Archive
A mother’s lonely battle for appropriate care for her son
Valerie Loveland has felt as though she has had to fight alone to protect her son from indifferent care and even abuse in the Department of Developmental Services (DDS) system.
Her decisions were questioned, she says, not only by the staff in her son’s previous group home in Cotuit, but by DDS officials and even the DDS-paid co-guardian for him.
At times she has feared that her own co-guardianship of her son might be taken away. (Although she wants her son’s story told here, she requested that his name not be used.)
In addition to other issues she has had to deal with, the state’s response to alleged sexual abuse of her son in March of this year in the group home seems to have been shrouded in secrecy.

Valerie Loveland
Even as co-guardian, she has not been allowed to view the complaint filed in the matter. She has been told only that her son was allegedly sexually abused by a group home staff member, but not what happened.
Tide may have turned
The good news is that in the past few weeks, the tide seems to have turned in her son’s favor.
Although Valerie was not able to get her son into a state-operated group home, as she had hoped, the May Institute did place him earlier this month in a new residence, also in Cotuit. And she said the new group home staff is making an effort to follow her requests to improve her son’s diet, which she said is linked both to his health and his behavior. The staff are also carrying out his occupational therapy plan.
For Valerie, it has all been about introducing common sense to her son’s care. “Maybe we should change what he’s getting to eat,” she said, citing an example. “That might actually save the state money on doctors visits, damage to the residence etc. That’s why I’ve been in their face.”
But as is so often the case, common sense does not prevail in the DDS system. Valerie’s case demonstrates how family members in the system frequently find themselves pitted against providers, clinicians, probate court judges, and bureaucrats. The family members’ concerns and wishes for their loved ones are too often disregarded or overridden.
Valerie’s son, who is 23, has an intellectual disability, is non-verbal, and needs 24-hour care. He has now been a resident for the past five years in three separate group homes on Cape Cod run by the May Institute.
Valerie said DDS had attempted to remove her as her son’s guardian when he turned 18, but then agreed to the co-guardianship arrangement. The other co-guardian is an attorney who is paid by DDS and who has other wards as well.
She said there had been problems in the previous Cotuit-based group home with cleanliness and thefts of her son’s electronic devices that help him communicate. In March, her son was allegedly sexually abused by a staff member of the group home. The incident was apparently reported to the Disabled Persons Protection Commission (DPPC) by another staff member.
Valerie has been told that DPPC is still investigating as are police. Her request to DPPC for a copy of the written complaint in the case was denied because the investigation is still underway.
Son’s care has taken a financial toll
After the alleged assault, Valerie removed her son from that group home and cared for him at home. He was placed in the new May Institute group home in Cotuit on June 19.
Valerie, who lives in Chatham, estimates that it has cost her thousands of dollars in lost income to care for her son at home and drive him each day to his day program in Mashpee.
Valerie works in grocery delivery and part-time in aromatherapy, and is working for a college degree in alternative medicine. She said the DDS-paid co-guardian has largely been uninvolved in her son’s physical care, but criticized her decision to remove her son from the group home in which he was allegedly abused.
She and her ex-husband were divorced in 2002. She said her ex-husband has been completely uninvolved in her son’s life and hasn’t seen him since her son was about 2 or 3 years old. Valerie cared for her son at home until he was 18. Her ex-husband owes her child support, she said, but has disappeared. Even private investigators, including one hired by the state Department of Revenue, haven’t been able to find him.
May Institute executives well compensated
Despite her tenuous financial situation, Valerie has had to deal with a system dominated by well-paid corporate executives and powerful state officials. The May Institute’s Fiscal Year 2019 tax filing with the IRS listed a dozen executives of the nonprofit organization as having received more than $100,000 each in salary and other compensation that year.
That list was topped by May Institute President and CEO Lauren Solotar, who received almost $477,000 in total compensation, followed by the COO, who received close to $331,000. Five other executives made more than $200,000 each.
COFAR President Thomas J. Frain maintained that with compensation levels that high, the May Institute’s executives should be held accountable for ensuring that all of its clients receive adequate and appropriate care.
Instead, Valerie said it is only now that she feels the organization understands and is responding to her son’s needs.
Saw diet as cause of problems
Valerie said that while her son was at the first May Institute group home in Cotuit, his aggressive behaviors started to escalate, including banging his head against walls and tearing up his mattresses. She said the group home tried to bill her for the expenses; but, as his Social Security representative payee, she argued that the staff needed to try to understand his behavior.
Valerie maintained that dietary changes that she insisted upon reduced the head-banging. Those dietary suggestions included giving him whole foods, including fresh vegetables, fruits, and whole-grains and essential oils supplements.
Until recently, there was resistance to her efforts, even from the other co-guardian. As late as May 31, the other co-guardian stated to her in an email: “Instituting a diet change for anyone is a major step. Especially if the reason is not medically required.”
Prior to her son’s placement in his new group home, the May Institute residential director for Cape Cod wrote to Valerie on June 2, saying the provider would not be able to meet her dietary requirements for her son.
That has lately changed, Valerie said. The new group home staff appear to be making an effort to follow those requirements.
Pushback on other efforts to protect son
Valerie said that over the past year, she encountered pushback from the provider, the co-guardian, and DDS to other efforts she was making to protect her son. Those included her initial efforts to remove her son from the first group home, even after the abuse allegation surfaced.
Valerie said she asked DDS several times after learning of the March abuse allegation about moving her son to another group home; but the area office said nothing was available due to the COVID crisis. As a result, she said, she took her son home with her.
In a May 25 email, the DDS-paid co-guardian stated, “I trust the May Institute and its staff to be working for the best for (her son). I am not in favor of looking for another residential placement… I am unaware of any other residential program that would accept (her son) or be in his best interests.”
As late as June 2, the co-guardian said he continued to “fully object to his (her son’s) removal from May until a response from DDS is obtained.”
Valerie claimed that as recently as a month ago, the co-guardian threatened in group meetings with DDS and the provider to have her removed as co-guardian. “He said he would take me to court to have me removed,” she said. She added that during those meetings, “no one from DDS or May said a word” in response.
Valerie said the co-guardian finally relented regarding removing her son from the first group home, and earlier this month approved his move to the new residence.
Denied use of bathroom
When the May Institute finally suggested the new group home for her son, Valerie took on the task of easing the transition for him to the new residence. She drove him to the new residence on May 26 to help him get acquainted with it and with the residents and staff.
But she herself wasn’t allowed inside, even to use the bathroom after the hour-long drive from her home in Chatham.
The reason given for denying her entry to the residence was the COVID crisis. But both she and her son were vaccinated, and her son was allowed inside even without a mask.
“I didn’t understand why I couldn’t run in and use the bathroom,” she said. “I wasn’t asking to stay inside. I was asking for toilet facilities. It seemed unreasonable to me.”
When Valerie later wrote to May Institute officials to complain, the May institute residential director responded that, “At this time, indoor visitation is not approved under state guidelines.” But that was not the case according to the DDS guidance, dated March 19, which was then in effect.
The DDS visitation guidance gave the providers discretion regarding indoor visits, stating that any restrictions should not be arbitrary. COFAR reported in May that many DDS group home providers were continuing to impose highly restrictive visitation requirements on family members even if all of the residents had been vaccinated.
Since her son moved into the new group home, Valerie said the residential staff has allowed her inside.
Valerie said she is hopeful that a new era of common sense-based care has begun for her son in his new group home. But she said she is mindful of the difficulties she has faced and the long road she has traveled to get him to this point.
She also recognizes that although the situation today for her son appears better than it was a few months or even weeks ago, that could change.
