younger brother Stephen, now 72 years old, has lived since age 10 at the Wrentham facility. The Center (originally named the Wrentham State School) has provided him with protection, care, affection, and community, especially since the major upgrade of all of the then Massachusetts state schools by federal district court litigation in the 1970s and 1980s, known collectively as the Ricci case and consent decree.
Since then, the Wrentham Center has functioned effectively as a campus village of concentrated human and physical resources benefitting Stephen enormously as he has aged.
I will do my best to describe the Wrentham Center’s human resources, its physical resources, and its communal benefits.
Human resources
The following personnel are assigned at the Wrentham Center to Stephen and each resident. A medical doctor oversees his health status. A nurse practitioner examines him promptly for any symptoms of illness. A daily staff nurse administers his medications and monitors his appearance.
His assigned social worker regularly visits him in his cottage dormitory and in socialization classes, and communicates her observations to us (his brother and sister).
A physical education specialist provides him with exercise at the Center’s gymnasium and swimming pool. A physical therapist has treated him for multiple orthopedic problems over the last 20 years, including knee replacements from arthritis, and hip and pelvic fractures from falls.
Vocational instructors have trained him to perform (to his own satisfaction) simple useful on-campus work, such as the collection and delivery of recyclable papers and objects. A recreational therapist periodically takes him for off-campus trips and treats, such as a stop at MacDonald’s. A psychologist responds to any episodes of behavioral or mood problems. A nutritionist watches his diet.
The Center also supports a “service specialist” program in which retired employees contract with families to take residents for off-campus rides or on trips to the families’ homes. Typically, the service specialists are familiar with the resident from years of work at the Center. With the fading of the COVID pandemic, the service specialist process can now resume.
Once each year, the Center must conduct a conference with each family to maintain and update the resident’s ongoing Individual Service Plan (ISP). The continuous Plan describes the resident’s health, activities, progress, problems, goals, needs, and spending objectives for the past and oncoming year. The Plan typically approximates 25 pages. The majority of the personnel enumerated above participate directly in the Conference (conducted by Zoom during the pandemic years) or contribute to the Plan.
As a final word about human resources, I should add that over the past 20 years, the Wrentham Center has received the dedicated service of three longtime facility directors and the involvement of devoted members of the Wrentham Family Association.
Physical resources
The Wrentham Center occupies a campus landscape of approximately 20 square blocks surrounded largely by open fields. The grounds include walking paths and picnic tables. The residents live in large cottages or small dormitories, each with a capacity of six to ten occupants.
Each resident has his or her own room. The communal bathrooms (with advanced shower facilities), kitchen, dining, and TV rooms are large and clean. Direct care workers are present at all times.
The campus contains a freestanding health care facility, the May Clinic, comprised of about 10 beds, three or four fulltime nurses, and visiting physicians. The Tufts Dental School maintains an office in the clinic.
The Wrentham Center has standing relationships with a number of hospitals, including New England Baptist for orthopedic care, and Brigham and Women’s Hospital, Sturdy Memorial Hospital, and Norwood Hospital for urgent and general care.
The campus buildings include a modern school structure of classrooms and meeting rooms; a gymnasium; a swimming pool; a canteen/snack bar; and two administrative buildings. Eight to 10 pre-1980s brick dormitories now long-abandoned remain scattered across the campus. The general setting is expansive and tranquil.
Communal benefits
A number of activities get the residents up and out of the cottage or dormitory:
- Physical ed classes at the gymnasium and pool. Classes at the school building in adult education, vocational education, and speaking skills.
- Day trips off campus to recreational parks, sports events, and the inevitable snack shops.
- The campus-wide Christmas decorations and party.
- A campus-wide spring celebration.
- A late summer week long country fair on campus conducted by a professional amusement company.
- Summer vacations of 3 or 4 days off campus conducted by staff and financed by families able to do so, or by the Center.
- The above mentioned service specialist program.
In all these activities the continuity and affection of the Center’s employees play a crucial role. Some of my brother’s caregivers have known and served him for more than 30 years.
My apologies for the length and detail of this message. I hope that it demonstrates the role of a well functioning ICF as a healthy community and home for its residents. It can serve as a unique concentration of both professional competence and elemental compassion.
A while back an old adage made a comeback: “It takes a village to raise a child.” I have thought that it applies even more so to the care of the developmentally disabled. At the very least, the families of the disabled deserve the informed choice of placement of their member in a well functioning ICF.
Since the great upgrade of the ICF system in the 1980s, the state has progressively reduced information made available to the public about the availability of the ICFs so that now only two ICFs remain in operation in Massachusetts. Those two facilities are subject to declining enrollment.
Post-Ricci administrations appear to retain a pre-Ricci vision of the care and conditions in the ICFs. That approach appears to have become dogmatic policy. It seems to me wrong upon several grounds. First, it is factually inaccurate and outdated. Second, it deprives applicant families of the opportunity of an informed placement choice. Third, it appears to violate requirements of both federal and state law that individuals and their families and guardians be able to make informed decisions about all available placements.
The federal Medicaid law and regulations require that individuals determined to be likely to need ICF-level care be informed of “the feasible alternatives” to that care, but also “given the choice of either institutional or home and community-based services.” [42 U.S.C.§ 1396n, and 42 C.F.R. § 441.302(d)].
However, as COFAR has often reported, families and guardians are generally not informed of the existence of the Wrentham or Hogan Centers. As such, those families and guardians are not being given the information or choices specified by the federal requirements.
Similarly, the Massachusetts Department of Developmental Services (DDS) regulations call for “informed consent” for admission to any departmental facility, including an ICF or group home. [115 CMR 3.04.] I suspect that additional sources of law and context would fortify the inherently fair and rational standard of informed consent and choice.
Faithful compliance with the legal standard of informed choice requires DDS to provide a family in need of a placement with a clear and explicit description of the ICFs and their resources and activities, and, if requested, with visiting tours of those facilities.
I hope that these thoughts are useful. Please do not hesitate to contact me for more information. Email: mitchsikora@gmail.com.