“I think it’s important for people to understand this type of situation isn’t a ‘one and done’ for a complex kid like my son,” she wrote to us. “His being nonverbal has been a big challenge for him and staff. I’ve been the bridge. I won’t always be here. I keep trying to figure that part out…”
COFAR and AFSCME warn that President Biden’s HCBS expansion plan could harm ICFs
COFAR has joined with AFSCME Council 93, a key Massachusetts state employee union, in warning that President Biden’s proposed $400 billion expansion of home and community-based services for people with disabilities and the elderly could pose a threat to the future of state-run services.
In a jointly written letter to U.S. Senator Elizabeth Warren, COFAR President Thomas J. Frain and AFSCME Council 93 Executive Director Mark Bernard expressed overall support for Biden’s proposed expansion of access to affordable home and community-based services (HCBS) for people with I/DD and the elderly.
But the letter noted that Biden’s plan fails to similarly propose any additional funding for state-run Intermediate Care Facilities (ICFs) for persons with I/DD and complex medical needs.
Expanding only HCBS, the letter said, would pose “a serious threat to the future of critically important ICF-level care in this country…(and would) interfere with the ability of individuals, particularly those with severe forms of I/DD, to access the residential settings and programs that meet their needs.”
Biden’s $400 billion HCBS expansion plan is part of his $2 trillion American Jobs Plan, a proposal to Congress to rebuild the American economy and the nation’s infrastructure.
The two remaining state-run ICFs in Massachusetts are the Wrentham Developmental Center and the Hogan Regional Center in Danvers.
Steering increased funding only toward community care would create a strong incentive for Massachusetts to close the Wrentham and Hogan facilities, the AFSCME-COFAR letter stated.
In addition to stripping the DDS system of a badly-needed component of the continuum of care for the developmentally disabled, the closure of the ICFs would jeopardize the jobs of approximately 1,400 union workers represented by AFSCME alone.
ICFs provide needed choice
The joint letter noted that choice in care is only meaningful if individuals are given access to the services that they need and prefer. As the United States Supreme Court held in the 1999 Olmstead v. L.C. case, there must be a recognition that, on a case-by-case basis, that setting might be in an ICF.
But the Massachusetts DDS does not routinely inform either individuals or their families who are waiting for residential placements even of the existence of either ICFs or state-operated group homes. The only “choices” routinely offered are corporate provider-run group homes or, in some cases, shared living arrangements. As such, families do not have a real choice along a full continuum of care.
The number of residents at the Wrentham and Hogan ICFs and in state-operated group homes has been declining in Massachusetts for several years. State funding for state-operated services has also been flat or has declined over the past decade.
In contrast, funding has skyrocketed for corporate, provider-run group homes. Successive administrations have long engaged in a race to privatize DDS services.
Calling for parity
The joint letter noted that In Fiscal Year 2019, Medicaid spending nationwide was $76 billion for HCBS and $9 billion for ICFs. Out of total Medicaid spending nationwide for long-term supports and services, 59% was spent on HCBS and 7% on ICFs.
If the Massachusetts Legislature concurs with Governor Baker’s proposed funding for DDS for Fiscal Year 2022, the corporate provider line item will be funded at more than $1.4 billion. That would represent a 91% increase over the funding appropriated for the same line item a decade previously, in Fiscal 2012.
In contrast, funding for state-operated group homes and the two remaining ICFs has been on a relatively flat or downward trajectory respectively.
When adjusted for inflation, the governor’s Fiscal 2022 budget would cut funding for state-operated group homes by somewhat less than 1% from the current fiscal year. The Wrentham and Hogan centers would similarly see their funding cut in Fiscal 2022 by a total of $2.1 million. Since Fiscal 2012, funding for the developmental center line item will have been cut by 32%.
The joint letter stated that the ongoing under-funding of state-run DDS programs has resulted in the increasing privatization of those programs and services.
Massachusetts State Auditor Suzanne Bump’s office reported in 2019 that while the resulting boost in state funding for privatized care produced surplus revenues for corporate providers, those additional revenues led to only minimal increases in wages for direct-care workers.
Disparity in care
The joint letter stated that In 1993, then U.S. District Court Judge Joseph L. Tauro ordered that ICFs in Massachusetts not be closed unless it was certified that each resident would receive equal or better care elsewhere. Judge Tauro was bringing an end to a landmark consent decree (Ricci v. Okin), which had resulted in major upgrades in care and services in the DDS system.
As the years went on, however, the promise of equal or better care in the community was not realized. Deinstitutionalization has turned out to be fraught with problems for people with I/DD just as it has for people with mental illness.
In testimony in 2018 to the state Legislature’s Children, Families, and Persons with Disabilities Committee, Nancy Alterio, executive director of the Massachusetts Disabled Persons Protection Commission (DPPC), stated that abuse and neglect in the DDS system had increased 30 percent in the previous five years, and had reached epidemic proportions.
Yet many advocates for corporate providers, such as the Arc of Massachusetts, have pushed for decades for complete deinstitutionalization and for additional privatization of services for people with I/DD. They have been joined by administrations at the state and national levels, which have continually made state-run care and services targets for closure and outsourcing to contracted providers.
Since 2009, the U.S. Justice Department has filed, joined, or participated in lawsuits around the country to close ICFs regardless of whether the residents or their families or guardians wanted to close the facilities they were living in or not.
Olmstead did not call for the closure of ICFs
The late U.S. Supreme Court Justice Ruth Bader Ginsburg wrote the majority opinion in the Olmstead case (referred to above). The decision has continued to be mischaracterized as advocating or requiring the end of institutional care. It didn’t. Justice Ginsburg wrote a balanced decision that “supports both the right to an inclusive environment and the right to institutional care, based on the need and desires of the individual.”
The incestuous nature of the privatized system
The closures of ICFs around the country and the rise of the privatized system of care have provided financial windfalls for politically connected corporate contractors. Their executives have garnered large increases in their personal compensation, but have frequently neglected to pass through the higher levels of state funding to direct-care workers. That is one of the reasons for the epidemic of abuse and neglect in the corporate provider-based system of care.
In 2015, COFAR calculated that more than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation. By COFAR’s calculations, state taxpayers were on the hook each year for up to $85 million of that total compensation.
What we are asking for
The COFAR-AFSCME letter asked for Senator Warren’s support in achieving the following goals:
- Parity in public-sector funding for ICFs and other state-run services with funding for privatized services. The letter suggested that an increase in the federal Medicaid match for HCBS should be matched by an increase in matching funding for ICFs. For example, a 10-percentage point increase in the federal match (FMAP) for ICFs would be roughly $1 billion nationwide.
- Ensuring a dedicated funding stream for state-operated group homes for individuals with I/DD.
Yet another corporate DDS provider is slapped by a state audit
The Berkshire County Arc is one of the the latest in a series of corporate residential providers to the Department of Developmental Services (DDS) that have found themselves targets over the past two decades of the state auditor for misuse of state funds.
A few other examples include audits of Brockton Area Multi Services just this week; Human Service Options and Nonotuck Resource Associates in 2016; the May Institute in 2013; Crystal Springs in 2012; and Toward Independent Living and Learning in 2002.
From personal use by corporate executives of the Berkshire Arc’s credit cards to personal use of its frequent flyer airline miles, the problems cited in the Berkshire Arc audit sound almost monotonously familiar.
The Berkshire Arc and its lobbying affiliate, the Arc of Massachusetts, have hit back, arguing that many of the audit findings were technical in nature.
To be sure, the Berkshire Arc audit does have at least one finding that seems to imply a largely technical violation involving the financing of capital improvements and maintenance of residential and other properties. The Berkshire Arc shouldn’t have charged the state for that, the audit said, because the properties are technically owned by another nonprofit affiliated with the Berkshire Arc.
That violation seems technical because it seems that the Berkshire Arc’s clients did potentially benefit from the capital improvements.
But other findings about misuse of credit cards and airline miles were clearly about people in high-level management positions allegedly benefiting themselves personally. One would think that after decades of these kinds of audit findings, the heads of these organizations would finally put an end to these practices.
“Our audit makes clear that those in leadership fell short of meeting their oversight and fiduciary responsibilities,” State Auditor Suzanne Bump said in a press release.
But it seems these kinds of problems will likely continue to occur in a system that has seen care for persons with developmental disabilities largely handed over to corporate contractors to DDS. It’s a system in which DDS itself and other regulatory agencies appear to constantly fall short of their own oversight responsibilities.
The Berkshire Arc received over $25 million in funding in Fiscal Year 2019 from state agencies including DDS, the Massachusetts Rehabilitation Commission, and the Commission for the Blind, according to the audit.
Among other problems cited by the audit, the Berkshire Arc allegedly used its credit cards to pay $124,247 in expenses that were non-reimbursable under its state contracts because they were inadequately documented, were not related to the organization’s social service program activities, or were luxury items otherwise prohibited by state regulations. Those items included valet parking, priority boarding, main-cabin extra seating on airlines, and alcohol.
The Berkshire Arc responded that the extra main-cabin seating was purchased so an individual with disabilities could attend a national self advocacy conference in 2018. But the audit stated that the supporting documentation that the Berkshire Arc provided indicated that the extra cabin seating was purchased by and for the organization’s chief operating officer, with no indication that it would be used by one of the clients.
The audit found that Kenneth Singer, the Berkshire Arc’s president and CEO, used credit card reward travel miles earned by the organization for his personal use in violation of state regulations and the organization’s own policy. The audit alleged that “at a minimum,” Singer redeemed miles earned by the Berkshire Arc on agency credit cards to pay for trips made for personal reasons to Hawaii and Mexico.
As a result of this issue, the audit stated, the Berkshire Arc “lost the opportunity to reduce its travel costs…(and) the money saved could have been used to provide additional services to its clients.”
The auditors also determined that Singer’s wife, Christine, who was working as a consultant to the Berkshire Arc, used the organization’s credit cards for $2,057 in trips, meals and gifts for a Berkshire Arc conference. Further, the audit noted, the Berkshire Arc charged its client funds accounts $43,192 in credit card purchases for which it did not have the required documentation.
In what seems to be the technical violation, the auditor said the Berkshire Arc paid for $487,341 in capital improvements to properties owned by a related party. The audit claimed those expenses were for assets that were not owned by Berkshire Arc and were therefore not program-related.
The Berkshire County Arc’s response was that its properties are “100% occupied and utilized by Berkshire County Arc for residential services, day services, programming, and operations.” It doesn’t appear that the audit questioned or contradicted that assertion.
The audit recommended, among other things, that the Berkshire Arc establish monitoring controls on all credit card expenses before payment, and that the organization “properly identify and correctly report all non-reimbursable expenses.”
We’re glad the state auditor is periodically reviewing the books of DDS providers, and making recommendations for correcting the deficiencies in financial management. The Berkshire Arc, in particular, also pledged to revamp some of its bookkeeping and management practices.
But what is needed is a more comprehensive review of the DDS system as a whole to address the patterns of faulty management that seem endemic to the system given that they keep coming up again and again in the audits. It is somewhat disappointing that these audits are done piecemeal. We have long called for a comprehensive investigation of the DDS system in Massachusetts.
If nothing else, the continuing series of piecemeal findings by the state auditor of mismanagement among providers shows just how much such an investigation is needed.
Proposed commission on former DDS state schools needs to acknowledge upgrades in care
The history of state-run institutions in Massachusetts for persons with intellectual and developmental disabilities is critically important for us to know.
That’s why we support legislation in concept that would establish a commission (S.1257and H. 2090) to study the controversial and often dark history of the state schools.
At the same time, we are pushing for changes in that legislation to ensure that the commission recognizes the significant upgrades in care and services that occurred in those facilities in the 1980s. Those changes were primarily due to Ricci v. Okin, a landmark federal consent decree case overseen by the late U.S. District Court Judge Joseph L. Tauro.
In that regard, the proposed commission needs to recognize that the Wrentham Developmental Center (WDC) and the Hogan Regional Center in Danvers — the state’s two remaining developmental centers or Intermediate Care Facilities (ICFs) — provide state-of-the-art care and services today. We don’t want to see the commission used as a political cudgel to attack ICF-level care in Massachusetts.
The ICFs of today are not the same institutions that were subject to the Ricci v. Okin litigation, which had sought to correct horrendous warehouse-like conditions in them. Nevertheless, ICFs have remained political lightning rods for advocates of deinstitutionalization and privatization of remaining care and services for the developmentally disabled.
For that reason, we want to make sure that the proposed membership of the commission and its written charge will not lead to a preordained conclusion that leaves out the history of these facilities after Judge Tauro’s intervention. To help ensure a balanced review by the commission, we are seeking additional seats on the panel for family members and guardians of current residents of WDC and Hogan.
Statements made by some key supporters of the commission have presented the former Fernald Developmental Center and other state-run congregate care facilities in a negative light. It also appears that the makeup of the commission, as currently described in the legislation, would primarily consist of opponents of ICFs and supporters of further privatization of DDS services.
COFAR has contacted Senator Michael Barrett and Representative Sean Garballey, the prinicipal sponsors of the legislation, to express our concerns.
We do support efforts, as described in the bill, to study the past history of institutional care in Massachusetts, and we agree with the premise of the legislation that records on these facilities are scattered and should be organized. We also strongly support efforts to identify persons buried in unmarked graves on the grounds of some of the former facilities.
As noted, however, a complete history of the state facilities in Massachusetts should include Judge Tauro’s assessment of the developmental centers in 1993, as he disengaged from the Ricci case. He noted that improvements made to the facilities as well as community placements had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
Alex Green, a key proponent of the commission, recently told Colleen M. Lutkevich, COFAR’s executive director, that he is sensitive to our concerns and will advocate for changes to the makeup of the panel.
The bill currently specifies that representatives of the Arc of Massachusetts, the Disability Law Center, Mass. Advocates Standing Strong, Mass. Advocates Organizing for Change, and the Center for Independent Living would be appointed to the commission. All of those organizations are on record as supporting the closure of ICFs in the state.
The bill also states that additional “community members” and former members of state institutions would be given seats on the commission. But the measure doesn’t recommend seats for current residents of either WDC or Hogan, or their family members or guardians.
We think the perspective of those current residents and their families and guardians is needed to provide a full understanding of how the ICFs function today.
In a written statement provided to COFAR, Green said he is seeking to amend the legislation to add two seats for “facility families–whose experiences deserve representation.” He said he will also seek to add a third seat “for another participant with an intellectual disability, ensuring that the composition of the commission adheres to the intent of being a majority of people with disabilities.”
Green added that, “Many of these families and individuals were part of the civil rights movement that led to the (Ricci v. Okin) consent decree, and also ensured that its implementation resulted in an unprecedented overhaul of, and investment in, these facilities.”
We support adding those seats, but would note that even with three seats on the commission, it would appear that pro-ICF members would be vastly outnumbered by proponents of privatized care.
Green said there were 27 groups “and hundreds of citizens signed on in support of the passage of these bills (the House and Senate versions of the legislation), along with co-sponsorship from 10% of the Legislature. Collectively, these individuals and groups represent hundreds of thousands of disabled people across the Commonwealth.”
Green added that, “COFAR’s support means that important amendments will be made to the bills, helping to ensure that a full, expansive, accurate understanding the consent decree era is included.”
Commission’s written charge needs to be expanded to recognize ICFs today
In addition to specifying that there would be current facility family members on the commission, the language in the legislation needs to be changed to specify that the commission will assess the quality of life of current residents of the Wrentham and Hogan Centers. The legislation, as currently worded, only refers to assessing the quality of life of “former residents (of state institutions) now living in the community.”
The quality of life of both current and former facility residents needs to be assessed in order to present a balanced view of Wrentham and Hogan today. Similarly, the bill language currently only requires that the commission “collect testimonials” from former institutional residents. It does not contain the same requirements regarding current residents. Again, those assessments and testimonials from current residents are needed for that full understanding.
“If we don’t talk about the success story that is Wrentham and Hogan today, it’s not telling the whole story,” Lutkevich said.
It’s important that we get the history of the state facilities right. That’s because we think that in many ways, the warehouse conditions of the institutional system prior to the 1980s are continuing today in many community-based, privatized settings. We hope that sometime in the not-too-distant future, a commission will be established to study that situation.
State House approves cuts to DDS day program funding, increases for provider group homes
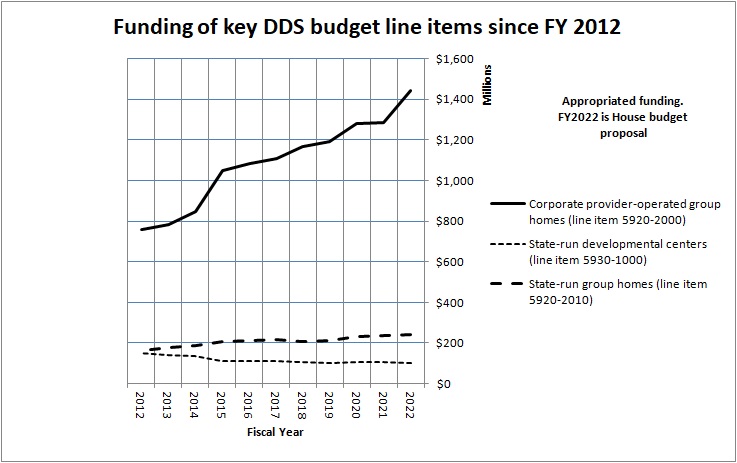
The House budget would add $100,000 to the governor’s proposed Fiscal 2022 funding for state-operated group homes (line item 5920-2010). However, when adjusted for inflation, even the House budget proposal would amount to a cut in funding for this line item of somewhat less than 1%. (We are basing that assessment on numbers from the Massachusetts Budget and Policy Center’s “Budget Browser.”)
The two remaining developmental centers would similarly see their funding cut in Fiscal Year 2022 by $2.1 million under the House budget, when adjusted for inflation (line item 5930-1000). Since Fiscal 2012, funding for the developmental center line item will have been cut by 32%.
COFAR is continuing to raise concerns regarding the ongoing under-funding of state-run DDS programs. We believe this has led to unchecked privatization of programs and services.
We are also concerned that even within provider accounts, we may be seeing a permanent pullback in funding for day programming, with much of that funding ultimately going to provider-run group homes.
Last month, we sent an issue paper raising those concerns, among others, to Senator Adam Gomez and Representative Michael Finn, the new chairs of the Legislature’s Children, Families, and Persons with Disabilities committee. You can find our issue paper here.
Congress still trying to eliminate congregate care for developmentally disabled
In their latest attempt to do away with congregate care for persons with intellectual and developmental disabilities and promote further privatization of services, lawmakers in Washington have proposed the Home and Community Based Services Access Act (HCBS Access Act).
While we support the intent of this legislation to eliminate waiting lists for disability services, the bill’s provisions are heavily biased against congregate care facilities such as the Wrentham Developmental Center and the Hogan Regional Center in Massachusetts. The bill is also biased against sheltered workshops and other programs for people who are unable to handle mainstream or community-based settings.
In that regard, this legislation is similar to the federal Disability Integration Act of 2019, which ultimately did not pass in the previous congressional session.
While we think it was good news that the Disability Integration Act didn’t pass, the bad news is that many in Congress, including most, if not all, of the Massachusetts delegation, appear to subscribe to the notion that community-based or privatized care is the only appropriate option for people with cognitive disabilities.
Every member of the Massachusetts delegation signed on to the Disability Integration Act, which would have encouraged further unchecked privatization of human services, diminished oversight, and reduced standards of care across the country. The HCBS Access Act would do so as well.
Comments are due April 26 on the HCBS Access Act, which has been proposed by Representative Debbie Dingell (D-MI), Senator Maggie Hassan (D-NH), Senator Bob Casey (D-PA), and Senator Sherrod Brown (D-OH). Comments can be sent to HCBSComments@aging.senate.gov.
We will also be urging the members of the Massachusetts delegation to take another look at the issue of congregate care, and reassess their positions.
The HCBS Access Act actually appears to go a step beyond the Disability Integration Act in that it would potentially eliminate funding for Intermediate care facilities (ICFs), including the Wrentham and Hogan Centers. Currently, the federal government pays 50% of the cost of care in both ICFs and community-based group homes. The state pays the other 50% of the cost.
The HCBS Access Act would change that federal-state funding formula to require the federal government to pay 100% of community-based group home costs. The federal share of the cost of ICFs would remain at 50%. That would place enormous pressure on states to eliminate ICFs since they would continue to receive only 50% federal funding.
As the National Council on Severe Autism (NCSA), a nonprofit organization, noted in comments on the HCBS Access Act, ICFs are “a key component of the national safety net.” The organization pointed out that it is a “fiction” that all community-based settings are better or safer than settings labeled as “institutional.”
“’Community services’ in reality often mean no supervision, no licensing, no consulting medical or nursing personnel, no properly trained staff to handle medical/behavioral crises, high burnout and turnover,” the NCSA stated in its comments.
Among the many unanswered questions involving the HCBS Access Act are how the federal government would pay the cost of 100% reimbursement of all community-based care.
The NCSA made a number of additional observations about the legislation, including the following:
- The bill is based on a “false assumption that the Medicaid system contains an ‘institutional bias’ that keeps adults with disabilities locked away from the community at large.
The NCSA noted that the steady closure of ICFs and sheltered workshops around the country in recent years “has already had the devastating impact of depriving individuals of critical options.”
- The bill would only support “supported (integrated or community-based) employment and integrated day services.”
According to the NCSA, the bill “could shutter desperately needed programs serving the severely disabled who are incapable of participating in integrated day services owing to their severe cognitive, behavioral, medical and functional challenges.”
We have been raising these same concerns about the closures of ICFs and sheltered workshops in Massachusetts for many years.
- The bill overlooks the difficulty of finding housing in the community for persons with autism, and the possibility of eviction for those with dangerous or disruptive behaviors.
We have also noted the potential for isolation of community-based group home residents whose guardians are perceived as troublesome or meddlesome
- The bill would establish an “advisory committee” that would place veto power in the hands of a few advocates. The NCSA stated that “a small, unelected and unaccountable committee would be handed broad discretion to determine what qualifies as HCB services across the country, trumping whatever needs and preferences of severely disabled individuals,”
As we noted about the Disability Integration Act, this new legislation does not comply with the choice provision in the Olmstead v. L.C. U.S. Supreme Court case. In 1999, the late Justice Ruth Bader Ginsburg, who wrote the majority opinion in Olmstead, endorsed the idea of a continuum of care for the most vulnerable members of our society. Her decision and message were models of inclusivity.
We urge people to email the Senate Special Committee on Aging, as we plan to do, at HCBSComments@aging.senate.gov. Feel free either to paste in this blog post or forward a link to it, along with a short message in opposition to the HCBS Access Act as currently written.
Fernald may be closed, but it’s still being blamed for the ills of the DDS system
The Fernald Developmental Center in Waltham has been closed for some seven years.
But activists who oppose all forms of congregate care are still making the former facility a focus of blame for the failures of the state’s care for people with developmental disabilities, even if it means portraying only one side of Fernald’s history.
It appears the latest effort to denigrate Fernald is a scheduled Zoom panel discussion being sponsored on March 10 by the Harvard Law School.
The discussion, titled “Fernald’s Legacy,” will feature Alex Green, a leader of a protest of a holiday light show late last year on the Fernald campus. Green started a petition last fall to stop the light show, contending a festive show on the campus would be “inappropriate, given (Fernald’s) history of human rights abuses and experimentation on children.”
A promotional text for the upcoming Harvard panel discussion refers to the legacy of institutions such as Fernald as “lurid,” and states that society must “critically and publicly interrogate the role they played in shaping today’s services, systems, and attitudes for persons with disabilities.” (my emphasis)
But dismissing the entire legacy and history of Fernald and similar facilities in Massachusetts as lurid may in fact be failing to “critically interrogate” their role.
Fernald was not the same institution by 1993 that it had been in 1970
Fernald’s past is, of course, notorious and controversial. Until the early 1980s, Fernald and other similar state-run centers were indeed horrendous warehouses of abuse and neglect.
In fact, many of COFAR’s members were plaintiffs in Ricci v. Okin, a combined class-action lawsuit first brought in the early 1970s by the late activist Benjamin Ricci over the conditions at the Belchertown State School. The Ricci lawsuit resulted in a consent decree that included the then Belchertown, Fernald, Wrentham, Dever, Monson, and Templeton state schools.
It was due to the dedication of the late U.S. District Court Judge Joseph L. Tauro in overseeing the consent decree that conditions at Fernald and the other state schools finally began to change.
What Green and other activists fail to understand or acknowledge is the revolutionary change that occurred at Fernald and the other institutions as a result of the litigation and Judge Tauro’s intervention. But acknowledging that change would be inconvenient if their purpose is to portray all congregate care, even as it exists today, as uniformly bad.
We have encountered this one-sided viewpoint repeatedly over the years among advocates, politicians, public administrators, and journalists.
That viewpoint betrays a lack of understanding of the history of care of the disabled in Massachusetts and elsewhere around the country. It also shows a lack of understanding of the strict federal standards under Title XIX of the Social Security Act that state-run developmental centers, also known today as Intermediate Care Facilities (ICFs), must meet.
Acknowledging the change that occurred at Fernald is also inconvenient for corporate group home providers to the Department of Developmental Services (DDS) and their lobbyists such as the Arc of Massachusetts. Since Fiscal 2014, when Fernald was closed, the DDS provider residential line item in the Massachusetts budget has risen by $354 million, or 37%, when adjusted for inflation.
That may explain why the Arc signed on to Green’s petition to stop the light show at Fernald, and why the Arc continues to lobby in favor of further closures of congregate-care facilities and further privatization of DDS services.
Our request to be on the Harvard Law School panel was not accepted
On Monday (March 1), I sent a detailed email to Green and to William P. Alford, chair, and Michael Stein, executive director of the Harvard Law School Project on Disability, which is hosting the panel discussion. In the email, I tried to present a balanced view of Fernald’s legacy, and suggested that the panel include at least one person who is aware of Fernald’s full history and understands its real meaning and importance. Tom Frain, our Board president, was willing to fulfill that role on the panel.
Yesterday, I received a 3-sentence response from Professor Stein, saying only that the event is open to the public and that we should “be respectful of the views expressed by our panelists.” He didn’t accept our offer to serve on the panel. Presumably, the most we would be allowed to do is participate in a question-and-answer session at the end of the discussion. As a result, we will pass on attending what is likely to be a one-sided event.
Stein’s email to me did not acknowledge, much less respond to any of the points I had raised about Fernald’s legacy.
The following are the points I made in my original email to Stein, Alford, and Green:
Judge Tauro attested to the improvements at Fernald
Judge Tauro, who died in November 2018 at the age of 87, had visited Fernald, Belchertown and the other Massachusetts facilities in the early 1970s to observe the conditions first hand. He noted two decades later in his 1993 disengagement order from the consent decree that the legal process had resulted in major capital and staffing improvements to the facilities and a program of community placements.
Those improvements and placements, Judge Tauro wrote, had “taken people with mental retardation from the snake pit, human warehouse environment of two decades ago, to the point where Massachusetts now has a system of care and habilitation that is probably second to none anywhere in the world.”
It is unfortunate that in a media release that Green wrote in November about the protest of the planned light show at Fernald, he appears to have selectively used only the “snake pit” portion of Judge Tauro’s statement in referring to Fernald and the other facilities. That, of course, reversed the meaning of Tauro’s disengagement statement.
Deinstitutionalization has not been a uniform success
Judge Tauro believed in the importance of a continuum of care for people with intellectual and developmental disabilities (I/DD), and knew that institutions such as Fernald had an important role to play in it. In his 1993 disengagement order, he maintained that facilities such as Fernald should not be closed unless it was certified that each resident would receive equal or better care elsewhere.
As the years went on, the promise of equal or better care in the community was not realized. Deinstitutionalization has turned out to be fraught with problems for people with I/DD just as it has for people with mental illness. Between 2000 and 2014, the VOR, our national affiliate, catalogued hundreds of cases of abuse and neglect in privatized group homes around the country.
In testimony in 2018 to a legislative committee, Nancy Alterio, executive director of the Massachusetts Disabled Persons Protection Commission (DPPC), stated that abuse and neglect of persons in the Department of Developmental Services (DDS) system had increased 30 percent in the previous five years, and had reached epidemic proportions.
Alterio’s testimony came long after the State of Massachusetts had begun to rely primarily on privatized, community-based group homes for residential care of persons with I/DD, and long after the state had phased out and closed all but two state-run ICFs comparable to Fernald.
Our own analysis of more than 14,000 allegations of abuse made to the DPPC showed that the rates of substantiated abuse and neglect per client in those two remaining ICFs — the Wrentham Developmental Center and the Hogan Regional Center — were practically zero between Fiscal 2010 and 2019.
Yet many advocates for corporate providers, such as the Arc of Massachusetts, have pushed for decades for complete deinstitutionalization and for additional privatization of services for people with I/DD. They have been joined by administrations at the state and national levels, which have continually made state-run care and services targets for closure and outsourcing to contracted providers.
Since 2009, the U.S. Justice Department has filed, joined, or participated in lawsuits around the country to close ICFs regardless of whether the residents or their families or guardians wanted to close the facilities they were living in or not.
Fernald’s opponents have misinterpreted the landmark Olmstead v. L.C. Supreme Court decision
Those advocates of deinstitutionalization and privatization have consistently misinterpreted the 1999 Olmstead v. L.C. U.S. Supreme Court decision, which held that institutional care is appropriate for those who desire it and whose clinicians recommend it.
The late Justice Ruth Bader Ginsburg wrote the majority opinion in Olmstead, which has been characterized as holding only that unjustified isolation in institutions is “discrimination based on disability.” But that statement is only half the holding of Olmstead.
There was another major element of Justice Ginsburg’s Olmstead decision that has continued to be disregarded by many who have then gone on to mischaracterize the decision as advocating or requiring the end of institutional care. It didn’t. As the VOR has pointed out, Justice Ginsburg wrote a balanced decision that “supports both the right to an inclusive environment and the right to institutional care, based on the need and desires of the individual.”
Justice Ginsburg’s majority opinion held that:
We emphasize that nothing in the ADA or its implementing regulations condones termination of institutional settings for persons unable to handle or benefit from community settings. . . Nor is there any federal requirement that community-based treatment be imposed on patients who do not desire it.
As Justice Ginsburg stated, community-based care is an appropriate option for those who desire it, whose clinicians support it, and in cases in which states have the resources to reasonably support care in the community system. Unless all three of those conditions hold, institutional care may well be the appropriate setting.
Fernald’s families fought the closure of Fernald from 2003 through 2014
In 2004, the plaintiffs in original Ricci v. Okin consent decree litigation asked Judge Tauro to reopen the case, arguing that the then Romney administration was illegally trying to close Fernald, and was thereby violating the terms of Tauro’s disengagement order. Those plaintiffs included families and guardians of Fernald residents, and members of COFAR and other advocacy organizations.
In February 2006, Tauro appointed then U.S. Attorney Michael Sullivan as Court Monitor in the case and asked Sullivan to review the transfers of 49 residents from Fernald since 2003. Sullivan ultimately recommended to the newly installed Patrick administration that Fernald remain open.
In making the recommendation, Sullivan maintained in his report to Tauro that while the level of care there might be able to be duplicated elsewhere, the loss of familiar surroundings and people “could have devastating effects [on the residents] that unravel years of positive, nonabusive behavior.”
Tauro subsequently ruled that the families at Fernald must be given the option of remaining there. But the Patrick administration ignored Sullivan’s recommendation and appealed Tauro’s ruling to the U.S. First Circuit Court of Appeals. The Circuit Court of Appeals overruled Tauro, without giving deference to his expertise in the case; and the Patrick administration proceeded to phase down and close Fernald and later three other ICFs of the six remaining in the state.
By 2014, the year Fernald was closed, some 14 families were still fighting legal and administrative battles to keep the facility open for their loved ones because they believed the care there was better than in the community-based system.
Those families came in for relentless media criticism and blame from lobbyists for corporate providers, who were seeking to close Fernald and the remaining state-run centers, and to garner the lucrative state contracts that would result from it.
The incestuous nature of the privatized system
The closures of ICFs around the country and the rise of the privatized system of care have provided enormous financial windfalls for politically connected corporate contractors. Their executives have garnered huge increases in their personal compensation, but have frequently neglected to pass through the ever higher levels of state funding to direct-care workers. That is one of the reasons for the epidemic of abuse and neglect in the corporate provider-based system of care.
In 2015, we calculated that more than 600 executives employed by corporate human service providers in Massachusetts received some $100 million per year in salaries and other compensation. By our calculations, state taxpayers were on the hook each year for up to $85 million of that total compensation.
As noted, the line item in the Massachusetts state budget for DDS-funded residential providers has been boosted by hundreds of millions of dollars since Fernald’s closure. Yet, as Massachusetts State Auditor Suzanne Bump’s office reported in 2019, while that boost in state funding resulted in surplus revenues for the providers, those additional revenues led to only minimal increases in wages for direct-care workers.
Administrations mistakenly believe closing ICFs will save money
Much of the justification for, and reasoning behind, closing developmental centers has been based on the fact that providers pay lower wages than do public agencies to direct-care workers. Successive administrations in Massachusetts have also sought to operate the ICFs as inefficiently as possible in order to make them appear as expensive as possible, thereby justifying their closure.
In 2014, the Fernald Working Group, a coalition of local organizations, had recommended a cost-effective approach to care in that setting. Their proposal was that the Fernald Center be downsized and converted to group homes on a portion of the campus while the remainder of the campus was opened to development, open space, and other uses. Similar proposals had been made over the years by the former Fernald League and COFAR.
But the then Romney and subsequent Patrick administrations were interested only in one thing — closing Fernald and three other ICFs in the state, contending the state would save tens of millions of dollars a year in doing so. They never considered any of the proposed alternatives to the closures.
That there isn’t necessarily a long-term fiscal savings in transferring people from developmental centers to decentralized, provider-based care has been acknowledged even by one of the leading proponents of deinstitutionalization in the Obama administration.
In a law journal article, Samuel Bagenstos, a former top litigator in the Justice Department’s Civil Rights Division, acknowledged that any cost savings in closing developmental centers “will shrink as people in the community receive more services.”
He added that a significant part of the cost difference between institutional and provider-based care “reflects differences in the wages paid to workers in institutional and community settings — differences…that states will face increasing pressures to narrow.”
Today, as noted, two ICFs remain in Massachusetts – the Wrentham Developmental Center (WDC) and the Hogan Regional Center in Danvers. We rarely, if ever, hear that families or guardians are unsatisfied with the care there.
Mary Ann Ulevich, a COFAR member and a member of the Wrentham Board of Trustees and of the Wrentham Family Association, wrote to DDS Commissioner Jane Ryder in November 2019 in praise of the care her cousin, Tom Doherty, had received at WDC. Tom had died on October 24 at the age of 68. Ms. Ulevich wrote:
I just want you to know how proud you can be of the work carried out at WDC. I know that the philosophy of care for those with intellectual disability is to provide support to remain in their community with their families, with guidance and services. I fully support this contemporary approach, but acknowledge that there are many who because of their history and challenges, and/or because of the progression of their needs combined with diminished family and community resources, can and do thrive in facility-based care.
Here are additional accounts of the value that families put today on the care at WDC.
Apparently, if we keep blaming Fernald and other congregate-care facilities for all of the dysfunctionality of the DDS system, we will not have to admit that the problems with abuse and neglect and financial mismanagement in the system primarily lie elsewhere.
Setting the record straight about Ruth Bader Ginsburg’s historic contribution to the rights of the disabled
As the nation celebrates the life and judicial legacy of the late U.S. Supreme Court Justice Ruth Bader Ginsburg, we would like to recognize and set the record straight about her major contribution in one particularly vital case to the rights of persons with cognitive disabilities.
Ginsburg wrote the majority opinion in Olmstead v. L.C., which has been characterized as the most important civil rights decision for people with disabilities in our country’s history. It may have certainly been that, but not, as is usually claimed, because it held that “unjustified isolation (in institutions) is properly regarded as discrimination based on disability.”
That statement is only half the holding of Olmstead. There was another major element of Ginsburg’s Olmstead decision that has continued to be disregarded by many who have then gone on to mischaracterize the decision as advocating or requiring the end of institutional care. It didn’t.
As our national affiliate, the VOR, has pointed out, Ginsburg wrote a balanced decision that “supports both the right to an inclusive environment and the right to institutional care, based on the need and desires of the individual.”
In other words, the greatness of Ginsburg’s contribution to the rights of the disabled was that her decision was all about choice. It provides a choice between community-based care and institutional care to persons with cognitive disabilities.
In announcing the Olmstead decision on June 22, 1999, Ginsburg stated that that the answer was “a qualified yes” to the question whether the Americans with Disabilities Act (ADA) “…may sometimes require a state to place persons with mental disabilities in community settings rather than in state institutions.”
The key word here was “qualified.” Ginsburg’s majority opinion held:
We emphasize that nothing in the ADA or its implementing regulations condones termination of institutional settings for persons unable to handle or benefit from community settings. . . Nor is there any federal requirement that community-based treatment be imposed on patients who do not desire it.
As Ginsburg stated, community-based care is an appropriate option for those who desire it, whose clinicians support it, and in cases in which states have the resources to reasonably support care in the community system. Unless all three of those conditions hold, institutional care may well be the appropriate setting.
The majority decision included a reference to amicus brief submitted by VOR, which stated that:
Each disabled person is entitled to treatment in the most integrated setting possible for that person – recognizing that, on a case-by-case basis, that setting may be in an institution.
Decision has been misinterpreted
Despite those clear statements, Olmstead has continuously been misinterpreted by policy makers, administrators, and even governmental agencies as requiring the closure of all remaining state-run congregate care facilities in the country and privatizing all remaining residential care. What these advocates have done is to take the choice out of it.
The U.S. Department of Justice’s Civil Rights Division, for instance, has mistitled its technical assistance website, “Olmstead: Community Integration for Everyone.” (my emphasis). That is simply not true. Olmstead clearly implied that community integration isn’t for everyone.
In line with this misinterpretation, the DoJ has for years filed lawsuits around the country to close state-run care facilities, whether the residents and their families and guardians have opposed those closures or not. This has caused “human harm, including death and financial and emotional hardship,” according to information compiled by VOR.
While the DoJ has not filed such a suit against the State of Massachusetts, that may be because the state closed four out of six developmental centers that were in operation in the state as of 2014. Olmstead, however, has been used as a justification in Massachusetts and other states for closing sheltered workshops, as Massachusetts did as of 2016 over the objections of many of the participants and their families.
Those acts and outcomes are not consistent with the plain language of Olmstead regarding the importance of the individual’s personal choice. Nevertheless, facility closure advocates consistently cite Olmstead as justifying their actions.
Community-based care was appropriate for original plaintiffs
The Olmstead lawsuit was brought on behalf of Lois Curtis and Elaine Wilson of Georgia, who both had diagnoses of mental health conditions and intellectual disabilities, according to a website created by attorneys with the Atlanta Legal Aid Society, who represented the women in the case.
Curtis and Wilson had asked the state of Georgia to help them get treatment in the community so that they would not have to live in a mental hospital. According to the Atlanta attorneys, the doctors who treated Curtis and Wilson agreed that they were capable of living in the community with appropriate supports. However, both women had been waiting for years for their community-based supports to be established.
Thus, the original plaintiffs in the Olmstead case satisfied at least two of the three conditions that Ginsburg set for community-based care in the decision: their clinicians deemed community-based care appropriate for them, and they desired it. But Ginsburg recognized that might not be true of everyone in institutional care.
Olmstead wrongly used to justify continuing privatization of DDS services
The Olmstead decision is based on regulations in the ADA that stipulate that public entities should provide services and programs in “the most integrated setting appropriate to the needs” of persons with disabilities.
In Massachusetts, administrations have long contended that the most integrated settings exist in the form of community-based group homes, the majority of which are run by corporate providers that receive state funding.
The problem with this view is that there have been countless examples of group homes that offer residents little opportunity for community integration. Yet the argument that group homes are more integrated than developmental centers is ingrained among policy makers, journalists, and others. This has made it accepted wisdom that all state-run congregate care facilities should be closed — an outcome that will ultimately lead to complete privatization of care.
That appears to be the goal of federal agencies such as the Centers for Medicare and Medicaid Services (CMS), which has issued regulations and provided billions of dollars in grants intended to boost the privatized group home system around the country.
On September 23, for instance, CMS announced the availability of up to $165 million in supplemental funding to states currently operating Money Follows the Person (MFP) demonstration programs. As a CMS press release put it, this funding “will help state Medicaid programs jump-start efforts to transition individuals with disabilities and older adults from institutions and nursing facilities to home and community-based settings of their choosing.”
But while this outcome is termed a choice, the closure of the institutions will actually eliminate the choice that Ginsburg articulated in Olmstead. The VOR amicus brief, as noted, stated that on a case-by-case basis, the most integrated setting may be an institution.
The Disability Integration Act of 2019 would further erode Olmstead choice
Unfortunately, the notion that community-based care is the only appropriate option for people with cognitive disabilities is so ingrained and pervasive that the entire Massachusetts congressional delegation signed onto a bill last year, which would encourage further unchecked privatization of human services, diminished oversight, and reduced standards of care across the country.
The bill, known as the federal Disability Integration Act of 2019 (HR.555 and S.117), would potentially threaten the Wrentham Developmental and Hogan Regional centers in Massachusetts, the state’s only two remaining residential facilities for the developmentally disabled that meet federal Intermediate Care Facility (ICF) standards.
The legislation calls explicitly for the the “transition of individuals with all types of disabilities at all ages out of institutions and into the most integrated setting…” (emphasis added). As such, the bill does not comply with the choice provision in Olmstead.
We have contacted the members of the members of the state’s congressional delegation to urge them to support a change in the language of the bill to respect the choice of individuals, families, and guardians either to get into or to remain in congregate care facilities.
Given that the two versions noted above of this bill are still pending in House and Senate committees in Congress, we plan to remind the members of the Massachusetts delegation of the legacy and words of Ruth Bader Ginsburg.
In 1999, Justice Ginsburg endorsed the idea of a continuum of care for the most vulnerable members of our society. Her decision and message were models of inclusivity. Now at the time of her passing, we think it is important to remember and reflect on that.
Direct care workers need more than an official state day and billboards in their honor
Governor Baker and an employee union recently honored home care workers in Massachusetts with an official state day and billboards.
But we think those workers might appreciate better pay and health benefits even more.
Baker and the 1199SEIU health care worker union teamed up to declare “Home Care Day” on September 4. The SEIU also funded the placement of 13 billboards in Boston, Worcester, Springfield, and other cities to highlight minority home care workers.
Tim Foley, vice president of 1199SEIU, told the State House News Service he hoped the billboards will “let home care workers know they are valued by so many families across the commonwealth and push elected leaders to invest in the workforce.”
We agree that the governor and Legislature need to do more to narrow the enormous gap that exists between the wages of direct-care workers and the executive salaries of the primarily private providers that employ them.
In 2018, Baker did sign legislation to raise the minimum wage of direct-care and other workers to $15 an hour; but it won’t reach that amount until 2023. In 2017, the Legislature rejected efforts to raise direct-care wages to $15 as of that year, and rejected a bid last year to raise direct care wages to $20 per hour.
A bill (H.4171) that would similarly raise hourly direct care wages to $20 has been stuck in the Health Care Financing Committee since last November.
Yet, it’s not as if the governor and Legislature are reluctant to provide continually rising levels of funding to the providers themselves. It’s just that the provider executives have chosen not to pass much of that increase through to the direct-care workers. Instead, they have greatly boosted their own personal wealth.
We reported in 2012 that direct-care workers working for corporate providers contracting with the Department of Developmental Services (DDS) had seen their wages stagnate and even decline in previous years while the executives running the corporate agencies were getting double-digit increases in their compensation.
Since 2012, the line item in the state budget for DDS-funded residential providers has increased by nearly 45 percent in inflation-adjusted terms, to over $1.5 billion in Fiscal 2020. That is according to the Massachusetts Budget and Policy Center’s online Budget Browser.
Yet, as State Auditor Suzanne Bump’s office reported last year, while that boost in state funding resulted in surplus revenues for the providers, those additional revenues led to only minimal increases in wages for direct-care workers.
Bump’s May 8, 2019 audit found that the average hourly direct-care wage was $11.92 in Fiscal 2010, and rose only to $14.76 as of Fiscal 2017. That’s an increase of only 24 percent over that eight-year period, an amount that only barely exceeded the yearly inflation rate.
Meanwhile, according to the audit, the increased state funding to the providers enabled them to amass a 237 percent increase in surplus operating revenues (total operating revenues over total operating expenses) during that same eight-year period. The increased state funding was at least partly intended to boost direct-care wages, but it “likely did not have any material effect on improving the financial well-being of these direct-care workers,” Bump’s audit stated.
In 2017, SEIU Local 509 in Massachusetts issued a report similarly asserting that increases in funding to human services providers enabled the providers to earn $51 million in surplus revenues. The union contended that the providers could and should have used the surplus revenues to boost direct-care wages.
Confirming our 2012 findings, the SEIU’s 2017 report stated that during the previous six years, the providers it surveyed paid out a total of $2.4 million in CEO raises. The SEIU report concluded that:
This all suggests that the amount of state funding is not at issue in the failure to pay a living wage to direct care staff, but rather, that the root of the problem is the manner in which the providers have chosen to spend their increased revenues absent specific conditions attached to the funding. (my emphasis)
So, as noted, it isn’t a matter of the providers not having the money. The governor and Legislature need to pass a bill such as H.4171, which would require providers to use up to 75 percent of their total state funding to boost direct-care worker salaries to at least $20 per hour.
In other words, if state-funded providers aren’t willing to pay a living wage to the workers they employ, then it’s time for the state to step in and require them to do so. If that were to happen, Governor Baker would have put some substance behind a declaration of a Direct-Care Worker Day in Massachusetts.
Why the media won’t cover issues of concern to people with developmental disabilities
Whether it’s due to “cancel culture” or a misguided ideology that the largely privatized system of care in society is functioning perfectly for people with intellectual and other developmental disabilities, the mainstream media these days just don’t seem interested in reporting about the system.
For a while now, we’ve been debating why it is so difficult to get media coverage in Massachusetts, in particular, of issues of concern to this group of people and their families and guardians.
A letter sent to the New York Times may provide one answer. In the August 20 letter, 75 organizations and leaders in the disability community critique that newspaper’s apparent lack of interest in covering “serious issues facing those with significant intellectual and developmental disabilities.”
The Times has apparently not yet published the letter, which is sponsored by the nonprofit National Council on Severe Autism (NCSA).
The letter points out that the Times, while recently honoring the 30th anniversary of the signing of the Americans with Disabilities Act (ADA), failed to include virtually any mention of persons with intellectual or other developmental disabilities. Yet the paper published over two dozen articles over the past few weeks about people with a wide range of other, non-cognitive disabilities.
As the NCSA’s letter to the Times notes, “the full story” in honoring the ADA would include those people with profound intellectual and developmental disabilities. But in doing so, the Times would have to acknowledge that this group of people do not have “the autonomous decision-making, independent living, and competitive, minimum-wage employment that are the cornerstones of the Disability Rights movement.”
The letter ties the Times’ disregard of the developmentally disabled to “cancel culture.” The letter states:
It is ironic that the Times has excluded the most disabled from its ADA coverage exactly as a debate about “cancel culture” has embroiled this newspaper and others. Severe intellectual and developmental disability should be a bipartisan issue — we, the undersigned, represent the broad range of the political spectrum. But because our stories don’t fit the progressive left’s disability narrative, they have been effectively cancelled — exactly by those who claim to care most about this vulnerable population.
We think the disregard of the developmentally disabled is evident in the mainstream media as a whole. The media buy into an ideology promoted by much of the disability advocacy community that no one, no matter how low their measured cognitive functioning may be, has limits on what they can achieve in the community system.
The problem is that this is an absurd position, and it leads to basic contradictions between the ideology and reality. People with intellectual disabilities do have limits on their ability to function in society. Rather than confront that contradiction, the media appear to have chosen to ignore people with cognitive disabilities altogether.
When we raise issues about the need for institutional care or sheltered workshops for those with intellectual disabilities, the media in Massachusetts don’t want to hear about it. It doesn’t fit the narrative that there is no one who is incapable of functioning perfectly in the community and working in mainstream jobs.
We recently reported that the Baker administration discussed reducing public reporting of data on testing of individuals and staff in DDS-funded group homes for COVID-19. Although we tried to bring our concerns over that issue to the attention of the mainstream media in Massachusetts, no media outlet has run any articles about it.
With only the occasional exception, the mainstream media in Massachusetts do no more than scattershot reporting even on the tragic and ongoing problem of abuse and neglect in the DDS system.
Community-first ideology pushed by successive administrations and corporate providers
Perhaps not coincidentally, the ideological position that the community system of care is working perfectly for everyone fits with a decades-long push by successive administrations in Massachusetts and corporate providers for more privatization of the DDS system. According to the ideology, clients in privatized, community-based residences are completely integrated with their communities and can reach their full potential there, unlimited by institutional constraints.
But while the community-based system has meant more state-funded contracts for providers and skyrocketing pay for its corporate executives, the system has largely failed to integrate its clients, and is beset by a bottom-line mentality that provides low pay, training, and supervision of direct-care staff.
Systematic reporting on inadequacies in care in the privatized system, or on a lack of adequate testing in that system for COVID-19, is not desired by corporate, state-funded providers.
Absurd position that autism is “perfect”
The letter to the Times pointedly criticizes an essay that the newspaper published in July that illustrates the ideology driving media coverage today. The essay by writer Madeleine Ryan, the mother of an autistic child, is titled “Dear Parents: Your Child with Autism is Perfect.”
In it, Ryan stated, “Your child might be verbal, nonverbal, aggressive, passive, introverted or extroverted. It doesn’t matter.” She added, “Your child is perfect. Be skeptical of what doctors, teachers, family members or friends say to the contrary.”
The letter to the Times includes a response to Ryan’s piece by Amy Lutz, founding board member of the NCSA and parent of a severely autistic son:
[Jonah] will never go to college, hold a job, see the world, or have a romantic relationship. He will always require round-the-clock supervision, because he has no safety awareness: he doesn’t look before crossing the street, despite years of instruction; and in one terrifying moment, he tried to jump off a cruise ship because he wanted to swim in the ocean… Jonah’s experience is just as important…and must not be elided from the narrative in favor of some kind of fantasy autism nirvana.
The letter further quotes Lee Elizabeth Wachtel, Medical Director of the Neurobehavioral Unit at the Kennedy Krieger Institute and an Associate Professor of Psychiatry at the Johns Hopkins School of Medicine:
When an autistic child has permanently blinded himself from self-injury, broken his teacher’s arm, or swallowed multiple toothbrushes and required emergency surgery, there is nothing perfect or magnificent about it, and it must be remedied.
Warning in the Olmstead decision
The letter to the Times notes a warning by Justice Anthony Kennedy in the Olmstead v. L.C. U.S. Supreme Court decision, which cleared the way for expanded privatization of care of the developmentally disabled. In a concurring opinion to the Olmstead decision, Kennedy wrote that:
It would be unreasonable, it would be a tragic event, then, were the (ADA) to be interpreted so that States had some incentive…to drive those in need of medical care and treatment out of appropriate (institutional) care and into settings with too little assistance and supervision.
Unfortunately, that is exactly what the ADA and the Olmstead decision itself have been interpreted by the media and many advocates as allowing.
Both the ADA and Olmstead are being used as covers for the real attitude toward the developmentally disabled on the part of the media and so many others in positions of power — they just don’t care.
